Download presentation
Presentation is loading. Please wait.

1
IN THE NAME OF GOD

2
PREGESTATIONAL DM

3
WHITE CLASSIFICATION OF DM DURING PREGNANCY Gestational DM Class A : diet alone,any duration or age Class B : age at onset > 20 y& duration < 10y Class C : age at onset 10- 19 or duration 10 – 19 y Class D : age 20 y or background retinopathy or HTN ( not preeclampsia) Class R : proliferative retinopathy or vitreous HE Class F : nephropathy with p. uria > 500 mg Class RF : R & F Class H : heart dx Class T : prior renal transplantation Joslin textbook 2005 joslins textbook 2005

4
Evaluation of diabetic women Risk assessment Preconception counseling

7
Risk assessment

8
Nephropathy During pregnancy, complicated by nephropathy, GFR & albuminuria increase &also increase in mean BP, it may worsen preexisting nephropathy. Women with class F diabetes demonstrate that a majority of these pts develop proteinuria in the nephrotic range by the third trimester but Creatinine is nl joslins textbook 2005

9
Mild nephropathy don`t complicated Moderate to severe nephropathy with GFR < 90 ml/min & proteinura more than 1 g /24 hrs have a more rapid decline in GFR joslins textbook 2005

10
Retinopathy Risk of progression of retinopathy increase in pregnancy Risk is influenced with : severity of baseline retinopathy HbA1C > 8.5% at the first prenatal visit intensively treated pt has 1.6 fold increase risk of retinopathy Conventionally treated pt has 2.4 fold increase in retinopathy In DCCT study,no difference in level of retinopathy in pt who became pregnant as compared with pt who never p. joslins textbook 2005

11
hypoglycemia Most severe in first half of pregnancy : more insulin sensitivity, morning sickness, strict BS control Severe hypoglycemia isnot teratogenic in human Treat with 15 g carbohydrate & then rechecked BS after 15 min & additional 15 g carbohydrate use It is Better use lispro( FDA safety rating of B ) and for aspart FDA safety rating of C joslins textbook 2005
 and for aspart FDA safety rating of C joslins textbook 2005")
12
Hypertensive disorder Chronic HTN: before or up to 20 th weeks of gestation & if HTN continue after 12 week after pregnancy Preeclampsia-eclampsia : ≥ 140/90 mmhg,usually after 20 th weeks of gestation with proteinuria more than 300mg/24 hrs Preeclampsia-eclampsia superimposed on chronic HTN Gestational HTN joslins textbook 2005

13
Start treatment from BP ≥ 130/ 80 mmHg especially if microalbuminuria or proteinuria is present

14
Management of diabetes in pregnancy

15
Preconception counseling Education Maternal risk assessment Fetal risk assessment HbA1C levels should be normal Uptodate 2006

16
Maternal risk assessment HX & P/E Review of complication Current & past glucose management Comorbid medical conditions Gynecologic & obstetric hx Discontinue oral anti-hyperglycemic agent Daily folic acid : 1 mg prior conception & continue after conception Self management skills should be reviewed Nutrition counseling Mental health professional should be available Uptodate 2006

17
Control of HTN : BP < 130/80 Thyroid dx : TSH, FT4 Neuropathy ( peripheral & autonomic ) vascular evaluation of lower extremities Infection : UTI SMBG HbA1C Discontinue alcohol & smoking Uptodate 2006
 vascular evaluation of lower extremities Infection : UTI SMBG HbA1C Discontinue alcohol & smoking Uptodate 2006")
18
Ophthalmic assessment Comprehensive eye examinatin in pt with planing for pregnancy f/u through pregnancy at least every 3 months & also one y after pregnancy Tight glycemic control may accelerate retinopathy & need more attention by ophthalmologist Laser photocoagulation for severe preproliferative diabetic retinopathy

19
Assessment of renal function Spot urine for microalbumin /cr or time collection for 24 hrs Serum cr Cr> 2mg/dl & GFR < 50 ml/min. & proteinuria more than 2 gr /day can be considered relative contraindications to pregnancy

20
Cardiac evaluation As the same as non pregnant women.( uptodate 2006) Symptomatic CHF & Ischemic heart disease are contraindicated to pregnancy. ( davidson 2004)
.")
21
MANAGMENT of HTN & /OR MICROALBUMINURIA Methyl dopa Hydralazine B-blocker Ca canal blocker ACE inhibitor is contraindicated Thiazid is relatively contraindicated BP should be managed aggressively Hold BP< 130 /80 mmHg Uptodate 2006

22
Management of hyperlipidemia Statins are contraindicated & should be discontinued before conception Hypertriglyceridemia treat with diet, supplementation with medium chain TG Joslin text book 2005

23
Preconception treatment goal Plasma FBS: 80-110 2hpp : 100-155 HbA1C : < 7% Avoid hypoglycemia Joslin text book 2005

24
goals for glycemic control for women with GDM, ( Fourth International recommendations from the Workshop-Conference on Gestational Diabetes) suggest: capillary blood glucose concentrations should be : FBS: 95 mg/dl BS-1hpp :140 mg/dl and/or BS-2hpp: 120 mg/dl ADA 2006
 suggest: capillary blood glucose concentrations should be : FBS: 95 mg/dl BS-1hpp :140 mg/dl and/or BS-2hpp: 120 mg/dl ADA 2006")
25
First trimester Same as preconception counseling care Evaluate risk factors Uptodate 2006

