Download presentation
Presentation is loading. Please wait.

1
Anaphylactic Shock in General Anesthesia Presented by R1 顏郁軒 2003/3/18

2
General Data (1) 80 y/o, Female, about 70 kgw Hx of HTN Hx of right knee & wrist fracture s/p op, gall stone s/p op, uterus prolapse s/p op No any complication was noted after general anesthesia No drug allergy history
 80 y/o, Female, about 70 kgw Hx of HTN Hx of right knee & wrist fracture s/p op, gall stone s/p op, uterus prolapse s/p op No any complication was noted after general anesthesia No drug allergy history")
3
General Data (2) Fell down on 92/3/2 ; right distal radial fracture was impressed and operation was arranged General anesthesia was done. Induction with Fentanyl 100 ug, Pentothal 275 mg, SCC 100 mg, Cis-atracurium 4 mg, Xylocaine 100 mg

4
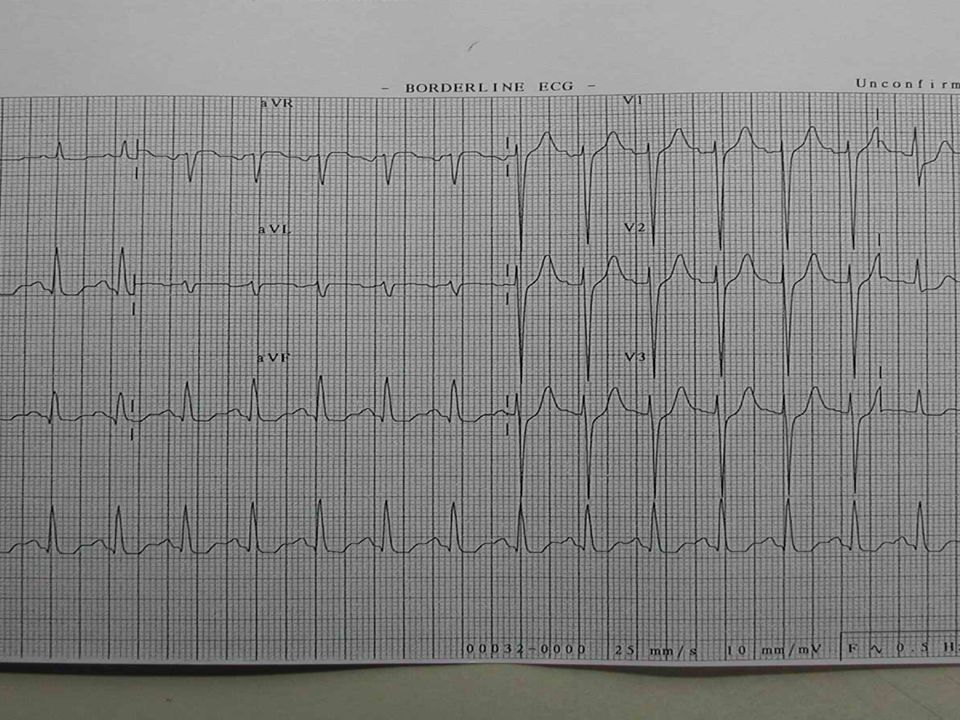
General Data (3) About 15 mins later, tachycardia about 130 ~ 140, low end tidal CO2 (30+ 10+) and high airway pressure were noted. Pulse : weak and then impalpable Breathing sound : bil decreased EKG : ST depression over lead II CPR was done Bosmine infusion Set A-line, but failed

5
General Data (4) About 3 mins later, pulse was returned and A-line was set successfully then. Erythematous change over trunk & four limbs were noted BP=110/65, PR =148 Transferred to SICU for further treatment and evaluation

7
What Happened ? D/D : AMI, Anaphylaxis, Pneumothorax, Pulmonary embolism Time sequence of drug administration Hints over physical examination How to explain the EKG change

8
Lab Data Series EKG was F/U Cardiac enzyme F/U 3/2 3/2 3/3 CK/CKMB 61/32.1 64/13.3 73/4.4 Troponin-I 0.1 3.3 7.3 Con’s returned at that night, and endo was removed on the next day smoothly.

