Download presentation
Presentation is loading. Please wait.

1
Concussion Evaluation: On the Sideline Jennifer E Sanders, MD Pediatric Emergency Medicine Fellow Icahn School of Medicine at Mount Sinai Department of Emergency Medicine

2
None Financial Disclosures Department of Emergency Medicine

3
12 year old soccer player collides with another player, striking their heads together. There is no loss of consciousness. He is pulled over to this sideline where he reports he has no headache or dizziness. He is put back into the game, but has trouble finding his position on the field and runs in the direction opposite his team. Does this player have a concussion? Should he be allowed to continue play? How should he be evaluated? Case Department of Emergency Medicine

4
Know how to recognize concussion symptoms Understand the role of concussion assessment tools Recognize that no child with concussion or suspected of having concussion should return to play on the same day Objectives/Goals Department of Emergency Medicine

5
Physicians Nurses Athletic trainers Coaches Parents Who is responsible? Department of Emergency Medicine

6
Impact may be obvious or subtle Play may not stop after the injury Players may minimize or deny symptoms Recognizing the injury Department of Emergency Medicine McCrea M, Barr WB, Guskiewicz KM, et al. Standard regression-based methods for measuring recovery after sport-related concussion.J Int Neuropsychol Soc. 2005;11:58-69.

7
Somatic symptoms Physical signs Behavioral / emotional changes Cognitive impairment Sleep disturbance Signs and symptoms Department of Emergency Medicine

8
ABCs C-spine evaluation Remove child from play Serial monitoring Initial response Department of Emergency Medicine

9
Standardized Assessment of Concussion (SAC) Balance Error Scoring System (BESS) Sport Concussion Assessment Tool (SCAT) SCAT-3 (age >13 years) SCAT-3 Child (age 5-12 years) On-field assessment tools Department of Emergency Medicine
 Balance Error Scoring System (BESS) Sport Concussion Assessment Tool (SCAT) SCAT-3 (age >13 years) SCAT-3 Child (age 5-12 years) On-field assessment tools Department of Emergency Medicine")
10
SAC- 1 point drop 80-94% sensitivity 76-91% specificity BESS- 3 point increase 34-64% sensitivity 91% specificity SCAT unknown On-field assessment tools Department of Emergency Medicine

11
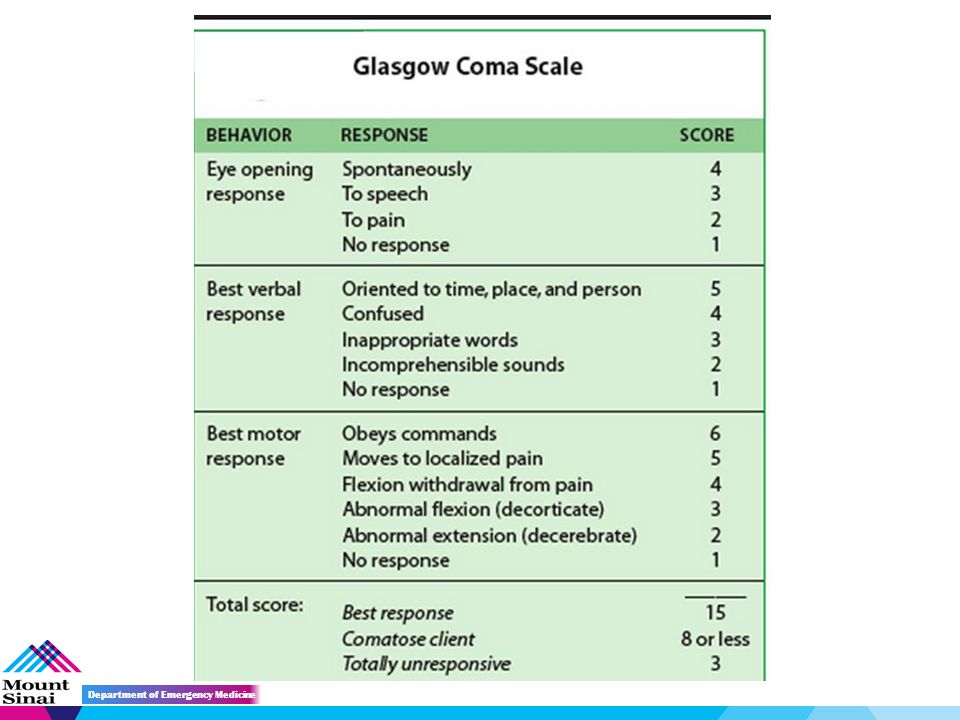
On-field assessment tools 15-20 minute battery Includes: Glascow Coma Score SAC Modified BESS Department of Emergency Medicine

13
Maddock’s Score What venue are we at today? Which half is it now? Who scored last in this match? What team did you play last week? Did your team win the last game? SCAT-3 Department of Emergency Medicine

