Download presentation
Presentation is loading. Please wait.

1
Evaluation and Management of Head Injuries in Sports
George S. Wham Jr., M.S., A.T.,C., S.C.A.T.

2
NATA Competencies concerning Head Injuries
Recognize signs and symptoms of head trauma, including loss of consciousness, changes in neurological function, cranial nerve assessment, and other symptoms that indicate brain injury Explain and interpret signs and symptoms associated with intracranial pressure Define cerebral concussion and lists the signs and symptoms used to classify cerebral concussion to accepted grading scales: Cantu, Colorado, ANA Assess a patient for possible closed-head trauma

3
Mechanisms of Injury Coup
a forceful blow to resting head, producing maximal injury beneath the point of impact example: being hit with a baseball or hockey puck

4
Mechanisms of Injury Contrecoup
moving head hits an unyielding object, producing maximal brain injury opposite the site of impact as the brain bounces within the cranium Example: head hits ground when being tackled

5
Mechanisms of Injury Repeated Sub-concussive Blows
Many nontraumatic blows overtime Example: Soccer players who head the ball frequently

6
Types of Head Injuries in Sports
Cerebral Concussion Cerebral Contusion Cerebral Hematoma

7
Cerebral Concussion Head trauma-induced alteration in mental status that may or may not involve a loss of consciousness

8
Cerebral Contusion A bruise of the brain resulting from an impact of the skull and an object causing bleeding from injured vessels May be associated with partial paralysis, one sided pupil dilation, and altered vital signs Progressive edema may further compromise brain tissue not injured in original trauma If basic life support, proper transport techniques, and prompt expert evaluation are delivered, no surgery is needed and prognosis is good

9
Cerebral Hematoma Blood clot in the tissue surrounding the brain causes pressure on the brain 3 Types Epidural Subdural Intercerebral

10
Epidural Hematoma Results from a severe blow to the head that produces a skull fracture in the temporoparietal region Neurological status may not be evident for 10 to 20 minutes after the injury Immediate surgery needed to decompress the hematoma and control the bleeding artery

11
Subdural Hematoma A blow to the skull that causes subdural blood vessels to tear resulting in venous bleeding and the slow formation of a clot Symptoms may not appear for hours, days, or even weeks Surgery is needed to drain the hematoma and decompress the brain

12
Intracerebral Hematoma
Bleeding from a torn artery collects within the brain itself Often results from a depressed fracture or penetrating wound No lucid interval after the injury Hematoma progresses rapidly Death occurs before the athlete can be moved to an emergency facility

13
Second Impact Syndrome
An athlete sustains a second concussion before an earlier one has resolved Potential for occurrence with mild head injuries Often the first concussion goes unreported or unrecognized A major consideration when making return to play decisions

14
Second Impact Syndrome (con’t)
Occurs within 1 week of initial injury Involves rapid brain swelling and herniation Brain stem failure develops within 2-5 minutes Causes rapid dilation of pupils, loss of eye movement, respiratory failure, and coma Athlete must be intubated Mortality rate 50%

15
Frequency of Concussions
1 in 5 (250,000) high school football players per year (Cantu 1986) 300,000 sport-related concussions per year (Thurman et al., 1998) Player is 3 times more likely to sustain a 2nd concussion after the 1st (Guskiewicz 2000) Only 1 in 100,000 high school football players suffer catastrophic injuries (Cantu 1999)
 high school football players per year (Cantu 1986) 300,000 sport-related concussions per year (Thurman et al., 1998) Player is 3 times more likely to sustain a 2nd concussion after the 1st (Guskiewicz 2000) Only 1 in 100,000 high school football players suffer catastrophic injuries (Cantu 1999)")
16
Who’s at Greatest Risk? (Mueller, F.O. 2001).
.")
17
Frequency of Head-Related Fatalities
(Mueller, F.O. 2001).
.")
18
Cause of Death? (Mueller, F.O. 2001).
.")
19
It’s Getting Better ….. (Mueller, F.O., 2001).
.")
20
OK, but isn’t it just football?.…
(Mueller, F.O., 2001).
.")
21
Mouth Guards Decrease Concussions? How?
(Winters, J.E., 2001)
")
22
Grading Scales Cantu (1984) Colorado Medical Society (1991)
American Academy of Neurology (1997)
")
23
Cantu’s Scale (1984) Grade 1 – no loss of consciousness
Grade 2 – loss of consciousness < 5 minutes Grade 3 – loss of consciousness > 5 minutes Revised in 1992 (Shultz et al., 2000)
")
24
Colorado Medical Society’s Scale
Grade 1 – confusion; no amnesia; no loss of consciousness Grade 2 – confusion; amnesia; no loss of consciousness Grade 3 – any loss of consciousness

