Download presentation
Presentation is loading. Please wait.

1
Session 5

2
Case

14
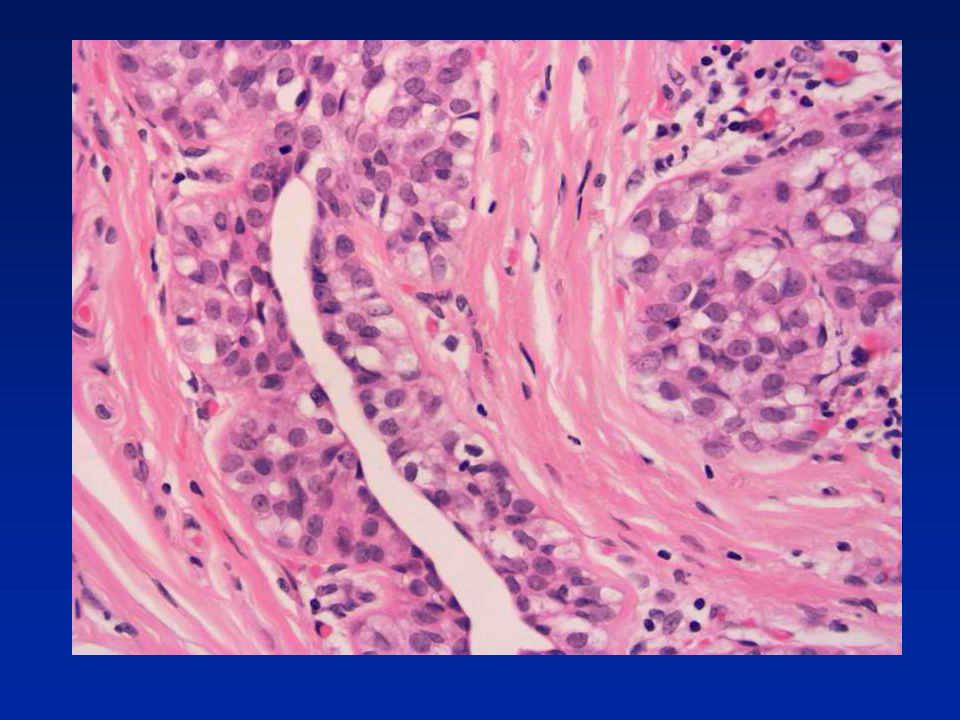
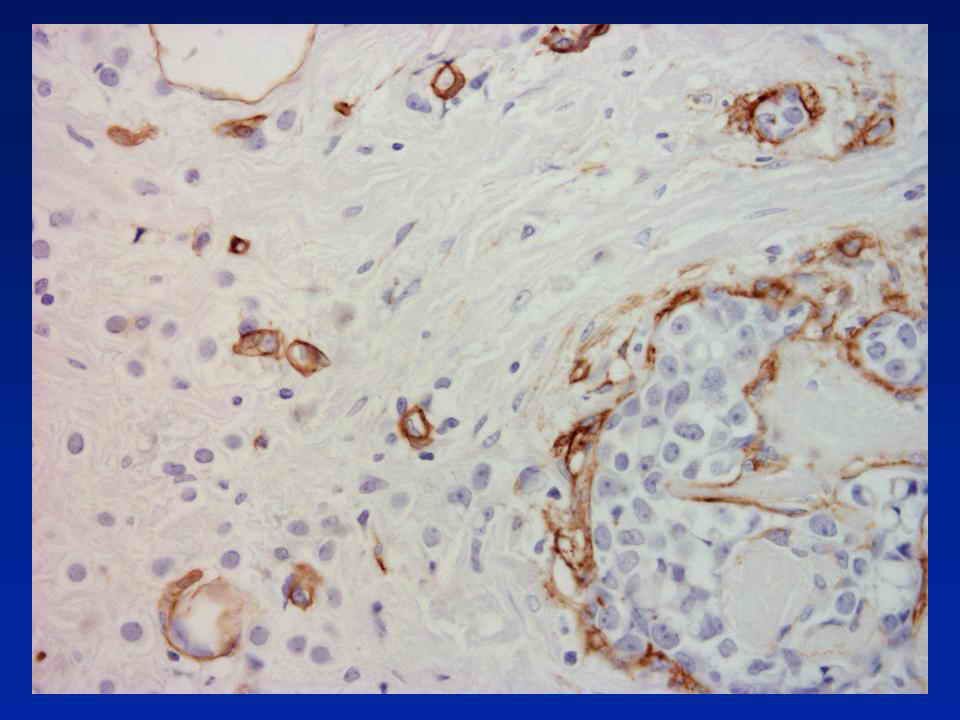
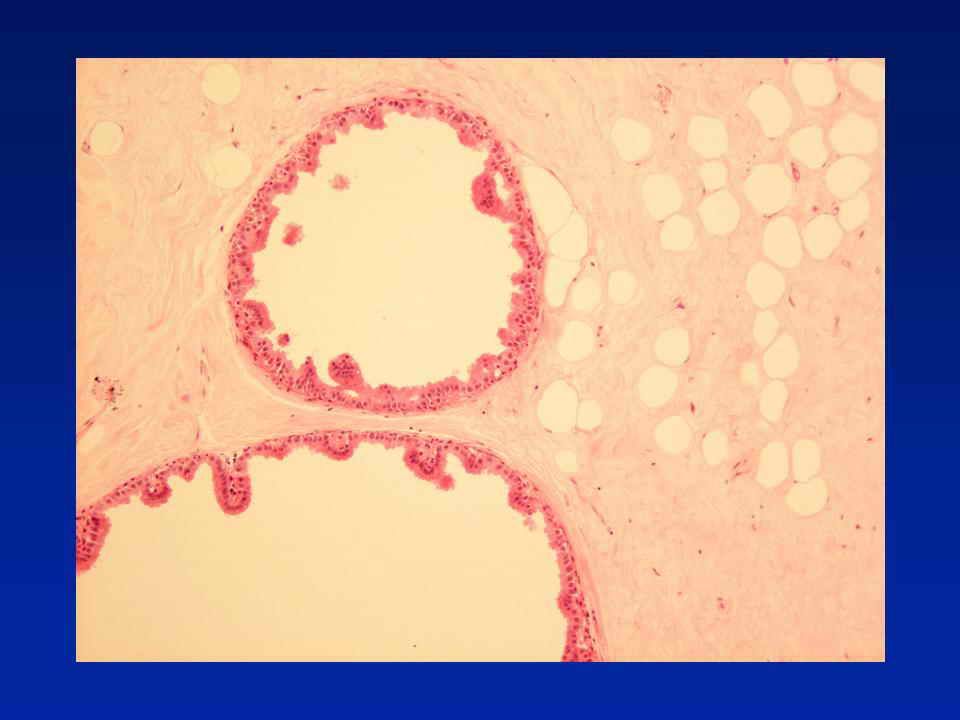
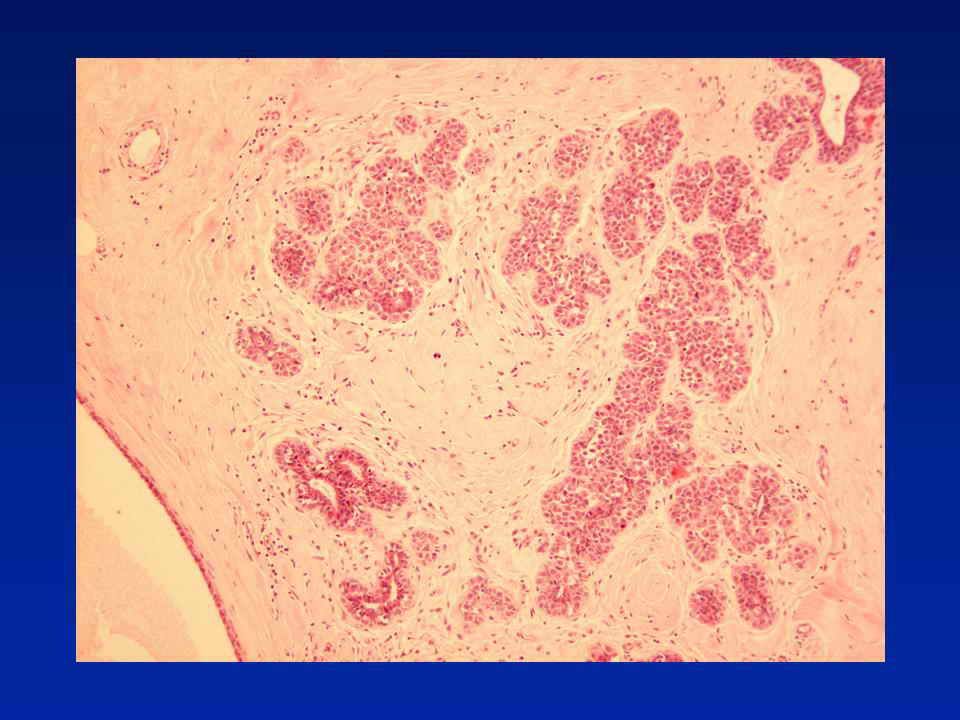
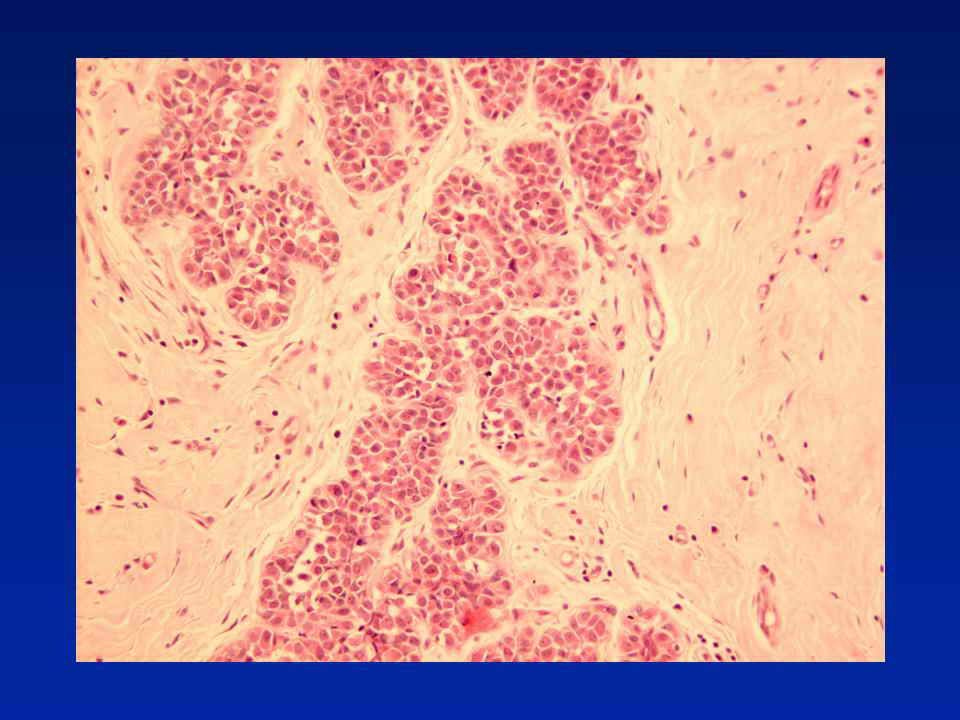