14
Symptom evaluation 22 symptoms Likert scale Self reported SCAT-3 Department of Emergency Medicine

15
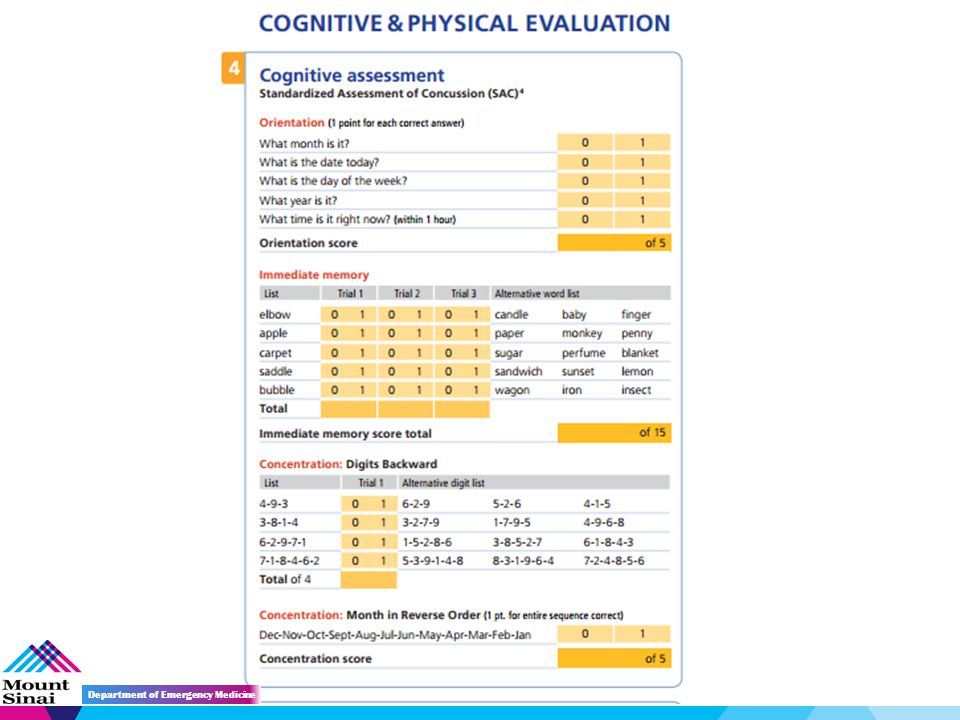
SAC Cognitive assessment Orientation Immediate memory Concentration Delayed recall SCAT-3 Department of Emergency Medicine

17
Neck exam Range of motion Tenderness over spinous processes Upper and lower limb sensation and strength SCAT-3 Department of Emergency Medicine

18
Balance Examination (modified BESS) Double leg stance Single leg stance* Tandem stance Tandem gait *Not included in SCAT-3 Child SCAT-3 Department of Emergency Medicine
 Double leg stance Single leg stance* Tandem stance Tandem gait *Not included in SCAT-3 Child SCAT-3 Department of Emergency Medicine")
19
Double leg stance Feet together Hands on hips Eyes closed Single leg stance Stand on non-dominant foot Dominant leg: 30° hip flexion / 45° knee flexion Hands on hips Eyes closed SCAT-3 Department of Emergency Medicine

20
Tandem stance Heel-to-toe with dominant foot in back Weight evenly distributed across both feet Hands on hips Eyes closed SCAT-3 Department of Emergency Medicine

21
Balance testing errors Hands lifted off iliac crest Opening eyes Step, stumble or fall Moving hip into > 30° abduction Lifting forefoot or heel Remaining out of test position > 5 sec SCAT-3 Department of Emergency Medicine

22
Tandem gait Feet together behind starting line Walk forward with alternate heel-to-toe gait for 3 meters Return to starting point with same gait 4 trials performed Should be completed within 14 seconds SCAT-3 Department of Emergency Medicine

23
Coordination Finger-nose-finger (1 point) 5 repetitions in <4 seconds SAC Delayed Recall Recall word list (5 points) SCAT-3 Department of Emergency Medicine
 5 repetitions in <4 seconds SAC Delayed Recall Recall word list (5 points) SCAT-3 Department of Emergency Medicine")
24
Scores can be followed over time SCAT-3 is not intended to diagnose concussion SCAT-3 Department of Emergency Medicine

25
When in doubt, sit them out! No child athlete with a concussion should return to play on the same day Sequester essential playing equipment to avoid inadvertent return to the game Return to play? Department of Emergency Medicine

26
No protective equipment has been clinically shown to prevent concussions Helmets Helmet add-on products Mouth guards Protective equipment Department of Emergency Medicine McGuine TA, Hetzel S, Rasmussen J, et al. The Association of the Type of Football Helmet and Mouth Guard With the Incidence of Sport Related Concussion in High School Football Players. Unpublished paper presented at 2013.AOSSM Annual Meeting. Paper 27.

27
When to refer to ED? Department of Emergency Medicine Loss of consciousness Focal neurologic deficit Unequal pupil size Severe symptoms Decreasing mental status Uncontrolled vomiting GCS <15

28
Questions? Department of Emergency Medicine

Similar presentations




>")