25
American Academy of Neurology’s Scale
Grade 1 – confusion less than 15 minutes, no loss of consciousness Grade 2 – confusion greater than 15 minutes, no loss of consciousness Grade 3 – any loss of consciousness

26
A.A.N.’s Recommendations for Management of Concussions in Sports
For a grade 1 Remove from activity Examine immediately and at 5 minute intervals Allow to return only if post-concussive symptoms resolve within 15 minutes If a 2nd grade 1 concussion occurs on the same day then remove until asymptomatic for 1 week

27
A.A.N.’s Recommendations for Management of Concussions in Sports
For a Grade 2 Remove from activity Examine frequently to assess the evolution of symptoms, with more extensive diagnostic evaluation if symptoms worsen or persist for more than 1 week Athlete may return to play after 1 week asymptomatic

28
A.A.N.’s Recommendations for Management of Concussions in Sports
For a Grade 3 Remove from activity for 1 week if loss of consciousness is brief, or for 2 weeks if prolonged If unconscious at time of initial evaluation or if neurological signs are abnormal, the athlete should be transported by ambulance to ER If a 2nd grade 3 occurs, the athlete should not return to sport until asymptomatic for 1month

29
If any abnormality exists on the MRI or CT scan the athlete should be removed from activity for the season and discouraged from a future return to contact sports

30
Another Classification Scale to Consider?
(Oliaro, S., et al. 2001).
.")
31
More Return to Play Guidelines
(Oliaro, S., et al. 2001).
.")
32
Evaluation

33
Signs of Severe Brain Damage
Damage below brain stem Rigid extension of all 4 extremities with arms internally rotated and pronated Damage above brain stem. Rigid extension of legs and flexion of the arms, wrist, and hands towards the chest Babinski Sign

34
Thorough Evaluation Before an Athlete Is Allowed to Return to Play
On-field Assessment Primary Survey Secondary Survey Off –field Assessment

35
On-field Assessment Primary survey check ABC’s Secondary survey
H.O.P.S. protocol determine if the athlete can go to the sideline for further evaluation or needs an ambulance **Often there is no “player down” assessment**

36
Check for Signs of Skull Fracture
Battle’s Sign – posterior auricular hematoma Ottorrhea – CSF draining from ears Rhinorrhea – CSF draining from nose Raccoon Eyes – periorbital ecchymosis resulting from blood leaking from anterior fossa of skull

37
Symptoms of a Concussion
Headache, nausea, vomiting, dizziness, poor balance, sensitivity to noise or light, ringing in the ears, blurred vision, poor concentration, memory problems, trouble sleeping, sleepiness, depression, irritability Only 8.9% result in a loss of consciousness (Guskiewicz et al., 2000)
")
38
Method to Rate Severity of Signs & Sx
(Oliaro, S., et al. 2001).
.")
39
Initial Assessment Obtain information about mental confusion, any loss of consciousness, and amnesia Confusion: dazed, stunned, or glassy-eyed facial expression; behaviors like running to the wrong huddle Unconscious: assume a cervical spine injury exists, athlete spine boarded sent to ER; If conscious ask if he has any tingling, numbness, or neck pain. Also, can he move his fingers and toes? Amnesia: test for post-traumatic amnesia by asking what he remember about the last play; test for retrograde amnesia by asking name, date, place

40
Initial Assessment (con’t)
Ask athlete if “his ears’ are ringing”, he has blurry vision, or nausea Check for any facial abnormalities While asking questions, observe speech patterns, respirations, and movement of the extremities Palpate the athlete’s cervical spine and skull to rule out fracture, assuming neck injury has been ruled out Walk to sideline for further assessment

41
Glasgow Coma Scale Used to assess level of consciousness
(Shultz et al., 2000)
")
42
Cranial Nerve Assessment
Rule out problems with II, III, IV, VI first II – check vision by read scoreboard and fingers III, IV, VI – check eye movement by asking athlete to track a moving object, check pupils for equal size and light reactivity with a penlight ** problems indicate increased intracranial pressure** (Shultz et al., 2000)
")
43
Further Cranial Nerve Assessment
I – check smell V – check by clinching jaw VII – check by raising eyebrows, smiling VIII – check balance and hearing IX and X – check by swallowing XII – check by sticking out tongue XI – check by neck rotation/extension and shoulder shrug

44
(Shultz et al., 2000)
")
45
Test Sensory/Motor Function
Dermatome Testing Myotome Testing ROM Testing Strength Testing