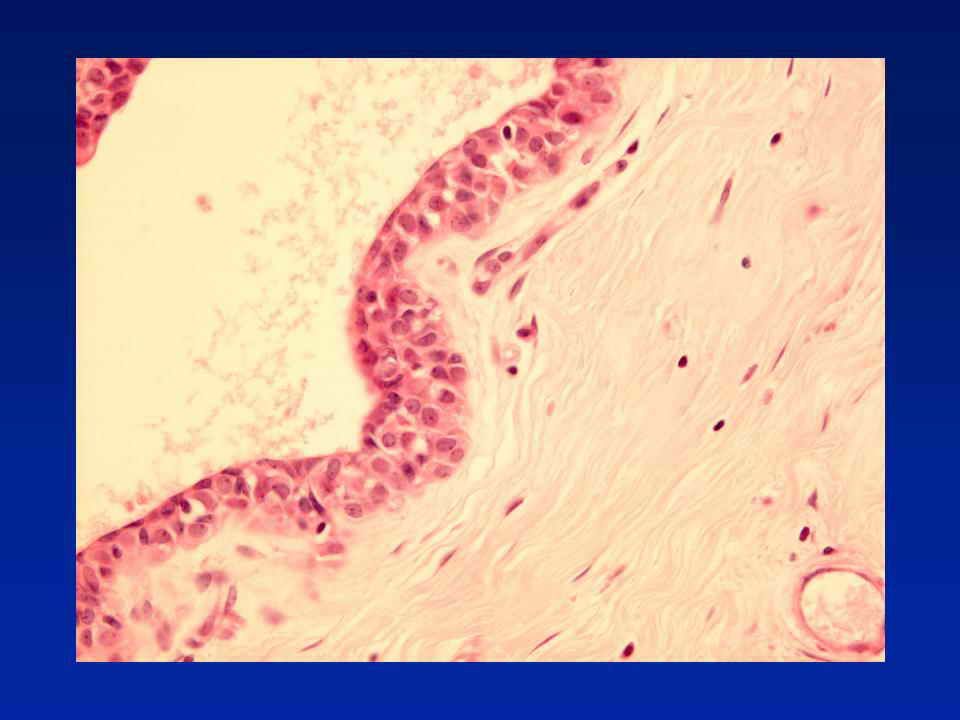
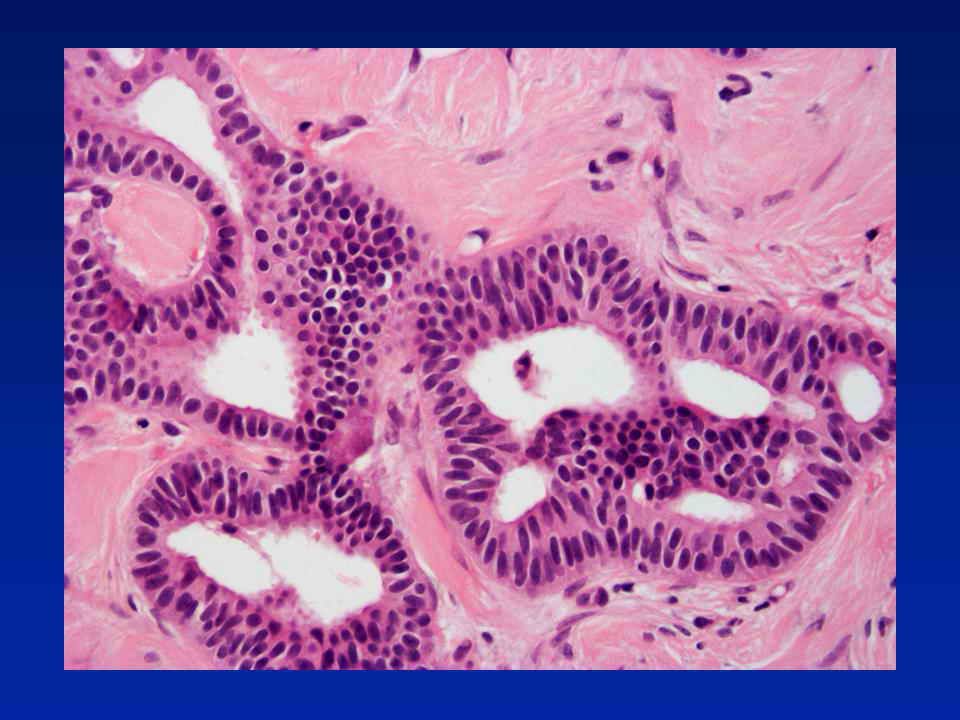
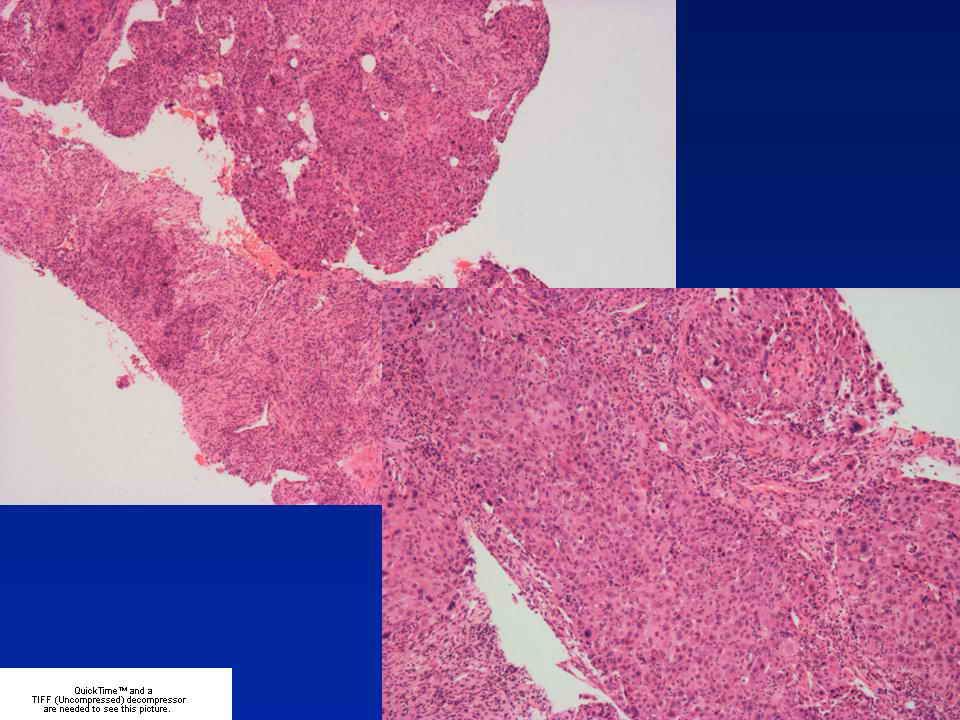
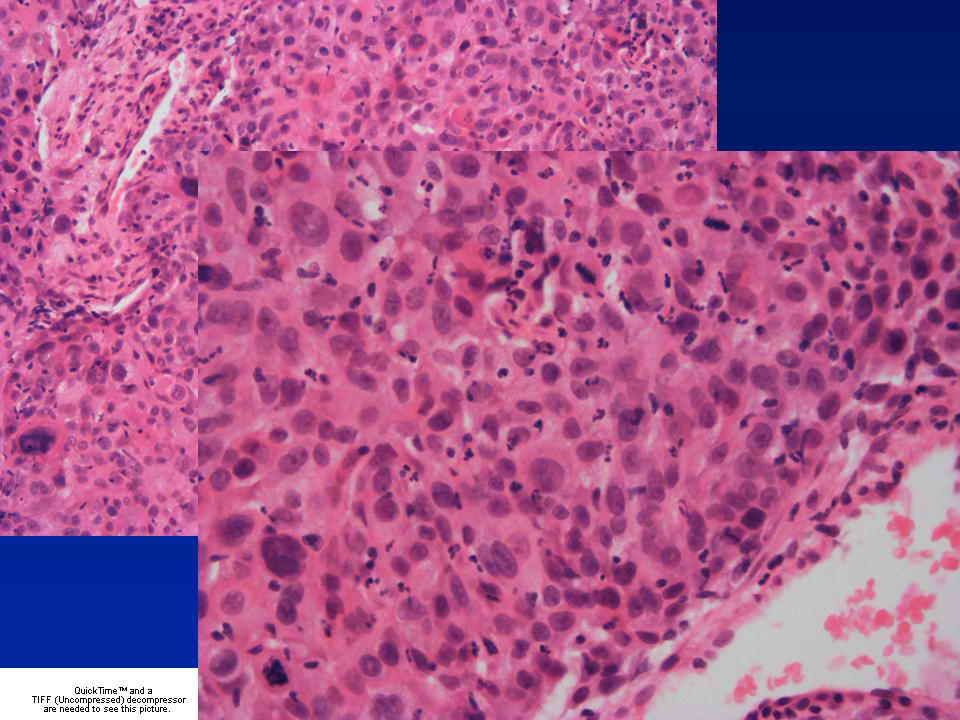
Diagnosis - Sclerosing adenosis with lobular neoplasia. No invasion in images provided.

