Download presentation
Presentation is loading. Please wait.

1
Christina Davey Regional Epidemiologist Serving Lawrence, Pike, Ross, and Scioto Counties Tick-borne Diseases in Ohio

2
Overview Rocky Mountain Spotted Fever Lyme Disease Ehrlichiosis/Anaplasmosis Tick Submission

3
Rocky Mountain Spotted Fever (RMSF) Agent/transmission Rickettsia rickettsii Maintained and amplified by hard ticks, primarily American dog tick (D. variabilis) and Rocky Mountain wood tick (D. andersoni). Brown dog tick (Rhipicephalus sanguineus) and Cayenne tick (Amblyomma cajennense) also been implicated as vectors.
 and Rocky Mountain wood tick (D. andersoni). Brown dog tick (Rhipicephalus sanguineus) and Cayenne tick (Amblyomma cajennense) also been implicated as vectors..")
4
Rocky Mountain Spotted Fever (RMSF) Agent/transmission (Continued) In Ohio, the American dog tick (Dermacentor variabilis) is the vector. Humans contract RMSF through the bite of dog tick, or by coming in contact with tick secretions or body fluids through careless handling of ticks. Dogs can transport ticks into the household environment and may also become ill with spotted fever. Humans are dead-end hosts

5
Rocky Mountain Spotted Fever (RMSF) Signs/Symptoms Average incubation 1 week after bite Fever (acute onset), possibly accompanied by –Headache –Malaise –Myalgia –Nausea/vomiting –Neurologic signs Fatal in 5-10% of untreated cases Severe fulminant disease possible
 Signs/Symptoms Average incubation 1 week after bite Fever (acute onset), possibly accompanied by –Headache –Malaise –Myalgia –Nausea/vomiting –Neurologic signs Fatal in 5-10% of untreated cases Severe fulminant disease possible")
6
Rocky Mountain Spotted Fever (RMSF) Signs/Symptoms (Continued) Characteristic spotted rash Macular or maculopapular rash in most (about 80% of) patients 4-7 days post-onset, Rash often present on palms and soles.
 Signs/Symptoms (Continued) Characteristic spotted rash Macular or maculopapular rash in most (about 80% of) patients 4-7 days post-onset, Rash often present on palms and soles.")
7
Rocky Mountain Spotted Fever (RMSF) Occurrence 71/88 counties in Ohio Almost half of all cases from Clermont, Franklin and Lucas (from 1999-2007) 19 deaths since 1964 April through July
 Occurrence 71/88 counties in Ohio Almost half of all cases from Clermont, Franklin and Lucas (from ) 19 deaths since 1964 April through July")
8
Rocky Mountain Spotted Fever (RMSF)
")
12
Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) Laboratory Confirmed: Serological evidence of a fourfold change in IgG-specific antibody titer reactive with R. rickettsii antigen by indirect IFA between paired serum specimens*, or Detection of R. rickettsii DNA in clinical specimen via amplification of a specific target by PCR assay, or Demonstration of spotted fever group antigen in biopsy or autopsy specimen by IHC, or Isolation of R. rickettsii from clinical specimen in cell culture

13
Rocky Mountain Spotted Fever (RMSF) Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) Laboratory Supportive: Serologic evidence of elevated IgG or IgM antibody reactive with R. rickettsii antigen by IFA, ELISA, dot- ELISA, or latex agglutination*

14
Rocky Mountain Spotted Fever (RMSF) Case Definitions for Surveillance Confirmed: A clinically compatible case (meets clinical evidence criteria*) that is laboratory confirmed. Probable: A clinically compatible case (meets clinical evidence criteria*) that has supportive laboratory results. Suspect: A case with laboratory evidence of past or present infection but no clinical information available (e.g. a laboratory report).
 that has supportive laboratory results. Suspect: A case with laboratory evidence of past or present infection but no clinical information available (e.g. a laboratory report)..")
15
Rocky Mountain Spotted Fever (RMSF) Treatment (need based on clinical and epidemiological information) Tetracycline antibiotics (usually doxycycline) Treat for at least 3 days after fever subsides and until evidence of clinical improvement Standard duration of treatment: 5-10 days
 Treatment (need based on clinical and epidemiological information) Tetracycline antibiotics (usually doxycycline) Treat for at least 3 days after fever subsides and until evidence of clinical improvement Standard duration of treatment: 5-10 days")
16
Rocky Mountain Spotted Fever (RMSF) Prevention and Control Avoid ticks in endemic areas Tuck pants into socks Use repellents (carefully following label instructions) Wear light-colored clothing Regularly inspect for and remove ticks (on humans and pets) Keep grass and weeds mowed
 Prevention and Control Avoid ticks in endemic areas Tuck pants into socks Use repellents (carefully following label instructions) Wear light-colored clothing Regularly inspect for and remove ticks (on humans and pets) Keep grass and weeds mowed")
17
Rocky Mountain Spotted Fever (RMSF)
")
18
Lyme Disease Agent/transmission Borrelia burgdorferi Reservoir=mice, squirrels, other small animals Ixodes scapularis (black-legged tick, also known as “deer tick”)=vector in eastern and midwestern states Ixodes pacificus=vector in western United States Other species of ticks not known to transmit Lyme Disease. No known human-human transmission (though transplacental transmission may occur)
.")
19
Lyme Disease Signs/Symptoms Incubation period of up to 30 days after tick bite Muscle aches Fever Swollen lymph nodes Headache Joint pain Fatigue Late manifestations