46
Upper Extremity Dermatome Testing
C6: Lateral forearm, thumb, fore finger C7: posterior forearm, middle finger C8: Lower medial forearm, 4th and 5th fingers T1: Medial forearm C1: Top of head C2: Temporal, Occipital C3: Neck, Posterior Check C4: Superior Shoulder C5: Deltoid patch

47
Upper Extremity Myotome Testing
C1/C2: Cervical flexion C3: Lateral neck flexion C4: Shoulder Shrug C5: Shoulder Abduction C6: Elbow flexion, wrist extension C7: Elbow extension, wrist flexion C8: Ulnar deviation, thumb extension, finger flexion & abduction T1: Finger abduction/adduction

48
Check Vital Signs Increased pulse, increased systolic blood pressure, and a decreasing diastolic blood pressure indicates increasing intracranial pressure A decrease in systolic bp denotes shock

49
Check for Post-traumatic Amnesia (Anterograde)
Give the athlete 3 unassociated words to remember, and periodically ask for recall Example: Red, Explorer, Clemson

50
Check for Retrograde Amnesia
Ask questions like Where are we playing? Which quarter is it? What did we have for pre-game meal? Who did we play last week?

51
Check for Concentration
Have athlete Recite days of the week or months of the year backward Count backward from 100 by 7’s (Serial 7’s) Multiple/Addition facts
 Multiple/Addition facts.")
52
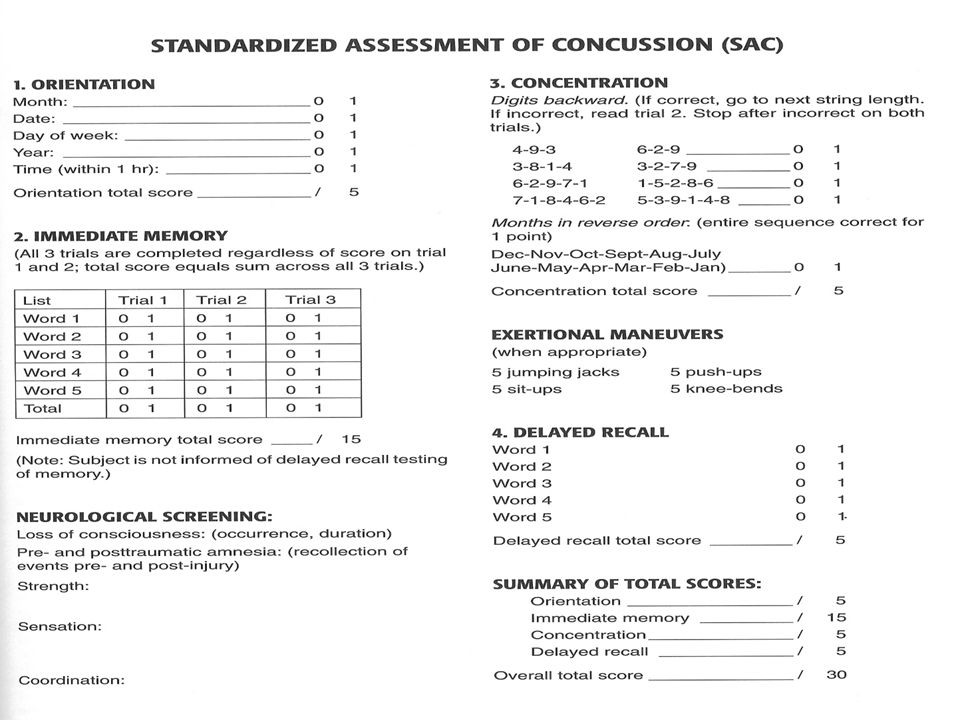
SAC (Standardized Assessment of Concussion)
Designed to detect impaired concentration Sideline or follow-up evaluation tool Takes 5 minutes to assess: Orientation Immediate memory Neurological fxn Concentration Delayed recall Sx during exertional testing (McCrea et al., 1997)
")
54
Neurocognitive Assessments
Trail-Making Test B: (working memory and rapid visual processing) Connect circles containing letters (A-L) to numbers (1-13) in alternating numeric fashion as fast as possible. Wechsier Digit Span Test: (concentration and memory recall) Subjects presented w/ a series of numbers and must repeat digits in same order or reverse order. (Guskiewicz, K. M. et al., 2001)
 Connect circles containing letters (A-L) to numbers (1-13) in alternating numeric fashion as fast as possible. Wechsier Digit Span Test: (concentration and memory recall) Subjects presented w/ a series of numbers and must repeat digits in same order or reverse order. (Guskiewicz, K. M. et al., 2001)")
55
Check Balance, Coordination, and Depth Perception
Romberg’s Test Finger-to-Nose Test Finger-to-Finger Test Heel-to-Toe Walking Supine Heel-to-Knee Test