17
Update - Risk with LISN Meta-analysis 9 studies of 228 patients 15% ipsilateral, 9% contralateral carcinoma Ipsilateral 3x more likely than contralateral A “model of premalignancy for ALH intermediate between a local precursor and a generalised risk for both breasts” Page DL. Lancet. 2003;361:125-9

18
Is there a sub-group of pre-invasive LCIS? LCIS with Microinvasion 6 LCIS with microinvasion described Nemoto T et al. J Surg Oncol 1998; 67; 41-46

19
Case 19

30
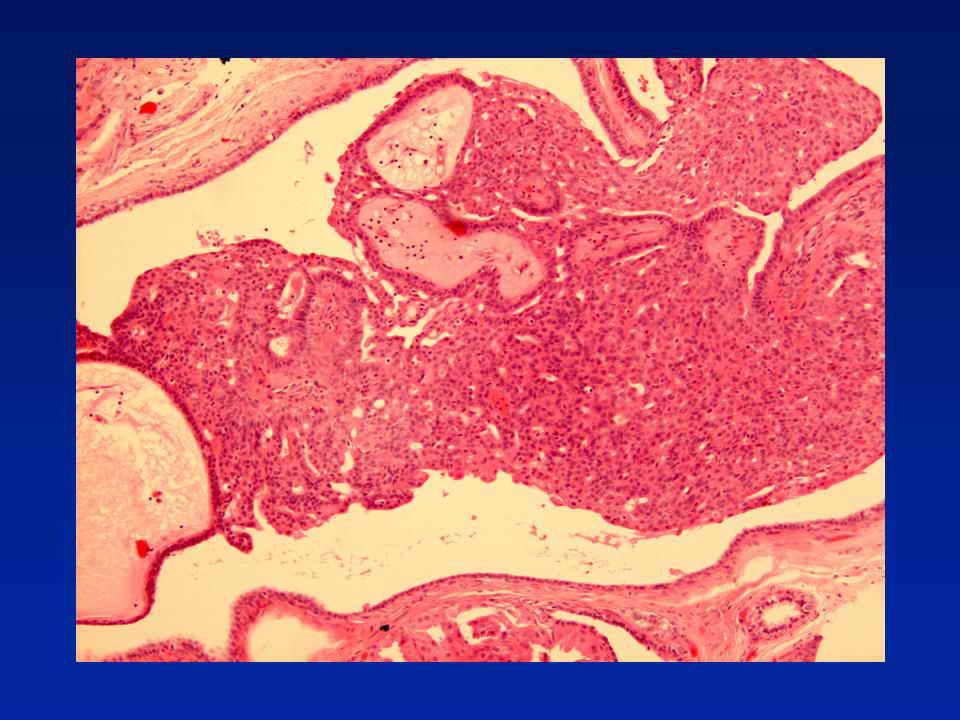
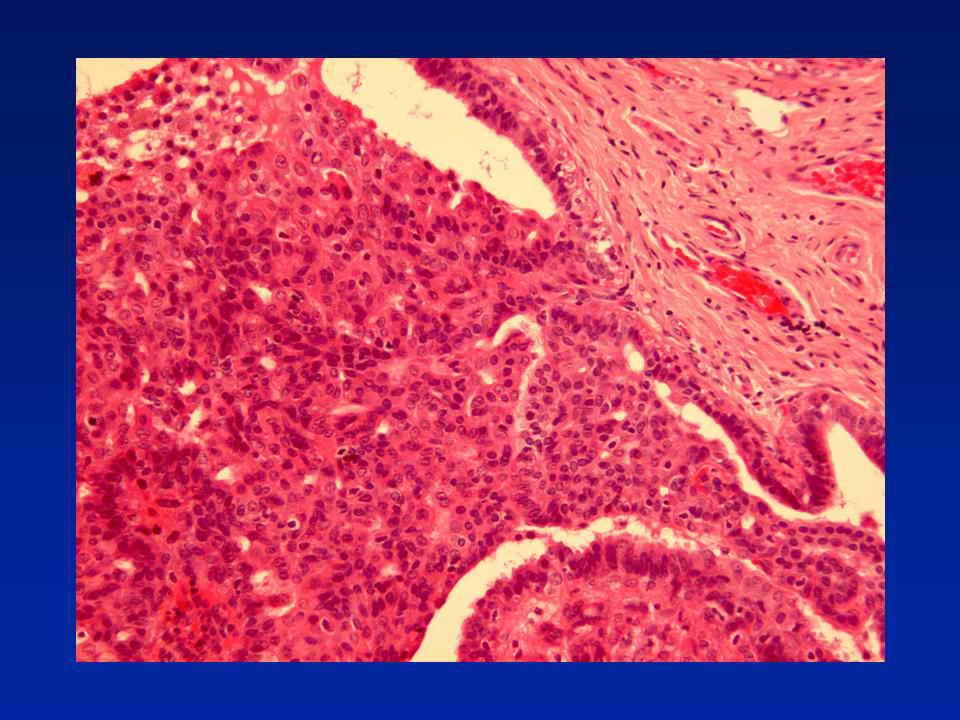
Diagnosis - Fibrocystic change with papillomas and florid usual epithelial hyperplasia