20
Lyme Disease Signs/Symptoms (Continued) Erythema migrans (“bull’s-eye” rash) –Best clinical marker –Seen in 60-80% of cases –Develops at site of tick attachment after a delay of 3-30 days –Usually appears 7-14 days after exposure –Gradually expands over several days
 Erythema migrans ( bull’s-eye rash) –Best clinical marker –Seen in 60-80% of cases –Develops at site of tick attachment after a delay of 3-30 days –Usually appears 7-14 days after exposure –Gradually expands over several days")
21
Lyme Disease Occurrence Since 1990, 932 cases reported from 83/88 Ohio counties 48 cases reported to CDC in 2008 Most commonly reported vector-borne disease in U.S. with 20,000 cases each year 80% of total U.S. cases from Mid-Atlantic and New England (mostly New York, New Jersey and Pennsylvania) Black-legged tick rare in Ohio
 Black-legged tick rare in Ohio.")
22
Lyme Disease

26
Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) Positive culture for B. burgdorferi, or Demonstration of diagnostic IgM or IgG antibodies to B. burgdorferi in serum or CSF*, or Single-tier IgG Western blot / immunoblot seropositivity interpreted using established criteria*

27
Lyme Disease Case Definitions for Surveillance Confirmed: a) a case of EM with a known exposure, or b) a case of EM with laboratory evidence of infection (by CDC lab criteria) and without a known exposure or c) a case with at least one late manifestation that has laboratory evidence of infection. Probable: any other case of physician-diagnosed Lyme disease that has laboratory evidence of infection (by CDC lab criteria). Suspected: a) a case of EM where there is no known exposure and no laboratory evidence of infection, or b) a case with laboratory evidence of infection but no clinical information available (e.g. a laboratory report).
. Suspected: a) a case of EM where there is no known exposure and no laboratory evidence of infection, or b) a case with laboratory evidence of infection but no clinical information available (e.g. a laboratory report)..")
28
Lyme Disease Treatment Antibiotic therapy during acute phase Doxycycline, amoxicillin, or cefuroxime axetil IV ceftriaxone or penicillin for neurological or cardiac Second 4-week course if symptoms persist or recur

29
Lyme Disease Prevention, and Control Vaccine no longer available Avoid of ticks in endemic areas Tuck pants into socks Wear light-colored clothing Use repellents (carefully following label instructions) Regularly inspect for and remove ticks (on humans and pets) Keep grass and weeds mowed Reduce reservoir populations
 Regularly inspect for and remove ticks (on humans and pets) Keep grass and weeds mowed Reduce reservoir populations")
30
Lyme Disease

31
Ehrlichiosis/Anaplasmosis Agents/transmission Ehrlichia chaffeensis - formerly known as human monocytic ehrlichiosis (HME) Anaplasma phagocytophilum, (aka Ehrlichia equi or Ehrlichia phagocytophila) - formerly known as human granulocytic ehrlichiosis (HGA, HGE) Ehrlichia ewingii
 Anaplasma phagocytophilum, (aka Ehrlichia equi or Ehrlichia phagocytophila) - formerly known as human granulocytic ehrlichiosis (HGA, HGE) Ehrlichia ewingii")
32
Ehrlichiosis/Anaplasmosis Agents/transmission E. chaffeensis is transmitted principally by the Lone Star tick, Amblyomma americanum A. phagocytophilum appears to be transmitted by the blacklegged ticks, Ixodes scapularis and Ixodes pacificus. E. ewingii appears to be transmitted by the Lone Star tick, Amblyomma americanum. Reservoirs for vector ticks: deer, elk, wild rodents and dogs.

33
Ehrlichiosis/Anaplasmosis Humans contract Ehrlichiosis/Anaplasmosis through the bite of vector tick, or by coming in contact with tick secretions or body fluids through careless handling of ticks. Humans are dead-end hosts.

