Download presentation
Presentation is loading. Please wait.

1
Data Linkages Between Birth Defects Registry and EHDI in Michigan Rupali Patel, Glenn Copeland, Yasmina Bouraoui, Joan Ehrhardt, Erin Estrada Michigan Department of Community Health Division of Epidemiology and Early Hearing Detection and Intervention Program Division of Epidemiology and Early Hearing Detection and Intervention Program

2
Faculty Disclosure Information In the past 12 months, I have not had a significant financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in my presentation. In the past 12 months, I have not had a significant financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in my presentation. This presentation will (not) include discussion of pharmaceuticals or devices that have not been approved by the FDA or if you will be discussing unapproved or "off-label" uses of pharmaceuticals or devices. This presentation will (not) include discussion of pharmaceuticals or devices that have not been approved by the FDA or if you will be discussing unapproved or "off-label" uses of pharmaceuticals or devices.
 of the product(s) or provider(s) of the service(s) that will be discussed in my presentation. This presentation will (not) include discussion of pharmaceuticals or devices that have not been approved by the FDA or if you will be discussing unapproved or off-label uses of pharmaceuticals or devices. This presentation will (not) include discussion of pharmaceuticals or devices that have not been approved by the FDA or if you will be discussing unapproved or off-label uses of pharmaceuticals or devices..")
3
Background: Estimated one to three out of every 1,000 infants are born with hearing loss Estimated one to three out of every 1,000 infants are born with hearing loss Approximately 8,000 to 16,000 of the infants born annually in the United States have some degree of hearing loss (HL), a commonly occurring congenital anomaly. Approximately 8,000 to 16,000 of the infants born annually in the United States have some degree of hearing loss (HL), a commonly occurring congenital anomaly. Leads to significant delays in speech and language development Leads to significant delays in speech and language development Early detection and intervention can improve the development of language and cognitive skills. Early detection and intervention can improve the development of language and cognitive skills.
, a commonly occurring congenital anomaly. Leads to significant delays in speech and language development Leads to significant delays in speech and language development Early detection and intervention can improve the development of language and cognitive skills. Early detection and intervention can improve the development of language and cognitive skills..")
4
Background Michigans Early Hearing Detection and Intervention (EHDI) program Michigans Early Hearing Detection and Intervention (EHDI) program Established in 1998 Established in 1998 Identifies all infants at birth with hearing loss Identifies all infants at birth with hearing loss All infants identified at birth with hearing loss should be also reported to the Michigan Birth Defects Registry (MBDR). All infants identified at birth with hearing loss should be also reported to the Michigan Birth Defects Registry (MBDR). Confidential statewide passive surveillance of birth defects Confidential statewide passive surveillance of birth defects Identifies all infants at birth with hearing loss Identifies all infants at birth with hearing loss Those identified in the MBDR may not be included in the EHDI program Those identified in the MBDR may not be included in the EHDI program However, hearing loss cases annually identified and reported to MBDR may not have been diagnosed by the early hearing screening. However, hearing loss cases annually identified and reported to MBDR may not have been diagnosed by the early hearing screening. It is important that these children are referred to Michigans EHDI Program, to assure that they receive the appropriate care. It is important that these children are referred to Michigans EHDI Program, to assure that they receive the appropriate care.
. Confidential statewide passive surveillance of birth defects Confidential statewide passive surveillance of birth defects Identifies all infants at birth with hearing loss Identifies all infants at birth with hearing loss Those identified in the MBDR may not be included in the EHDI program Those identified in the MBDR may not be included in the EHDI program However, hearing loss cases annually identified and reported to MBDR may not have been diagnosed by the early hearing screening. However, hearing loss cases annually identified and reported to MBDR may not have been diagnosed by the early hearing screening. It is important that these children are referred to Michigans EHDI Program, to assure that they receive the appropriate care. It is important that these children are referred to Michigans EHDI Program, to assure that they receive the appropriate care..")
5
Objectives: The objective of this study is to explore the hearing loss rates reported to MBDR and understand the use and value of the linked data with EHDI. The objective of this study is to explore the hearing loss rates reported to MBDR and understand the use and value of the linked data with EHDI.