31
Case 32

46
Diagnosis - Fibrocystic change with atypical lobular hyperplasia and flat high grade DCIS

47
Case 54

54
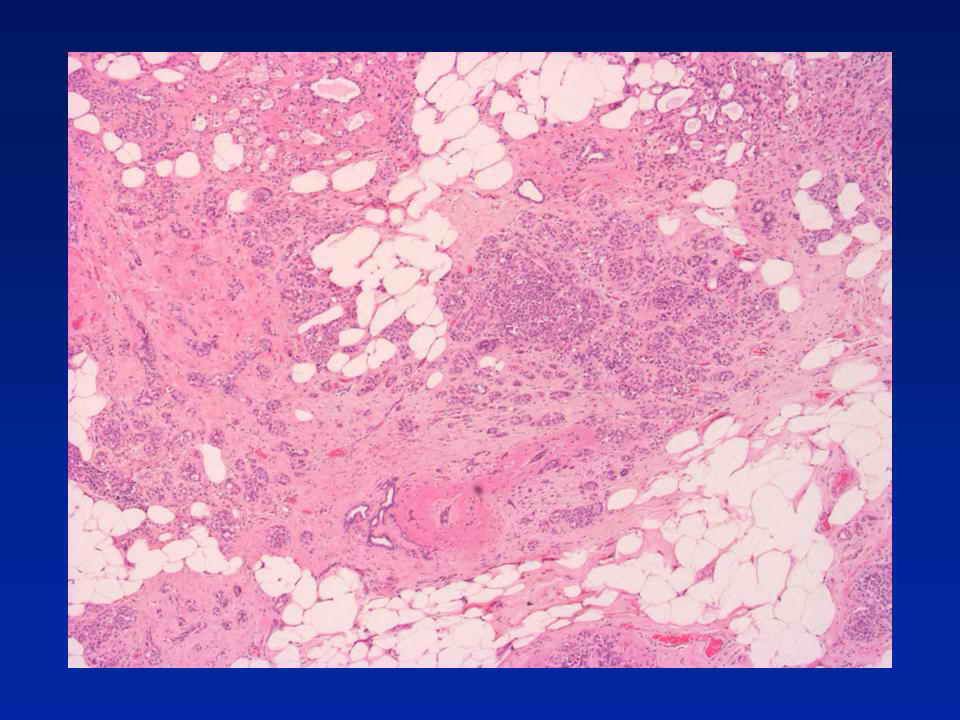
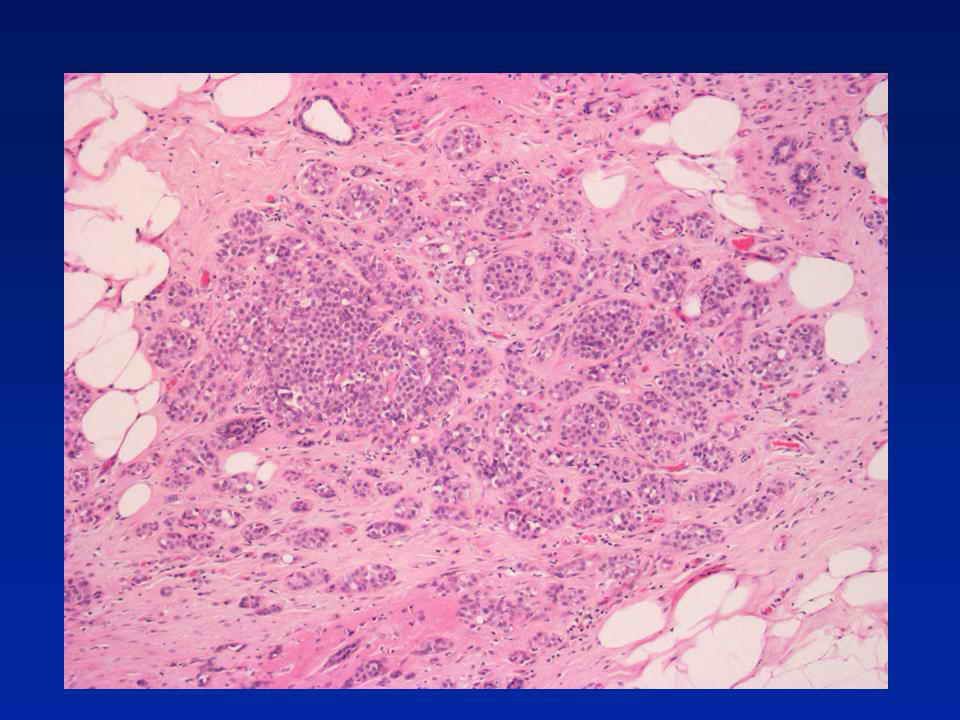
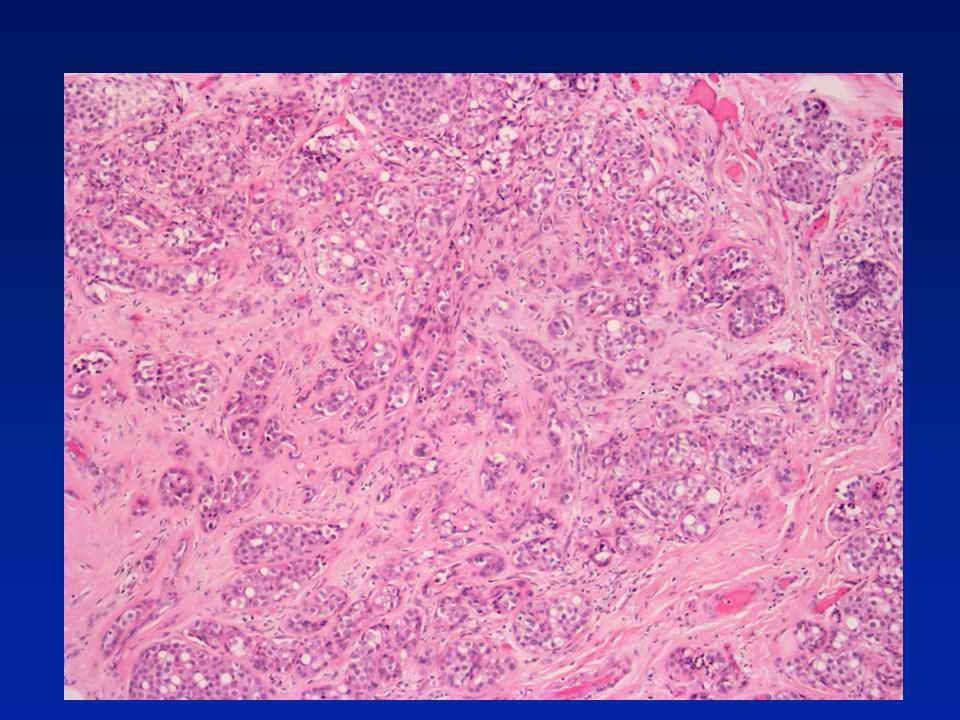
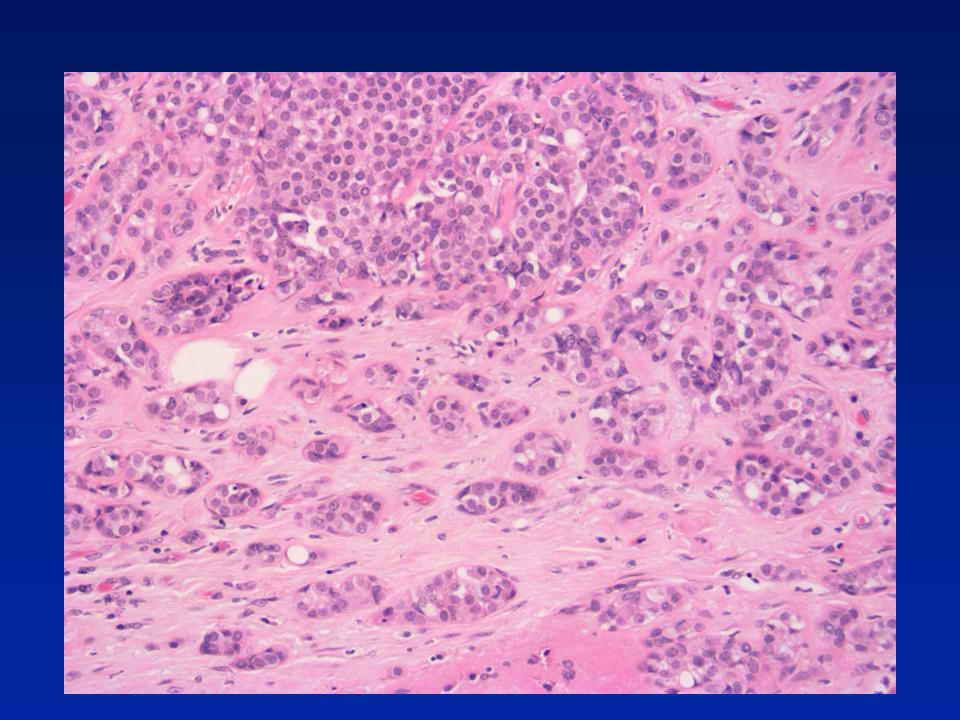
