Download presentation
Presentation is loading. Please wait.

1
DISEASES OF RESPIRATORY SYSTEM
The Department of Pathology Zili Lv 吕自力

2
Go over Pneumonia lobar pneumonia Air space pneumonia
lobular pneumonia Air space pneumonia Interstitial pneumonia viral pneumonia mycoplasma pneumonia Good morning everyone, last time we have talked about pneumonia, Penumonia can be classified into 2 groups: air space and interstitial Air space, we have talked about lobar and lobular, the alveolar have been invloved , the differences: the exudation: fibrous, neutrophil, the sputum: rusty and purulent

3
Respiratory system diseases 2
Chronic (diffuse) obstructive passage disease Chronic cor pulmonale |
 obstructive passage disease. Chronic cor pulmonale. |")
4
Chronic Obstructive Pulmonary Diseases, COPD
Chronic bronchitis 慢性支气管炎* Pulmonary emphysema 肺气肿* Bronchial asthma 支气管哮喘 Bronchiectasis 支气管扩张症 COPD refers to a group diseases These diseases have the same symptom: dyspnea, shortness of breath COPD is diagnosed by abnormalities of tests of ventilatory function. The major diseases are: chronic bronchitis, pulmonary emphysema, bronchial asthma and bronchiectasis

5
Chronic Bronchitis Definition:
A persistent productive cough, sputum for at least 3 months in at least 2 consecutive years. The most common disease in respiratory system. More common in old age (<40 ) Most cases caused by smoking Chronic bronchitis is a clinical name It is chronic inflammation happens in bronchus Often happens in old man, especially in cigarette smokers.
 Most cases caused by smoking. Chronic bronchitis is a clinical name. It is chronic inflammation happens in bronchus. Often happens in old man, especially in cigarette smokers.")
6
A. Etiology and Pathogenesis
Causes: Cigarette smoking: 90% Air pollution: sulfur dioxide and nitrogen dioxide, may contribute. 3. Microorganism infection is often present but plays a secondary role. So the disease is more common in city than in country, more common in developing countries than developed

7
Etiology and Pathogenesis
Smoking Pollution Infection Destroy the defensive mechanisms Hypertrophy of mucous glands Metaplasia of squamous Infiltration of inflammatory cells

8
B. Pathology* The inflammation of trachea and larger bronchi Grossly:
Hyperemia, Edema, Mucous or mucopurulent secretion The surface of the mucus-membrane of the bronchus is covered with a layer of mucous-secretion, sometimes with purulent

9
Histology The injury and regeneration of epithelia.
The hypertrophy, hyperplasia and metaplasia of mucus-secreting glands. (Reid I >0.5) Infiltration with chronic and acute inflammatory cells. The epithelium losses it’s ciliated cells, and have been replaced by squamous epitheilium The Reid Index- the ratio of mucous gland thichkeness to bronchial wall thickness- is increased above the normal value of 0.5
 Infiltration with chronic and acute inflammatory cells. The epithelium losses it’s ciliated cells, and have been replaced by squamous epitheilium. The Reid Index- the ratio of mucous gland thichkeness to bronchial wall thickness- is increased above the normal value of 0.5.")
10
上皮损伤与修复 The epitheilium loss its ciliary
A lot of chronic inflammatory cells infiltrated in the wall of bronchi The wall is thicken The smooth muscle is injuried

11
Squamous metaplasia The cilliated cell displaced by squamous epithelium, it may become dysplastic, and even become malignant The mucus membrane is covered with squamous epithelium.

12
An increase of goblet cells
The goblet is hyperplasia and can secret a lot of mucous, it may be a mucous plug, and produce the obstruction of the airways

13
Hypertrophy and hyperplasia of mucos-secreting glands

14
C. Clinical Features Cough Sputum Puff Secretion
For the patients, there are two typical features: production of cough and sputum For the chronic patients, may be only mucous sputum, but if the patients infect with bacterial, the symptom may be serious, for example: fever, purulent sputum, dyspnoea, hypercapnia, cyanosis.

15
D. Complications Bronchiectasis Cor pulmonale Bronchopneumonia
Chronic bronchitis Cor pulmonale Pulmonary emphysema

17
Pulmonary Emphysema 肺气肿
Emphysema : Permanent enlargement of the airspaces distal to the terminal bronchioles. Accompanied by destruction of their walls.