6
Methods: A data set of 1997-2003 hearing loss cases reported to MBDR was created for this study. A data set of 1997-2003 hearing loss cases reported to MBDR was created for this study. Cases within the MBDR were linked with confirmed cases of hearing loss in newborns from the Early Hearing Detection and Intervention (EHDI) program that were identified beginning with 1997. Cases within the MBDR were linked with confirmed cases of hearing loss in newborns from the Early Hearing Detection and Intervention (EHDI) program that were identified beginning with 1997. The analysis was restricted to unspecified hearing loss (ICD9 Code 383.9). The analysis was restricted to unspecified hearing loss (ICD9 Code 383.9). The analysis did not include did not include Congenital Anomalies of the Ear, Face, and Neck (ICD9 Codes 744.0 - 744.49) The analysis did not include did not include Congenital Anomalies of the Ear, Face, and Neck (ICD9 Codes 744.0 - 744.49) The prevalence rates were calculated per 10,000 live births and trend analysis was conducted by using SAS 9.1 software. The prevalence rates were calculated per 10,000 live births and trend analysis was conducted by using SAS 9.1 software.
 program that were identified beginning with Cases within the MBDR were linked with confirmed cases of hearing loss in newborns from the Early Hearing Detection and Intervention (EHDI) program that were identified beginning with The analysis was restricted to unspecified hearing loss (ICD9 Code 383.9). The analysis was restricted to unspecified hearing loss (ICD9 Code 383.9). The analysis did not include did not include Congenital Anomalies of the Ear, Face, and Neck (ICD9 Codes ) The analysis did not include did not include Congenital Anomalies of the Ear, Face, and Neck (ICD9 Codes ) The prevalence rates were calculated per 10,000 live births and trend analysis was conducted by using SAS 9.1 software. The prevalence rates were calculated per 10,000 live births and trend analysis was conducted by using SAS 9.1 software..")
9
Prevalence of Hearing Loss at Age of Diagnosis Other/ Unknown 18.0% 1mnth-1 yr 43.0% <1 month 15.7% 1-2 yr 23.3%

10
Cases of Hearing Loss stratified by Age at Diagnosis 0% 20% 40% 60% 80% <1 month1month-1 year1-2 yearOther/Unknown HL Cases not in EHDIHL Cases in EHDI

11
Cases Born in Level 3 Hospital Stratified by EHDI Status EHDI Cases 29.3% Cases Not In EHDI 70.7%

12
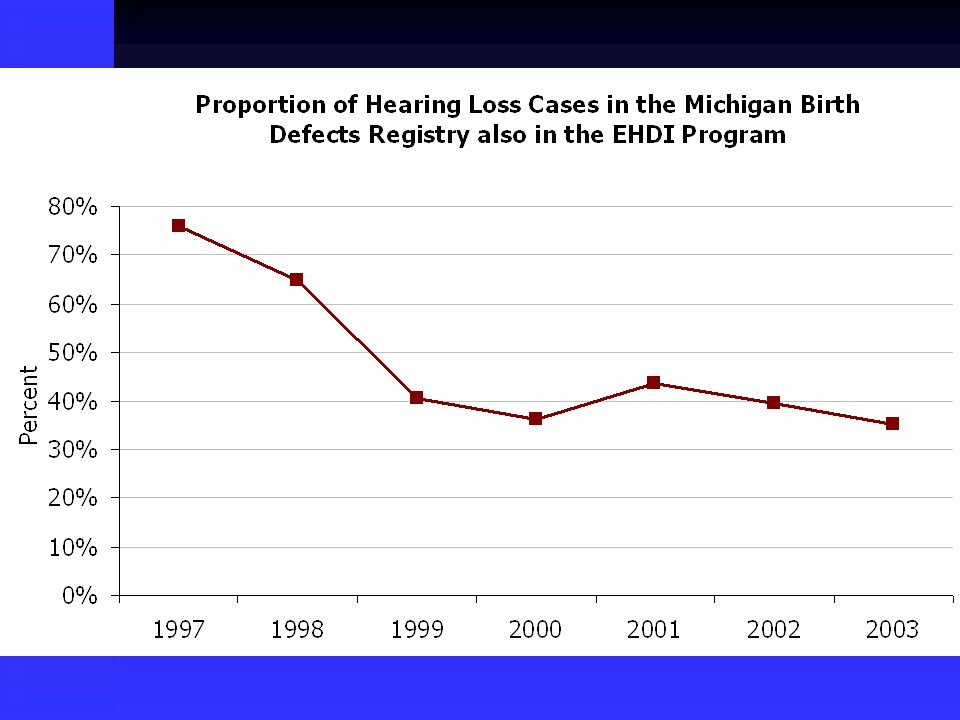
Results There were 2,368 unspecified hearing loss cases identified and reported to MBDR between 1997- 2003 with an overall prevalence rate of 25.5/10,000 live births. There were 2,368 unspecified hearing loss cases identified and reported to MBDR between 1997- 2003 with an overall prevalence rate of 25.5/10,000 live births. About 40.0% of the cases were reported to the Registry by the EHDI program. About 40.0% of the cases were reported to the Registry by the EHDI program. Overall the percentage of cases referred to MBDR by the EHDI program decrease over the study period, from 75.9% in 1997 to 35.2% in 2003. Overall the percentage of cases referred to MBDR by the EHDI program decrease over the study period, from 75.9% in 1997 to 35.2% in 2003.