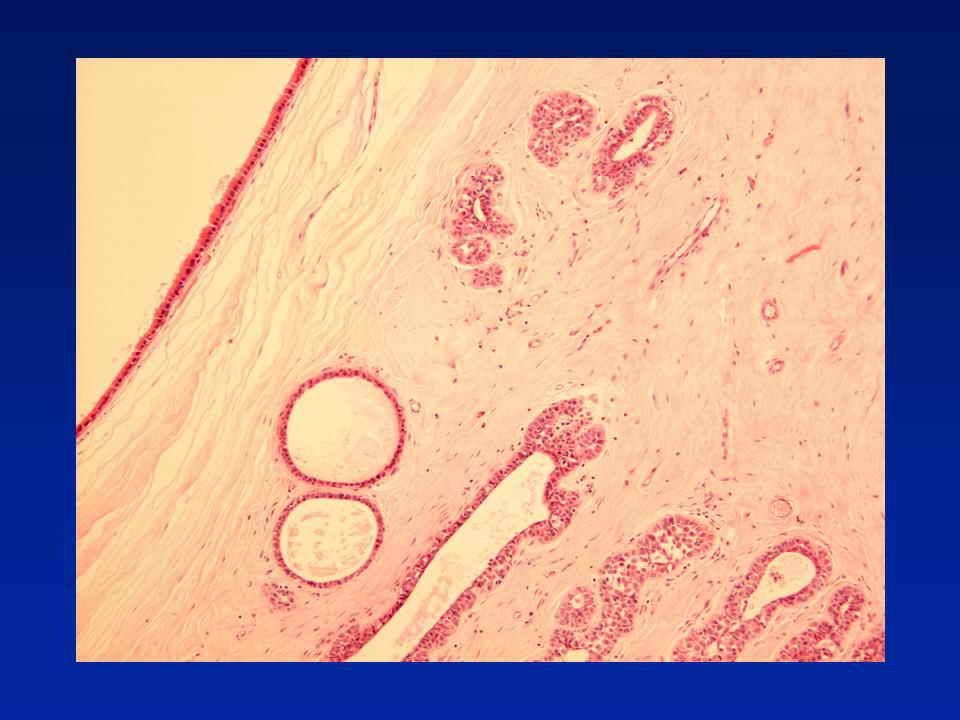
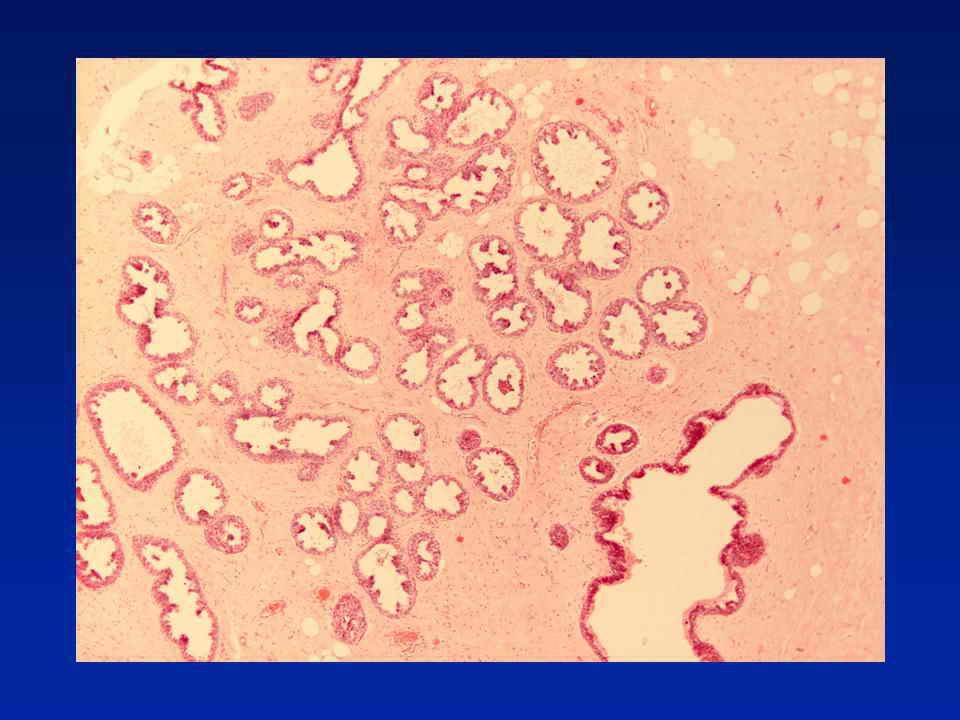
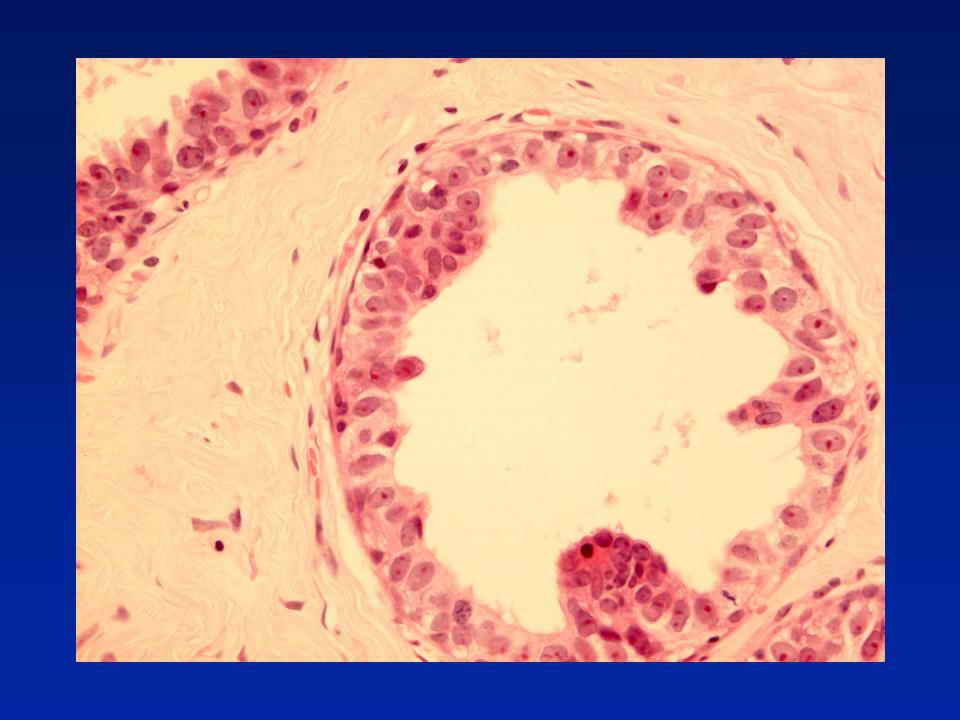
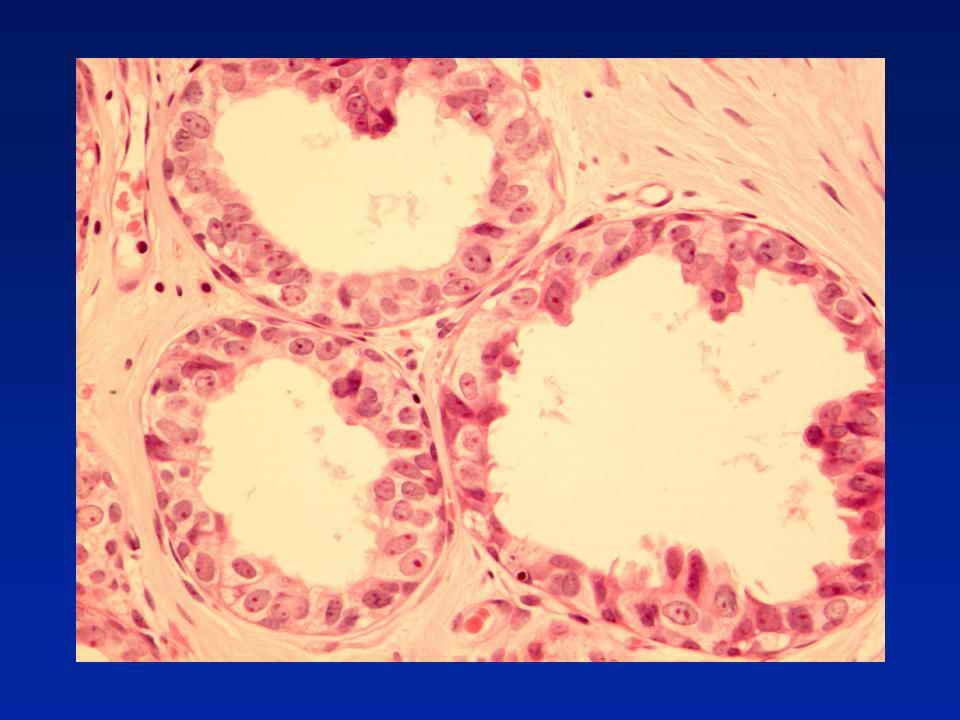
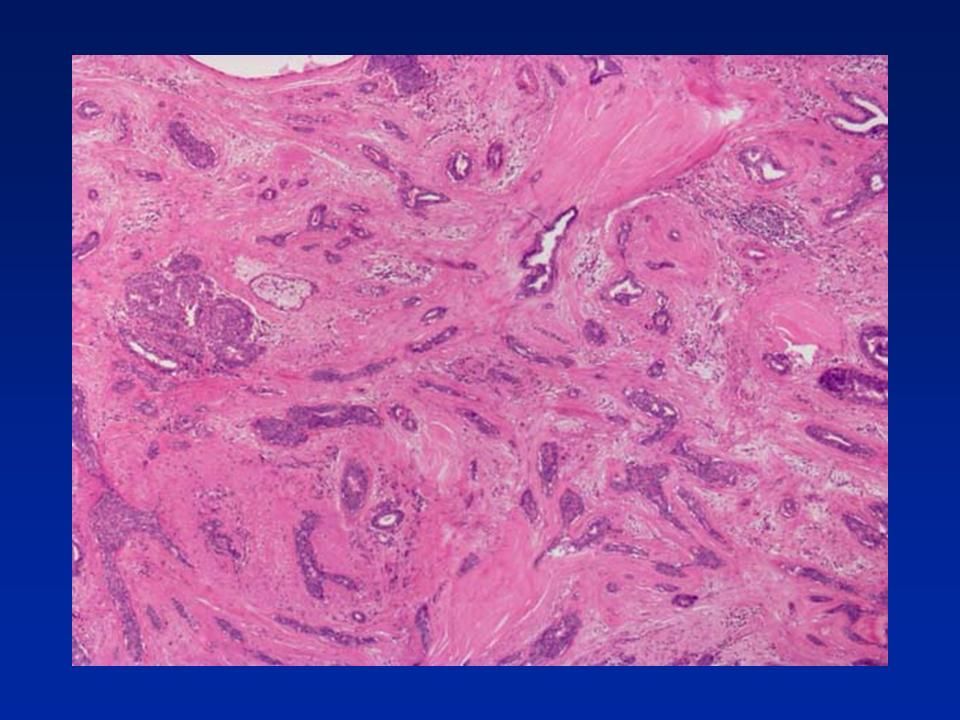
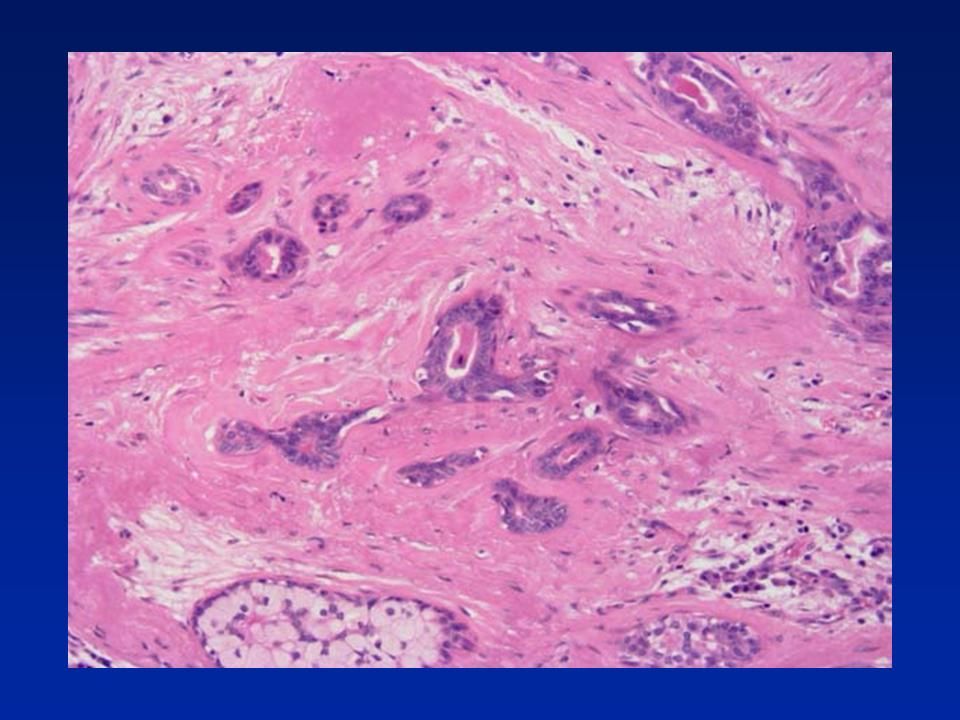
Diagnosis - Radial scar with florid usual epithelial hyperplasia