18
We can see the enlargement from terminal bronchioles to the end
The dilation from the terminal bronchiole to the alveolar We know the airway is getting narrower and narrower until to the pleura

19
A. Classification of emphysema
Centriacinar(腺泡中央型) Alveolar Periacinar (腺泡周边型) Panacinar (全腺泡型) Interstitial: The air comes into the septa of the lung. There are two major types of emphysema: Alveolar emphysema, it is the most common type. According to the location of the lesions within the pulmonary acinus, there are three principal types: centriacinar, panacinar and periacinar. Interstitial emphysema, it refers to the accumulation of air in the interstitial tissues, and is most commonly due to traumatic rupture of an airway or spontaneous rupture of an emphysematous bulla. The air may spread to mediastinum or subcuits, giving the characteristic spongy crepitus on palpation. Others type
 Alveolar. Periacinar (腺泡周边型) Panacinar (全腺泡型) Interstitial: The air comes into the septa of the lung. There are two major types of emphysema: Alveolar emphysema, it is the most common type. According to the location of the lesions within the pulmonary acinus, there are three principal types: centriacinar, panacinar and periacinar. Interstitial emphysema, it refers to the accumulation of air in the interstitial tissues, and is most commonly due to traumatic rupture of an airway or spontaneous rupture of an emphysematous bulla. The air may spread to mediastinum or subcuits, giving the characteristic spongy crepitus on palpation. Others type.")
20
This a normal lobular, consists of 4 acinars, from terminal bronchioles to respiratory bronchioles, alveolar duct, alveolar sac, alveoli

21
Centriacinar腺泡中央型 Heavy smokers
The dilation involves the center of the acinar, the respiratory bronchiole Occurs predominatly in heavy smokers, often in association with chronic bronchitis

22
Panacinar 全腺泡型 A1-AT deficiency
The dilation and destruction involve the entire acinus, including the alveoli and alveolar ducts as well as the respiratory bronchioles It is probably associated with A1-antitrypsin deficiency

23
Periacinar 腺泡周围型 This is periacinar emphysema
The dilation involves the distal acinar from respiratory bronchioles It occurs adjacent to areas of fibrosis, scarring Is usually more severe in the upper half lung.

24
B. Pathology* Grossly: pale and voluminous lungs emphysema
Normal lungs emphysema The chest and abdominal cavities are opened here at autopsy. The lungs in the chest have a normal pink aerated appearance with minimal anthracotic pigmentation, because this 80 year old male never smoked and never allowed smoking in his workplace. The mediastinum contains mostly fat. The pericardial sac around the heart has not been opened.The diaphragmatic domes extend upward to the level of the 6th ribs. The lung obviously becomes large, pink or pale, soft but with poor elasticity

26
are prone to rupture causing spontaneous pneumothorax
Bullous lung 肺大泡 Balloon-like >10 mm in diameter are prone to rupture causing spontaneous pneumothorax 自发性气胸 We can see a balloon-like foci of emphysema over 10 mm in diameter. Bullae are prone to rupture causing spontaneous pneumothorax

27
Histology 1.Thinning and destruction of alveolar walls, septa broken, adjacent alveoli become confluent. 2. Terminal and respiratory bronchioles may be deformed. 3. The number of alveolar capillaries decreases.

28
Thinning and destruction of alveolar walls, large airspaces
Histotogically: thinning and destruction of alveolar walls. With advanced disease, adjacent alveoli become confluent, creating large airspaces. Small airways collapse during expiration (the loss of elastic tissue in the surrounding alveolar septa, there is reduced radial traction on the small airways). the number of alveolar capillaries is diminished.
. the number of alveolar capillaries is diminished.")
29
C. Pathogenesis* Proteases Anti-proteases Leukocytes Alfa1-antitrypsin
The balance: one side is protease, which damage soft tissue, another side is antiprotease, which can protect the soft tissues from danmage. Protease is released by leukocytes, for example neutriphils, for cigeratter smoking, chronic inflammation occurs, it stimulates the leukocytes secreting proteases. In some inheritance deficiency, the antiproteases activity is poor. Then the septa will be damaged by protease, a lot of alveoli will be confident and become a big sac. Smoking, Inflammation Inheritance

30
D. Clinical Features Cough : dry or productive Dyspnea Mucoid sputum
Type A: Pink puffers Type B: Blue bloaters

31
Barrel chest 桶状胸 The anteroposterior diameter is increased

32
Relationship between chronic bronchitis and emphysema
chronic bronchitis and emphysema usually co-exist because the major pathogenic mechanism, cigarette smoking, is common to both.