10
Operation was done on 3/12 Anesthesia with IVG was performed Agent : Fentanyl 100 ug, Propofol infusion No any complication was noted during anesthesia The post operative condition was good, and then discharged smoothly.

11
Anaphylaxis during anesthesia (1) Allergy,anaphylaxis,and general anesthesia Immunology and Allergy Clinics of North America Volume 21 Number 4 November 2001 Anaphylaxis. What is Monitored to Make a Diagnosis? How is Therapy Monitored? Anesthesiology Clinics of North America Volume 19 Number 4 December 2001

12
Anaphylaxis during anesthesia(2) Definition Anaphylaxis : rapid, generalized immunologically mediated events involving an antigen-specific IgE-mediated mechanism that occur after exposure to foreign substances in previously sensitized persons Anaphylactoid reaction : not mediated by way of the IgE antibody and prior exposure is not necessary
 Definition Anaphylaxis : rapid, generalized immunologically mediated events involving an antigen-specific IgE-mediated mechanism that occur after exposure to foreign substances in previously sensitized persons Anaphylactoid reaction : not mediated by way of the IgE antibody and prior exposure is not necessary")
13
Anaphylaxis during anesthesia(3) The incidence of anaphylaxis in GA is about 1:5000 to 1: 20000 and with a mortality rate of up to 6% Mechanism : 1. Specific IgE cross-linked by allergen (drug) 2. Complement activation by specific IgG or IgM binding to antigen (drug) 3. Direct complement activation by way of the alternate pathway 4. Direct activation of mast cells or basophils
 2. Complement activation by specific IgG or IgM binding to antigen (drug) 3. Direct complement activation by way of the alternate pathway 4. Direct activation of mast cells or basophils.")
14
CAUSES OF ANAPHYLAXIS AND ANAPHYLACTOID REACTIONS DURING ANESTHESIA Causes Rate of Reaction (%) Muscle relaxants61.6 Latex16.6 Antibiotics8.3 Hypnotics5.1 Colloids3.1 Opioids2.7 Other (aprotinin, ethylene oxide, local anesthetics) 2.6 Data from French survey by Perioperative Anaphylactoid Reactions Study Group; 1648 patients, July 1994 to December 1996.
 Muscle relaxants61.6 Latex16.6 Antibiotics8.3 Hypnotics5.1 Colloids3.1 Opioids2.7 Other (aprotinin, ethylene oxide, local anesthetics) 2.6 Data from French survey by Perioperative Anaphylactoid Reactions Study Group; 1648 patients, July 1994 to December 1996.")
15
RECOGNITION OF ANAPHYLAXIS DURING ANESTHESIA SystemVital Sign ChangesOther SignsSymptoms Pulmonary Increased respiratory rateStridor (laryngeal edema), wheezing (bronchospasm), coughing, sneezing, decreased pulmonary compliance, pulmonary edema, respiratory failure Dyspnea, chest discomfort Cardiovascular Increased blood pressureDecreased systemic vascular resistance, dysrhythmias, pulmonary hypertension, cardiac arrest Retrosternal pain Increased heart rate Cutaneous Increased skin temperature (redistribution of blood) Urticaria (hives), flushing, periorbital edema, perioral edema diaphoresis Itching, burning Neurologic NonspecificDisorientation, loss of consciousness Dizziness, light-headedness, malaise Gastrointestinal NonspecificVomiting, diarrheaNausea, abdominal pain
, wheezing (bronchospasm), coughing, sneezing, decreased pulmonary compliance, pulmonary edema, respiratory failure Dyspnea, chest discomfort Cardiovascular Increased blood pressureDecreased systemic vascular resistance, dysrhythmias, pulmonary hypertension, cardiac arrest Retrosternal pain Increased heart rate Cutaneous Increased skin temperature (redistribution of blood) Urticaria (hives), flushing, periorbital edema, perioral edema diaphoresis Itching, burning Neurologic NonspecificDisorientation, loss of consciousness Dizziness, light-headedness, malaise Gastrointestinal NonspecificVomiting, diarrheaNausea, abdominal pain")
16
Treatment (1) Airway maintenance, 100% oxygen administration, intravascular volume expansion, and epinephrine
 Airway maintenance, 100% oxygen administration, intravascular volume expansion, and epinephrine")
17
Treatment (2) Initial therapy 1. Stop administration of antigen 2. Maintain airway with 100% oxygen 3. Discontinue all anesthetic agents 4. Start intravascular volume expansion (2–4 L of crystalloid with hypotension) 5. Administer epinephrine (5–10 μg intravenous initial bolus with hypotension, titrated as needed; 0.1–0.5 mg intravenously with cardiovascular collapse)
 5. Administer epinephrine (5–10 μg intravenous initial bolus with hypotension, titrated as needed; 0.1–0.5 mg intravenously with cardiovascular collapse).")
18
Treatment (3) Secondary treatment 1. Antihistamines (0.5–1 mg/kg diphenhydramine) 2. Catecholamine infusions (starting doses: epinephrine, 5–10 μg/min; norepinephrine, 5–10 μg/min, as an infusion, titrated as needed) 3. Bronchodilators (inhaled albuterol or terbutaline with bronchospasm) 4. Corticosteroids (0.25–1 g hydrocortisone; alternating 1–2 g methylprednisolone) 5. Sodium bicarbonate rarely needed (0.5–1 mEq/kg with persistent hypotension and acidosis refractory to volume repletion and epinephrine) 6. Airway evaluation (before extubation)
 3. Bronchodilators (inhaled albuterol or terbutaline with bronchospasm) 4. Corticosteroids (0.25–1 g hydrocortisone; alternating 1–2 g methylprednisolone) 5. Sodium bicarbonate rarely needed (0.5–1 mEq/kg with persistent hypotension and acidosis refractory to volume repletion and epinephrine) 6. Airway evaluation (before extubation).")
19
An anaphylactic reaction possibly associated with an intraoperative coronary artery spasm during general anesthesia Journal of Clinical Anesthesia Volume 13 Number 3 May 2001