55
Central fibro-elastosis with entrapped tubular structures Usual epithelial hyperplasia Helpful features – retraction around tubular structures – often seen in radial scars Lack of fibroblastic stromal reaction (commonly, but not invariably seen (!) in tubular carcinoma) Confirm presence of myoepithelial cells and exclude diagnosis of tubular carcinoma (e.g. with smooth muscle myosin or smooth muscle actin or p63) In the epithelial proliferation look for (a) mixed population, (b) streaming and (c) slit-like peripheral spaces Radial Scar
 In the epithelial proliferation look for (a) mixed population, (b) streaming and (c) slit-like peripheral spaces Radial Scar.")
62
Case 44

69
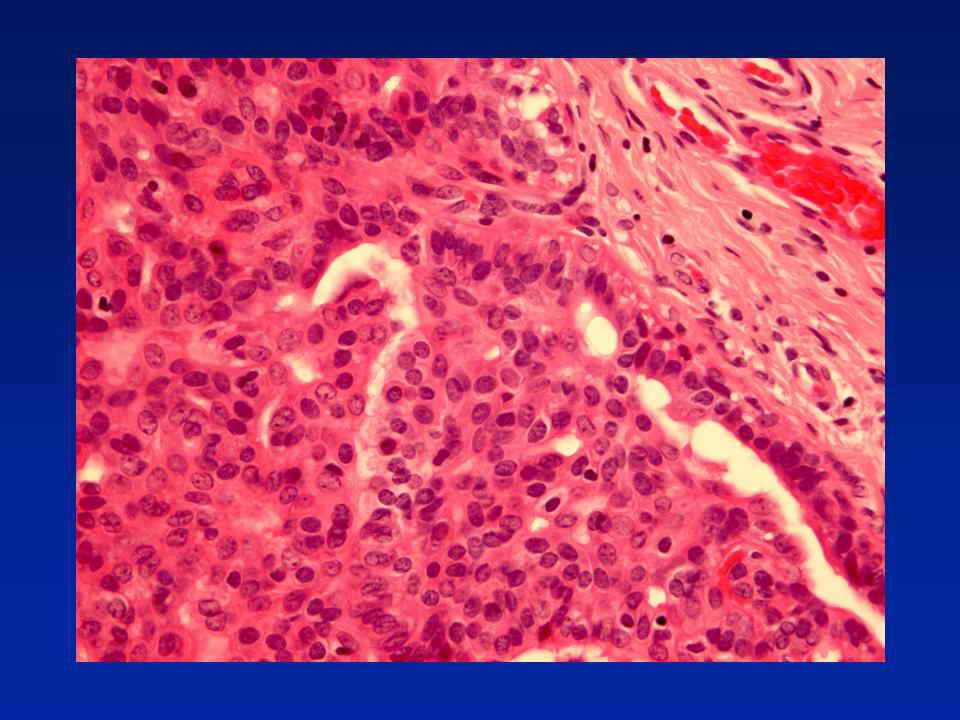
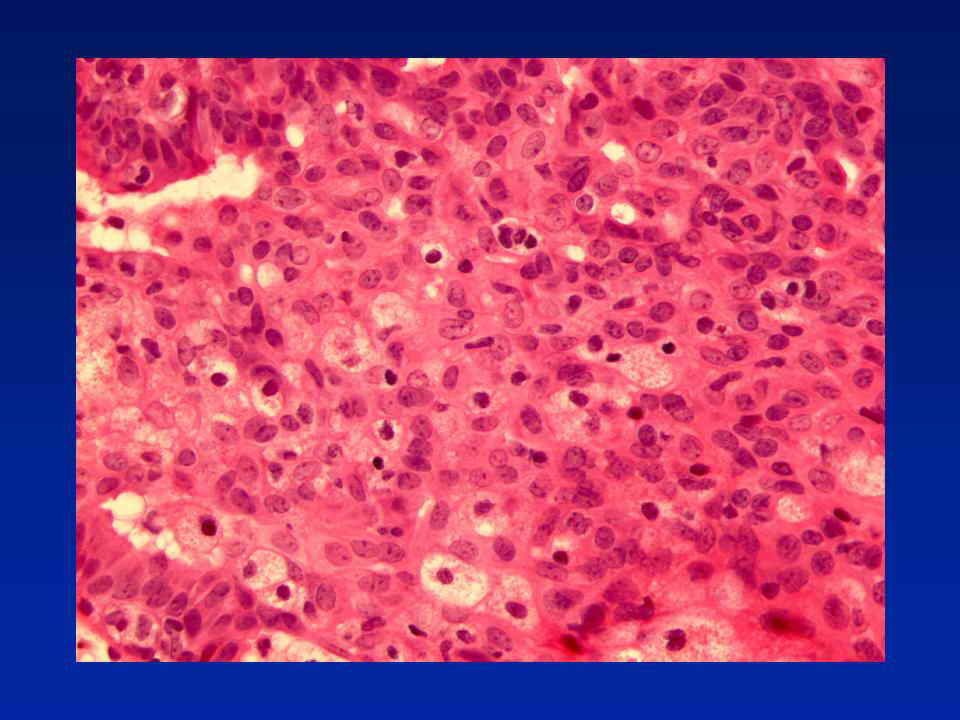
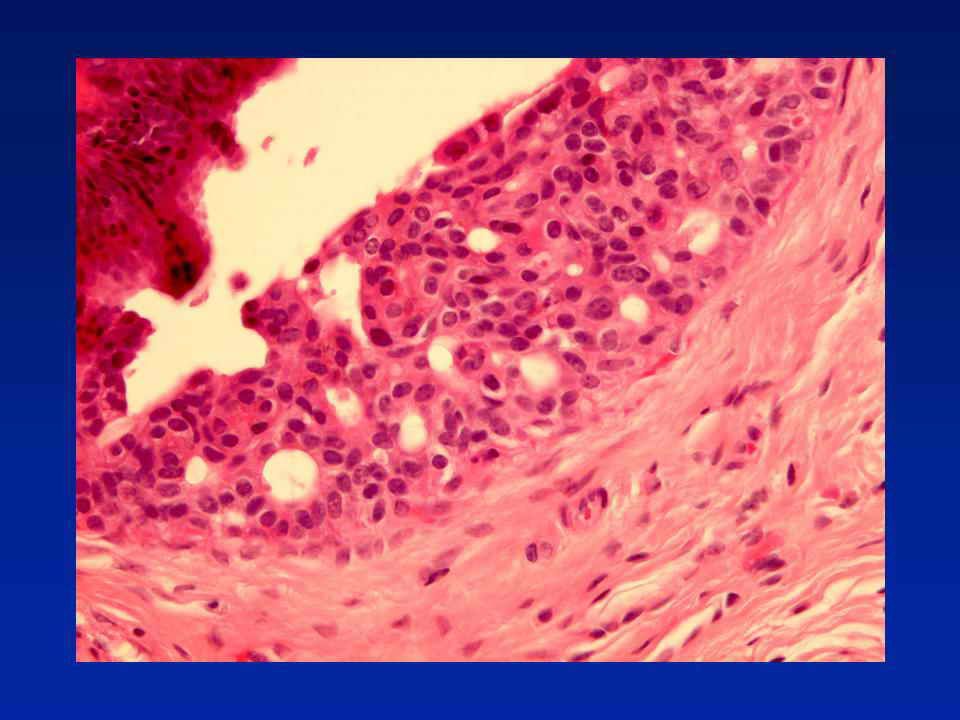
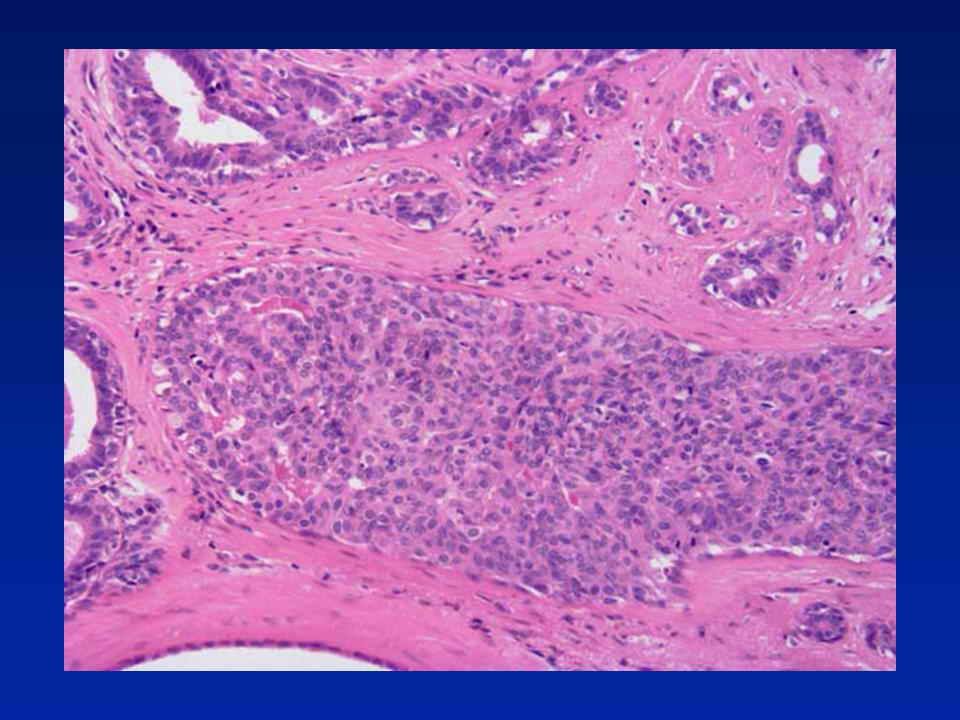
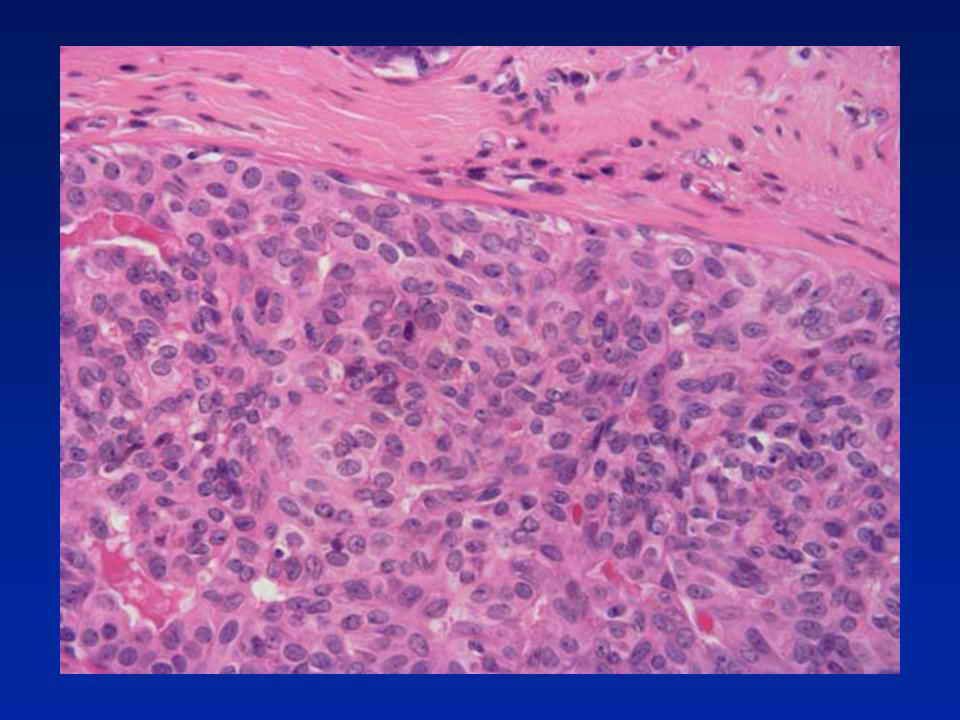
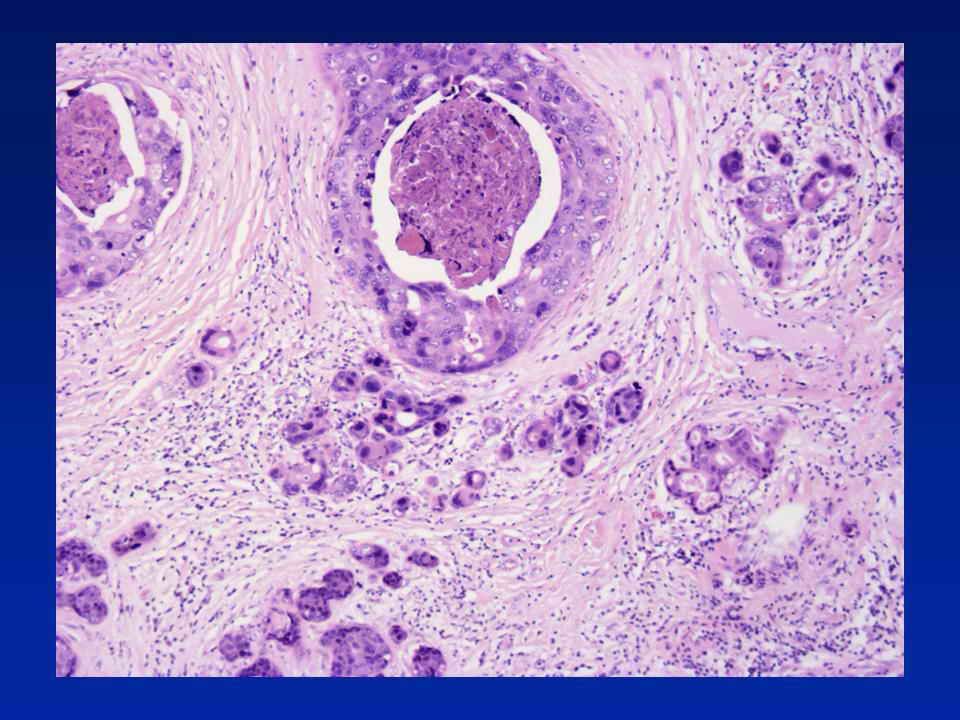
Diagnosis - High grade DCIS with comedo- type necrosis and cancerisation of lobules. No invasion or microinvasion.