34
Bronchial Asthma 支气管哮喘
Increased responsiveness of tracheobronchial tree to a variety of stimuli. Bronchiolar smooth muscle contraction (bronchospasm支气管痉挛). Paroxysmal attacks阵发性 Mucus plugs in bronchi
. Paroxysmal attacks阵发性. Mucus plugs in bronchi.")
35
A. Etiology and pathogenesis
Hypersensitivity Hyper-reactive airways Bronchial smooth muscle spasm Hypersecretion—mucus plugs Increased vascular permeability The cause of asthma is unknown, but is believed to be related to bronchial inflammation For the mechanisms, a lot of scientists believe type I and iii hypertensitivity are related to the disease Inflammation Nerve system

36
B. Clinical Features— episodic attacks
Dyspnea(呼吸困难) Wheezing(喘) Dry cough 邓丽君1995年5月8日死于泰国,气喘发作 The Chinese famous singer died in Thailand, in 8th May, 1995, after paroxysmal wheezing attacked
 Wheezing(喘) Dry cough. 邓丽君1995年5月8日死于泰国,气喘发作. The Chinese famous singer died in Thailand, in 8th May, 1995, after paroxysmal wheezing attacked.")
37
4. BRONCHIECTASIS 支气管扩张症
Permanent dilation of bronchi and bronchioles Results from bronchial obstruction with distal infection and scarring Destruction of alveolar walls, especially interstitial elastin, and fibrosis of lung parenchyma

38
Dilation The destruction of the wall Fibrosis Fibrosis Obstruction
Chronic inflammation Congenital, hereditary The destruction of the wall Dilation Fibrosis Fibrosis Congenital or hereditary conditions. Only a few are cited: cystic fibrosis, immunoglobulin deficiencies, Necrotizing, or suppurative, pneumonia Bronchial obstruction. Common causes are tumors, foreign bodies. Under these conditions, the bronchiectasis is localized to the obstructed lung segment. Obstruction ---> infection ---> damage bronchial walls ---> leading to weakening and dilation of bronchi Two processes are critical and intertwined in the pathogenesis of bronchiectasis: (1) obstruction (2) chronic persistent infection. Obstruction
 obstruction. (2) chronic persistent infection. Obstruction.")
39
Pathology, Gross 1) Lower lobes of bilateral lungs are more common, particularly left side 2) The airways may be dilated to as much as four times their usual diameter 3) The dilated bronchioles can be seen almost to the pleura. Grossly usually affects the lower lobes the most severe involvement is found in the more distal bronchi and bronchioles. The airways may be dilated to as much as four times their usual diameter (dilated bronchi and bronchioles )
 Lower lobes of bilateral lungs are more common, particularly left side 2) The airways may be dilated to as much as four times their usual diameter 3) The dilated bronchioles can be seen almost to the pleura. Grossly. usually affects the lower lobes. the most severe involvement is found in the more distal bronchi and bronchioles. The airways may be dilated to as much as four times their usual diameter (dilated bronchi and bronchioles )")
40
This is another form of obstructive lung disease known as bronchiectasis. Bronchiectasis occurs when there is obstruction or infection with inflammation and destruction of bronchi so that there is permanent dilation.Once the dilated bronchi are present, as seen here grossly in the mid lower portion of the lung, the patient has recurrent infections because of the stasis in these airways. Copius purulent sputum production with cough is typical.