26
Second trimester Visit the pt every 2 to 4 weeks or more if pt has complications or glycemic control is suboptimal. Maternal analyte screening : screening for Dawn SX or neural tube defects ( α fetoprotein,unconjucated estriol,HCG,inhibin A ) Sonography : at 18 weeks of gestation Uptodate 2006
 Sonography : at 18 weeks of gestation Uptodate")
27
Third trimester Visit for every 1 to 2 weeks untile 32 wks of gestation & then weekly Glycemic control Sonography Estimation of fetal size Surveillance for pregnancy complication Fetal surveillance : weekly NST at 32 weeks with suboptimal HbA1C & from 35 weeks with nl HbA1C Assess for macrosomia,premature labor, hydramnious Uptodate 2006

28
Davidsons DM 2004

29
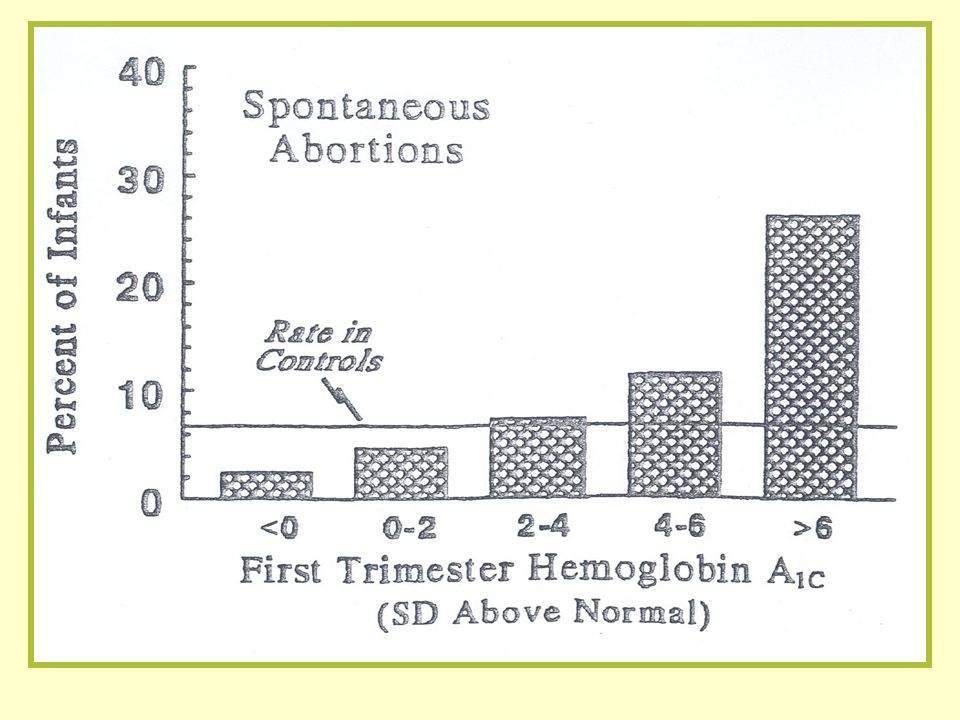
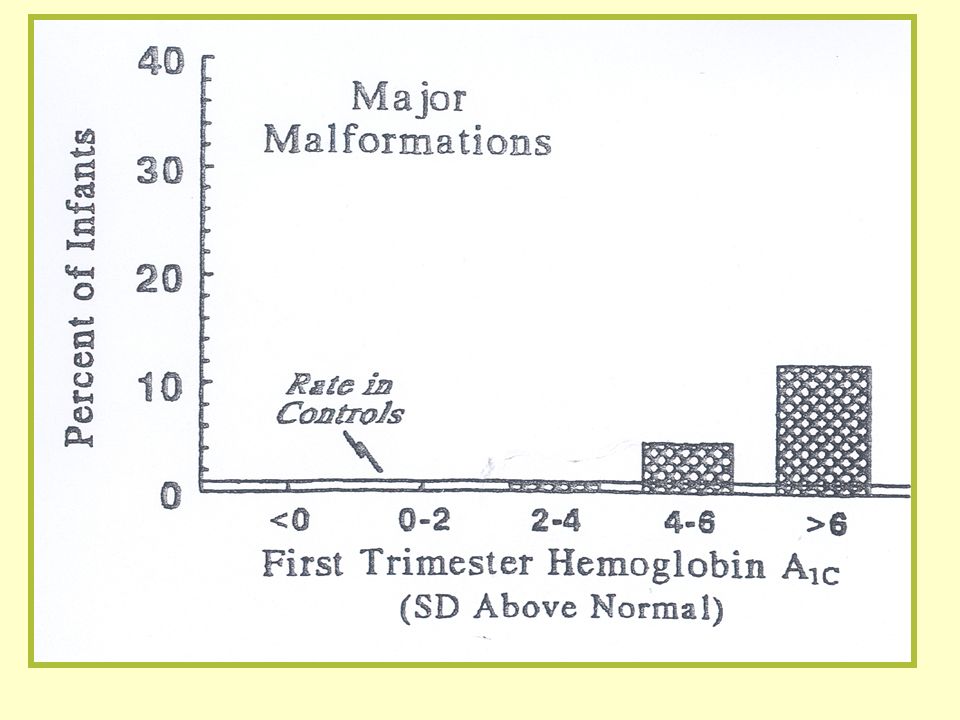
Fetal risk Congenital malformation & spontaneous abortion : incidence is 5% -9% when occurs in blastogenesis ( first 4 weeks of conception ) is more severe than organogenesis ( weeks 4-5 after conception ) HbA1C < 8.5 % 3.4% HbA1C > 8.5 % 22.4% Uptodate 2006
 is more severe than organogenesis ( weeks 4-5 after conception ) HbA1C < 8.5 % 3.4% HbA1C > 8.5 % 22.4% Uptodate 2006")
31
Congenital m

33
Thanks for your attention

Similar presentations