20
A 72 y/o male with choledocholithiasis HTN & smoking, no allergy history Epidural and GA with Fentanyl, vecuronium and propofol were done Hypotension ( 60/42 mmHg ) and tachycardia ( 122 beats /mins ) after antibiotics given (Cefa)
 and tachycardia ( 122 beats /mins ) after antibiotics given (Cefa)")
21
ST elevation over lead II, III, AVF and V6 PE : flush over neck and chest Anaphylaxis with coronary spasm was considered Tx with Epinephrine and solu- medrol(500 mg) ; 5 mins later BP elevation and ST returned normal
 ; 5 mins later BP elevation and ST returned normal")
22
histamine causes dilation in both epicardial and resistance coronary arteries that are free of atherosclerosis histamine induces profound vasoconstriction in segments of coronary arteries with a defective endothelial vasodilation mechanism

23
coronary artery spasm in their case may be explained by an increased histamine level and an impaired endothelial coronary vasodilation mechanism

24
the adventitial mast cells of the coronary artery may play an important role in the pathogenesis of coronary artery spasm

25
degranulated mast cells are increased in the adventitia of the coronary artery segments with ruptured plaque that are responsible for MI, suggesting histamine and other vasoactive substances released from the adventitial mast cells may locally provoke coronary artery spasm

26
Thanks for your Attention !!

Similar presentations

















 leading to damage Require sensitizing dose(s) Introduction to Lab Ex. 24:>")
 leading to inadequate oxygen delivery to tissues.>")
, MD (Acu), Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi medical college and.>")