41
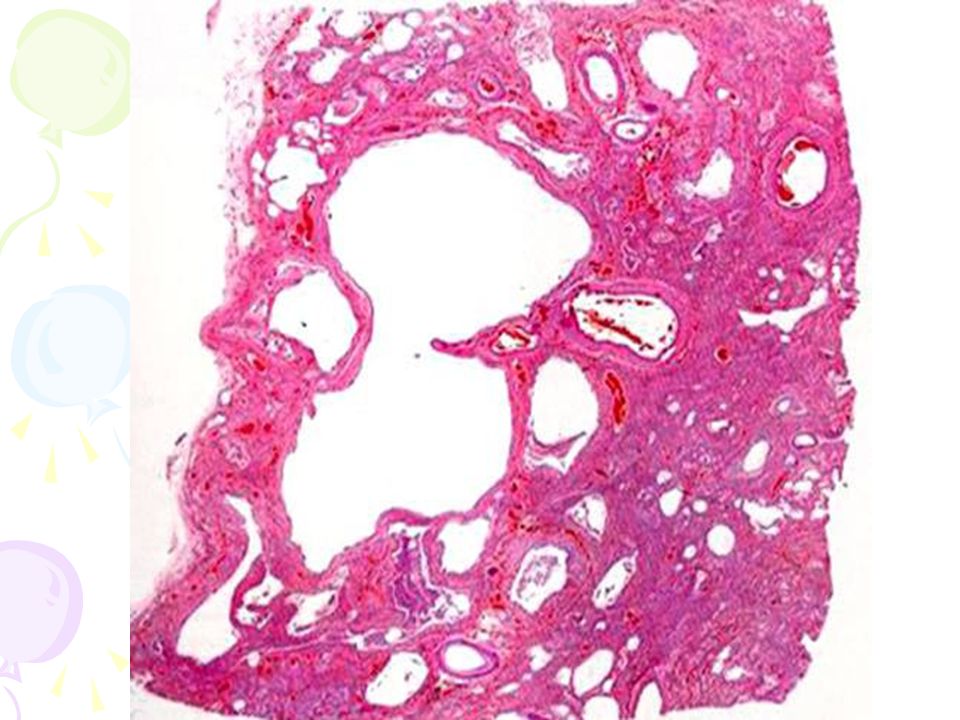
Pathology Destruction of the bronchial or bronchiolar walls
Histological Destruction of the bronchial or bronchiolar walls Acute and chronic inflammatory exudate within the walls of the bronchi and bronchioles Ulceration formation: the desquamation of lining epithelium cause extensive areas of ulceration. Fibrosis of the bronchial and bronchiolar walls (in chronic cases). Lung abscess.
. Lung abscess.")
43
Acute and chronic inflammation, ulcer, squamous metaplasia.
Smooth muscle, elastic tissue and cartilage are damaged, even disappear. Fibrosis of the bronchial and bronchiolar walls.

44
Clinical Features Cough Mucopurulent sputum Hemoptysis(咯血)
Finger-clubbing Dyspnoea Clubbing:杵状指 Usually, the lower lobes are affected Leading to pooling of bronchial secretions with further infection. Symptoms are chronic cough with expectoration of large quantities of foul-smelling sputum, sometimes flecked with blood. Patients may have finger-clubbing because of anoxic Respiratory tract inflammation is very usual, sometimes the metastatic abscess may happen, for example, brain abscesses. severe, persistent cough sputum (mucopurulent, sometimes fetid). The sputum may contain flecks of blood; frank hemoptysis can occur. Clubbing of the fingers may develop. In cases of severe, with hypoxemia, hypercapnia, pulmonary hypertension, and (rarely) cor pulmonale.
. The sputum may contain flecks of blood; frank hemoptysis can occur. Clubbing of the fingers may develop. In cases of severe, with hypoxemia, hypercapnia, pulmonary hypertension, and (rarely) cor pulmonale.")
45
Clubbing Normal For the normal finger, the angle is less than 160
For the finger-clubbing, the angle is more than 180

46
Complications Pneumonia, lung abscess Emphysema Remote abscesses
Pulmonary hypertension Chronic cor pulmonale

48
Chronic cor pulmonale 慢性肺源性心脏病
A heart disease results from chronic lung diseases, chest or pulmonary vascular diseases. Pulmonary hypertension(肺动脉高压). Thickened right ventricle(右心室肥厚).
. Thickened right ventricle(右心室肥厚).")
49
A. Etiology and pathogenesis
Recurrent pulmonary emboli Heart disease: Chronic obstructive or interstitial lung disease:

50
Key Key Chronic obstuctive pulmonary disease
Disorders affecting chest movement Abnormalities of the pulmonary vasculature Pulmonary arteriolar constriction Pulmonary vascular bed Key Key Pulmonary hypertension* Right ventricle hypertrophy