13
Results, cont. Approximately 15.7% of unspecified hearing deficiency cases in the MBDR were diagnosed within one month after birth, with 31.7% of these also reported in EHDI. Approximately 15.7% of unspecified hearing deficiency cases in the MBDR were diagnosed within one month after birth, with 31.7% of these also reported in EHDI. The highest percentage of cases were diagnosed between the ages of one month to one year at 43.0%, with 46.1% also reported in EHDI. The highest percentage of cases were diagnosed between the ages of one month to one year at 43.0%, with 46.1% also reported in EHDI. When further stratified by the level of care, 59.7% were born at level 3 birthing hospitals suggesting that the majority of infants with hearing loss were from high-risk pregnancies. When further stratified by the level of care, 59.7% were born at level 3 birthing hospitals suggesting that the majority of infants with hearing loss were from high-risk pregnancies.

14
Conclusion Less than half of the unspecified hearing loss cases were also in the EHDI program Less than half of the unspecified hearing loss cases were also in the EHDI program Further analysis should explore the risk factors for developing evidence based prevention strategies Further analysis should explore the risk factors for developing evidence based prevention strategies

15
Public Health Implications: Regardless of improvement in Michigans EHDI program to detect HL at birth, the follow up reporting is still poor and limits the ability to determine access to and participation in early intervention services. Regardless of improvement in Michigans EHDI program to detect HL at birth, the follow up reporting is still poor and limits the ability to determine access to and participation in early intervention services. Collaboration and data sharing between MBDR and EHDI data systems will provide more accurate information on the incidence of diagnosed hearing loss. Collaboration and data sharing between MBDR and EHDI data systems will provide more accurate information on the incidence of diagnosed hearing loss. In addition, it will assure that every child with hearing loss will be referred to the appropriate intervention services. In addition, it will assure that every child with hearing loss will be referred to the appropriate intervention services.

16
Limitations Under reporting - Lack of consistent reporting from different hospitals and other healthcare facilities Under reporting - Lack of consistent reporting from different hospitals and other healthcare facilities Over reporting Over reporting Possible false diagnoses Possible false diagnoses Entered into MBDR because initial screen shows hearing loss, but later screen determines not a hearing loss case Entered into MBDR because initial screen shows hearing loss, but later screen determines not a hearing loss case Lack of interstate exchange Lack of interstate exchange Data manipulation Data manipulation MBDR is constantly cleaned and updated MBDR is constantly cleaned and updated May not get the same results if study done at a different time May not get the same results if study done at a different time

17
Hearing Loss cases within the MBDR Birth Year All cases EHDI only EHDI and other source Other source only Other Source only in CSHCS Total23706124341324385 199714280273516 1998261122479224 19993671044421976 20004471006428390 20014247810723966 2002391758023671 2003338536522042

18
Explanation of 2002 data 236 cases in MDBR from other source only 236 cases in MDBR from other source only 227 were unspecified hearing loss code (ICD-9 CM 389.9) 227 were unspecified hearing loss code (ICD-9 CM 389.9) EHDI found: 39% Passed initial hearing screening 39% Passed initial hearing screening 23% Passed rescreen hearing screen 23% Passed rescreen hearing screen 5% had a diagnostic outcome of Within Normal Limits 5% had a diagnostic outcome of Within Normal Limits 14% of bilateral/unilateral failed initials screening and did not have follow-up 14% of bilateral/unilateral failed initials screening and did not have follow-up 2% were incomplete screens with no follow- up 2% were incomplete screens with no follow- up 13% had no information in the EHDI system 13% had no information in the EHDI system 1% were identified as having a hearing loss in the EHDI system 1% were identified as having a hearing loss in the EHDI system
 227 were unspecified hearing loss code (ICD-9 CM 389.9) EHDI found: 39% Passed initial hearing screening 39% Passed initial hearing screening 23% Passed rescreen hearing screen 23% Passed rescreen hearing screen 5% had a diagnostic outcome of Within Normal Limits 5% had a diagnostic outcome of Within Normal Limits 14% of bilateral/unilateral failed initials screening and did not have follow-up 14% of bilateral/unilateral failed initials screening and did not have follow-up 2% were incomplete screens with no follow- up 2% were incomplete screens with no follow- up 13% had no information in the EHDI system 13% had no information in the EHDI system 1% were identified as having a hearing loss in the EHDI system 1% were identified as having a hearing loss in the EHDI system")
19
Benefits of Matching Data Identify false positive cases Identify false positive cases Verify the validity of the data Verify the validity of the data Potential to follow-up on cases in either MDBR and/or EDHI Potential to follow-up on cases in either MDBR and/or EDHI

20
Contact: Michigan Department of Community Yasmina Bouraoui, MPH Yasmina Bouraoui, MPH EHDI Coordinator EHDI Coordinator Bouraouiy@mi.gov Bouraouiy@mi.govBouraouiy@mi.gov Erin Estrada, BA Erin Estrada, BA Data Analyst Data Analyst Estradae@michigan.gov Estradae@michigan.govEstradae@michigan.gov

Similar presentations