56
Nerurocom Smart Balance Master System
SOT (Sensory Organization Test) Forceplate system measures postural sway by quantifying balance deficits and sensory organization problems resulting from a concussion Expensive and immobile (Guskiewicz, K. M. et al., 2001)
 Forceplate system measures postural sway by quantifying balance deficits and sensory organization problems resulting from a concussion. Expensive and immobile. (Guskiewicz, K. M. et al., 2001)")
57
NeuroCom Smart Balance Master vs BESS
(Guskiewicz, K. M. et al., 2001) Strong Correlation between the two tests!
 Strong Correlation between the two tests!")
58
Balance Error Scoring System (BESS)
Quantifiable modified Rhomberg 3 tests lasting 20s each Double-leg Single-leg Heel-toe Eyes Closed Perform once on ground and once on foam Tally number of errors (Guskiewicz, K. M. et al., 2001)
")
59
6 Types of Errors in BESS (Guskiewicz, K. M. et al., 2001)
")
60
Test Equilibrium and Balance
(Oliaro, S., et al. 2001).
.")
61
(Shultz et al., 2000)
")
62
How long do symptoms linger?
Post Concussion Syndrome (Guskiewicz, K. M. et al., 2001)
")
63
Functional Testing Must be asymptomatic
Designed to see if activity will cause symptoms Sit-ups Push-ups Jogging Running Sports Specific Tasks

64
Return to Play Protocol
95% of baseline on cognitive and balance tests (Oliaro, S., et al. 2001).
.")
65
Return to Play Assuming the athlete passes the complete exam he/she may return to play

66
Take Home Message While experts argue over specifics of the guidelines all agree – NO ATHLETE EXPERIENCING SYMPTOMS SHOULD PARTICIPATE!

67
References Guskiewicz, K.M., Weaver, N.L., Padua, D.A., Garrett, W.E. (2000). Epidemiology of concussion in collegiate and high school football players. American Journal of Sports Medicine, 28, Guskiewicz, K.M., Ross S.E., Marshall, S. W. (2001). Postural stability and neuropsychological deficits after concussion in collegiate athletes. Journal of Athletic Training. 36 (3), McCrea, M, Kelly, J.P., Kluge, J., Ackley, B., and Randolph, C. (1997). Standardized assessment of concussion in football players. Neurology, 48, (3), Mueller, F.O. (2001). Catastrophic head injuries in high school and collegiate sports. Journal of Athletic Training 36, (3), Oliaro, S., Anderson S., and Hooker, D. (2001). Management of cerebral concussion in sports: the athletic trainer’s perspective. Journal of Athletic Training, 36, (3), Shultz, S.J., Houghlum, P.A., Perrin, D.H. (2000). Assessment of Athletic Injuries. (1st Ed., pp ). Human Kinetics. Champaign IL. Thurman, J.D., Branche C.M., Sniezek, J.E. (1998). The epidemiology of sports-related traumatic brain injuries in the United States: recent developments. Journal of Head Trauma Rehabilitation, 13, 1-8. Winters, J.E. (2001). Commentary: Role of properly fitted mouthguards in prevention of sport-related concussion. Journal of Athletic Training, 36 (3),
. Epidemiology of concussion in collegiate and high school football players. American Journal of Sports Medicine, 28, Guskiewicz, K.M., Ross S.E., Marshall, S. W. (2001). Postural stability and neuropsychological deficits after concussion in collegiate athletes. Journal of Athletic Training. 36 (3), McCrea, M, Kelly, J.P., Kluge, J., Ackley, B., and Randolph, C. (1997). Standardized assessment of concussion in football players. Neurology, 48, (3), Mueller, F.O. (2001). Catastrophic head injuries in high school and collegiate sports. Journal of Athletic Training 36, (3), Oliaro, S., Anderson S., and Hooker, D. (2001). Management of cerebral concussion in sports: the athletic trainer’s perspective. Journal of Athletic Training, 36, (3), Shultz, S.J., Houghlum, P.A., Perrin, D.H. (2000). Assessment of Athletic Injuries. (1st Ed., pp ). Human Kinetics. Champaign IL. Thurman, J.D., Branche C.M., Sniezek, J.E. (1998). The epidemiology of sports-related traumatic brain injuries in the United States: recent developments. Journal of Head Trauma Rehabilitation, 13, 1-8. Winters, J.E. (2001). Commentary: Role of properly fitted mouthguards in prevention of sport-related concussion. Journal of Athletic Training, 36 (3),")
Similar presentations







>")