51
B. Pathology Lung Existed lung diseases:
Medium-sized muscular arteries: proliferation of myo-intimal cells and smooth muscle cells, causing thickening of the intima and media with narrowing of the lumina Smaller arteries and arterioles: thickening, medial hypertrophy, and reduplication of the internal and external elastic membranes. For the lungs, there two parts disorders: 1\ chronic obstructive pulmonary disease, including chronic bronchitis, emphysema, asthma, bronchiectasis,etc.----diffuse pulmonary fibrosis, or severe emphysema and chronic bronchitis, points to chronic hypoxia as the initiating event. 2\ vascular disorders:

52
The wall is thickened The proliferation of smooth muscle, fibrosis.

54
B. Pathology Heart* Right ventricle hypertrophy:
More than 1 cm in thickness (normal cm) More than 500—700 gm The right ventricle and atrium may be dilated when failure occurs The right ventricle is thickened, the thickness of the right ventricular wall may be exceeding more than 0.5cm, under the pulmonary artery valve 2 cm. it is the diagnostic criterion. the weight of the heart is increased, 500—700gm. The right ventricular wall may reach a thickness of more than 1.5 When ventricular failure develops, the right ventricle and atrium may also be dialted.
 More than 500—700 gm. The right ventricle and atrium may be dilated when failure occurs. The right ventricle is thickened, the thickness of the right ventricular wall may be exceeding more than 0.5cm, under the pulmonary artery valve 2 cm. it is the diagnostic criterion. the weight of the heart is increased, 500—700gm. The right ventricular wall may reach a thickness of more than 1.5. When ventricular failure develops, the right ventricle and atrium may also be dialted.")
55
The right ventricle is thickened, the thickness of the right ventricular wall may be exceeding more than 0.5cm, under the pulmonary artery valve 2 cm. it is the diagnostic criterion. the weight of the heart is increased, 500—700gm. The right ventricular wall may reach a thickness of more than 1.5

56
Clinical features Cyanosis: hypoxemia Pulmonary encephalopathy(肺性脑病)
Right-sided congestive heart failure--- congestion, edema of lower extremities, palpitation, ascites 1\dark purple can be seen in the lip, skin , the finger, because of the hypoxemia, the air exchange have been stopped by the chronic lung diseases. 2\when hypoxemia develops, the central nerve system will be damaged, the sleepiness may occurs. 3\

57
SUMMARY COPD: Chronic bronchitis* Asthma Pulmonary emphysema*
Bronchiectasis Pulmonary hypertension Chronic cor pulmonale*

58
65, woman, cough with purulent sputum after catching cold 15 years ago.
She developed cough and expectoration of white spumy sputum every winter and spring. Since 3 years ago, she felt breath shortness and palpitation(心悸) after physical labor.
 after physical labor.")
59
Pitting edema(水肿) occurred repeatedly on her lower limbs for 2 years.
Two months ago after catching cold, she developed fever, cough with purulent sputum, palpitation, breath shortness, and abdominal distension(膨隆), and could not lie down.
, and could not lie down.")
60
Physical examination:
T: 37.6℃, HR:102 times/min, R: 30 times/min. Chronic sickness appearance, up-straight sit breathing(端坐呼吸), sleepiness, dark purple lip and skin, cervix venous engorgement (颈静脉怒张)
, sleepiness, dark purple lip and skin, cervix venous engorgement (颈静脉怒张)")
61
Chest: Barrel-shape chest, hyper-resonance(过清音) to percussion(叩诊), scattered dry and moist rales(啰音). Abdomen: Abdominal bulge, a large amount of ascites(腹水), the liver is hard with the rim under the rib 7.8 cm, lower limbs show pitting edema.
, the liver is hard with the rim under the rib 7.8 cm, lower limbs show pitting edema.")
62
Questions 1. what is the pathological diagnosis of the patient?
2. how to explain the process of the development of the diseases about the patient.

63
Pathological diagnosis
Chronic bronchitis Emphysema Chronic cor pulmonale complicated with: (1) right heart failure---- liver congestion, lower limbs edema, ascites (2) pulmonary encephalopathy
 right heart failure---- liver congestion, lower limbs edema, ascites. (2) pulmonary encephalopathy.")
64
The relationship Chronic bronchitis---- emphysema----
chronic cor pulmonale---- right heart failure and pulmonary encephalopathy.

65
See you next time!

Similar presentations








>")








>")

Asthma 2)COPD 3)Comparison.>")



>")