34
Ehrlichiosis/Anaplasmosis Signs/symptoms Incubation period: 5-14 days after tick bite for Ehrlichia chaffeensis infection and E. ewingii infection; 5-21 days for Anaplasma phagocytophilum infection Fever (acute onset) and one or more of the following: –Headache –Myalgia –Malaise –Anemia –Leuokpenia –Thrombocytopenia –Hepatic transaminase elevation –Nausea –Vomiting –Rash (uncommon for HME, rare for HGE) Case fatality rate of 2-3% for E. chaffeensis, less than 1% for A. phagocytophilum, and not documented for E. ewingii
 and one or more of the following: –Headache –Myalgia –Malaise –Anemia –Leuokpenia –Thrombocytopenia –Hepatic transaminase elevation –Nausea –Vomiting –Rash (uncommon for HME, rare for HGE) Case fatality rate of 2-3% for E. chaffeensis, less than 1% for A. phagocytophilum, and not documented for E. ewingii.")
35
Ehrlichiosis/Anaplasmosis Occurrence Found primarily in the South and Mid-Atlantic, North/South Central United States, and isolated areas of New England, E. chaffeensis is transmitted principally by the Lone Star tick, Amblyomma americanum. A. phagocytophilum is more likely to be found in the New England, North Central and Pacific States, and appears to be transmitted by the blacklegged ticks, Ixodes scapularis and Ixodes pacificus. Found primarily in the South Atlantic and South Central United States with isolated areas of New England, E. ewingii appears to be transmitted by the Lone Star tick, Amblyomma americanum. Lone Star ticks becoming more common in Ohio, especially Southern Ohio.

36
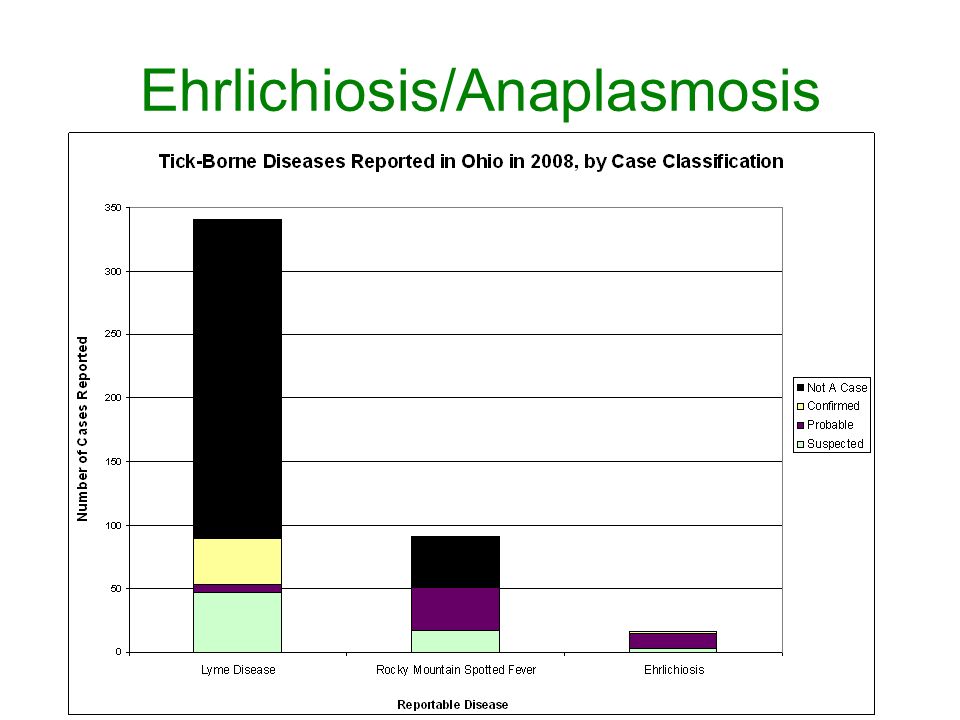
Ehrlichiosis/Anaplasmosis

42
Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) – E. chaffeensis (HME) Laboratory Confirmed: Serological evidence of fourfold change in IgG-specific antibody titer to E. chaffeensis antigen by indirect IFA between paired serum samples*, or Detection of E. chaffeensis DNA in clinical specimen via amplification of specific target by PCR assay, or Demonstration of ehrlichial antigen in biopsy or autopsy sample by immunohistochemical methods, or Isolation of E. chaffeensis from clinical specimen in cell culture
 Laboratory Confirmed: Serological evidence of fourfold change in IgG-specific antibody titer to E. chaffeensis antigen by indirect IFA between paired serum samples*, or Detection of E. chaffeensis DNA in clinical specimen via amplification of specific target by PCR assay, or Demonstration of ehrlichial antigen in biopsy or autopsy sample by immunohistochemical methods, or Isolation of E. chaffeensis from clinical specimen in cell culture.")
43
Ehrlichiosis/Anaplasmosis Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) – E. chaffeensis (HME) Laboratory Supportive: Serological evidence of elevated IgG or IgM antibody reactive with E. chaffeensis antigen by IFA, ELISA, dot-ELISA, or assays in other formats*, or Identification of morulae in the cytoplasm of monocytes or macrophages by microscopic examination
 Laboratory Supportive: Serological evidence of elevated IgG or IgM antibody reactive with E. chaffeensis antigen by IFA, ELISA, dot-ELISA, or assays in other formats*, or Identification of morulae in the cytoplasm of monocytes or macrophages by microscopic examination.")
44
Ehrlichiosis/Anaplasmosis Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) – E. ewingii Laboratory Confirmed: E. ewingii DNA detected in clinical specimen via amplification of a specific target by PCR assay

45
Ehrlichiosis/Anaplasmosis Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) – A. phagocytophilum (HGE) Laboratory Confirmed: Serological evidence of fourfold change in IgG-specific antibody titer to A. phagocytophilum antigen by indirect IFA in paired serum samples*, or Detection of A. phagocytophilum DNA in clinical specimen via amplification of a specific target by PCR assay, or Demonstration of anaplasmal antigen in biopsy/autopsy sample by immunohistochemical methods, or Isolation of A. phagocytophilum from clinical specimen in cell culture
 Laboratory Confirmed: Serological evidence of fourfold change in IgG-specific antibody titer to A. phagocytophilum antigen by indirect IFA in paired serum samples*, or Detection of A. phagocytophilum DNA in clinical specimen via amplification of a specific target by PCR assay, or Demonstration of anaplasmal antigen in biopsy/autopsy sample by immunohistochemical methods, or Isolation of A. phagocytophilum from clinical specimen in cell culture.")
46
Ehrlichiosis/Anaplasmosis Diagnosis (CDC Laboratory Criteria for Surveillance Purposes) – A. phagocytophilum (HGE) Laboratory Supportive: Serological evidence of elevated IgG or IgM antibody reactive with A. phagocytophilum antigen by IFA, ELISA, dot-ELISA, or assays in other formats*, or Identification of morulae in the cytoplasm of neutrophils or eosinophils by microscopic examination
 Laboratory Supportive: Serological evidence of elevated IgG or IgM antibody reactive with A. phagocytophilum antigen by IFA, ELISA, dot-ELISA, or assays in other formats*, or Identification of morulae in the cytoplasm of neutrophils or eosinophils by microscopic examination.")
47
Ehrlichiosis/Anaplasmosis Case Definitions for Surveillance Confirmed: A clinically compatible case (meets clinical evidence criteria) that is laboratory confirmed. Probable: A clinically compatible case (meets clinical evidence criteria) that has supportive laboratory results. Suspect: A case with laboratory evidence of past or present infection but no clinical information available (e.g. a laboratory report).
 that has supportive laboratory results. Suspect: A case with laboratory evidence of past or present infection but no clinical information available (e.g. a laboratory report)..")
48
Ehrlichiosis/Anaplasmosis Treatment Begin immediately upon strong suspicion of ehrlichiosis through clinical and epidemiological findings Doxycycline or other tetracyclines (fever generally subsides within 24-72 hours) Minimal course of 5-7 days Patients with anaplasmosis should be treated with doxycycline for 10-14 days because of possible Lyme disease coinfection
 Minimal course of 5-7 days Patients with anaplasmosis should be treated with doxycycline for days because of possible Lyme disease coinfection")
49
Ehrlichiosis/Anaplasmosis Prevention and Control Avoid ticks in endemic areas Tuck pants into socks Use repellents (carefully following label instructions) Wear light-colored clothing Regularly inspect for and remove ticks (on humans and pets) Keep grass and weeds mowed
 Wear light-colored clothing Regularly inspect for and remove ticks (on humans and pets) Keep grass and weeds mowed")
50
Ehrlichiosis/Anaplasmosis

51
Tick Identification Free service through ODH Zoonotic Disease Program Proper tick identification essential in determining potential risk of infection with tick-borne disease

52
Tick Identification Instructions for Submitting Ticks Keep ticks alive. Live ticks are easier to identify Moisten paper strip with one or two drops of water, place tick and paper strip in vial and close tightly. Complete form and submit with tick.

53
Tick Identification

54
Questions Christina Davey Regional Epidemiologist Serving Lawrence, Pike, Ross and Scioto Counties, Ironton and Portsmouth Cities Pike County General Health District (Home Office) 14050 US 23 N Waverly, OH 45690 Office Phone: 740-947-7721 Cell (24/7 Contact #): 740-222-2292 Email: cdavey@pike-health.org
 US 23 N Waverly, OH Office Phone: Cell (24/7 Contact #):")
Similar presentations












 March 20 2014. Lyme Disease First identified in 1975 in a group of arthritis patients in Lyme, Connecticut 1978 it was.>")










 ticks Untreated, the mortality is very high.>")

 Brown dog tick (Rhipicephalus sanguineus) Rocky.>")