70
Microinvasion DCIS with a focus of invasion less than 1mm in max. dimension More than one focus, if each less than 1mm Individual deposits may vary in size from a few islands to 1 mm diameter In the non-specialised, interlobular or inter-ductal connective tissue - neoplastic islands definitely within interlobular fibrous or adipose tissue Excludes: Ultrastructural or immunocytochemical evidence of breached or discontinuous basement membrane "Cancerisation of lobules"

71
Microinvasion Observations Associated with high-grade comedo DCIS more than other types Increasing risk of axillary node involvement with increasing duct space involvement (>50 ducts)
")
72
Microinvasion Problems of interpretation Duct boundary poorly defined Periductal fibrosis Indistinct basement membrane zone Tangential cutting of involved duct/lobule

73
Microinvasion Tips Outside organoid structures Involves non-specialised stroma Host lymphocytic response No myoepithelial component

74
Microinvasion Key points Restrictive definition Rare Axillary node involvement low Prognosis very good

79
Case 11a

89
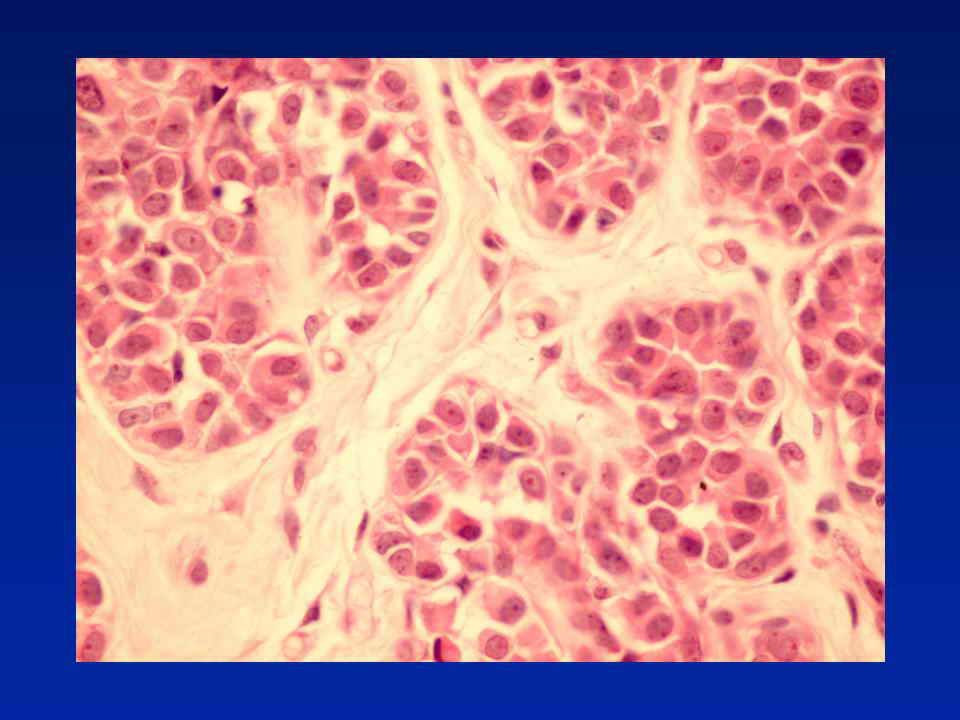
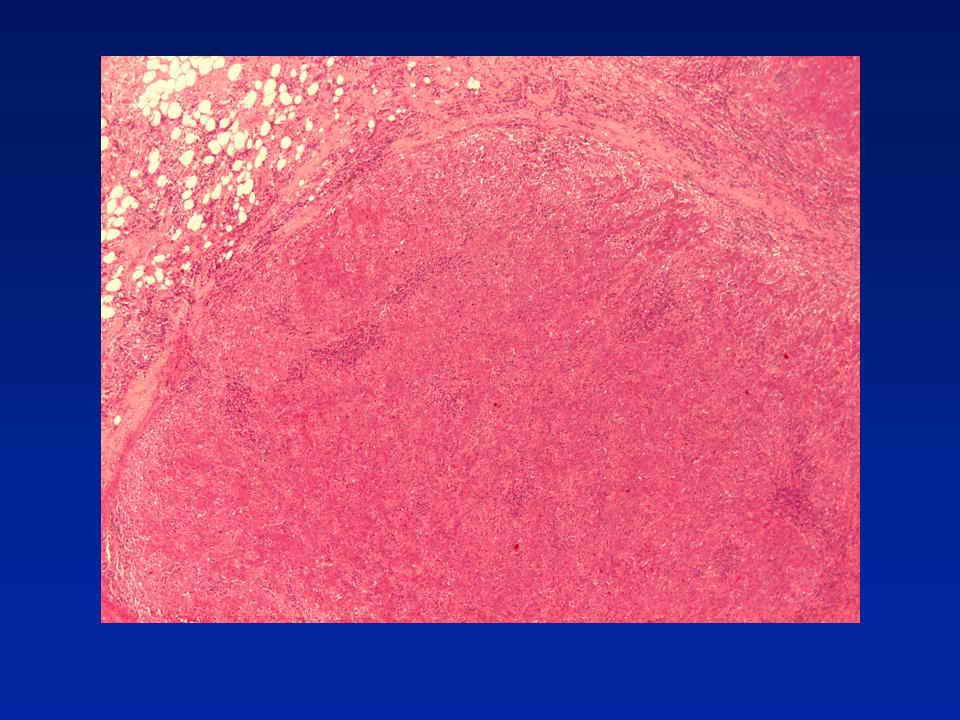
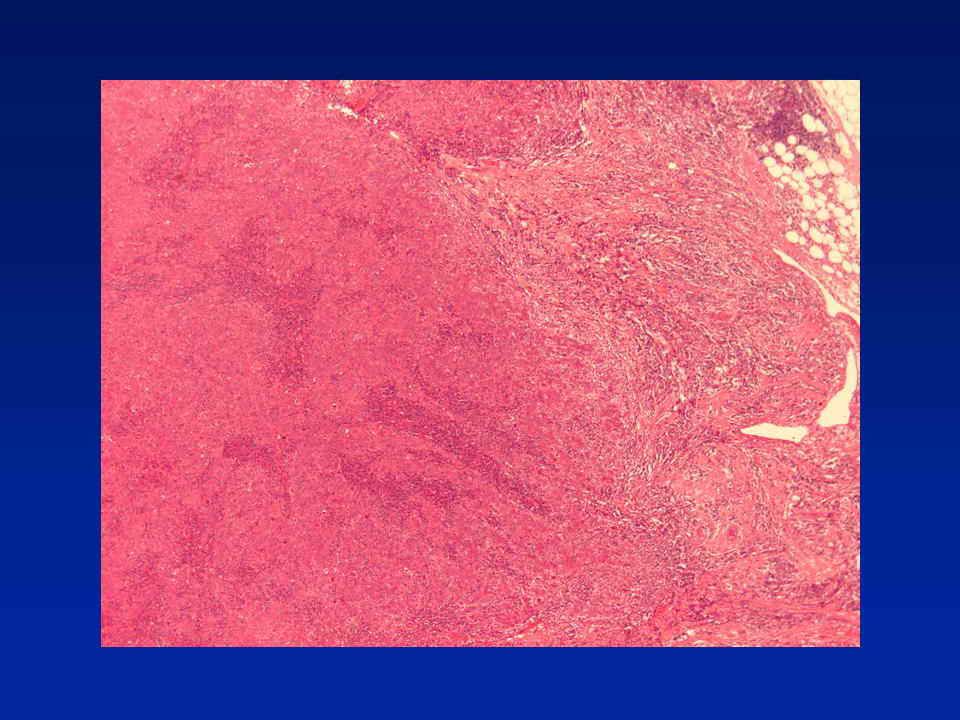
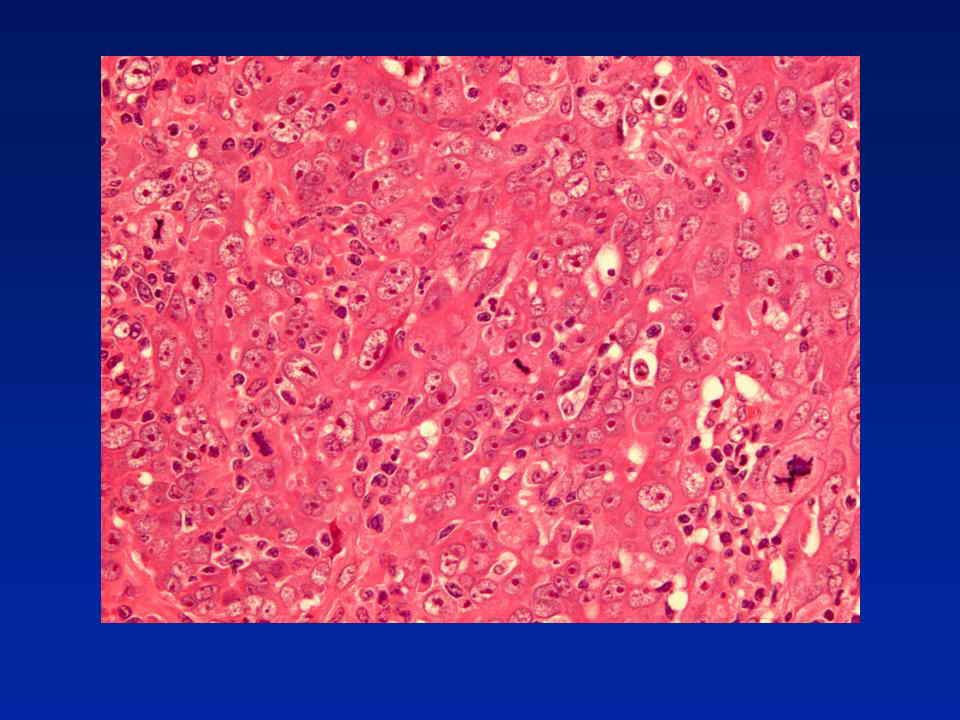
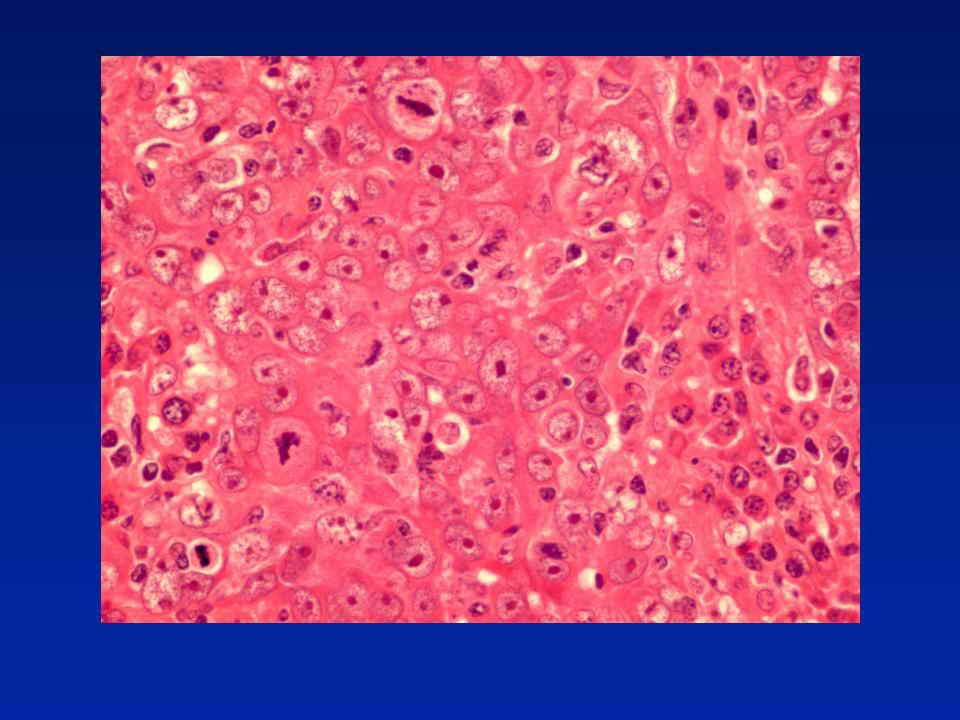
Diagnosis - Medullary-like carcinoma

90
CASE ? 36 year old patient Mastectomy and ALND post chemotherapy 5 months previously had core from 41mm mobile hypoechoic mobile mass in RUOQ

93
Core Biopsy B5, invasive carcinoma of provisional (core) grade 3 (333) and no special type ER = 6/8 PGR = 0/8 HER2 = negative (score 0)
 grade 3 (333) and no special type ER = 6/8 PGR = 0/8 HER2 = negative (score 0)")
105
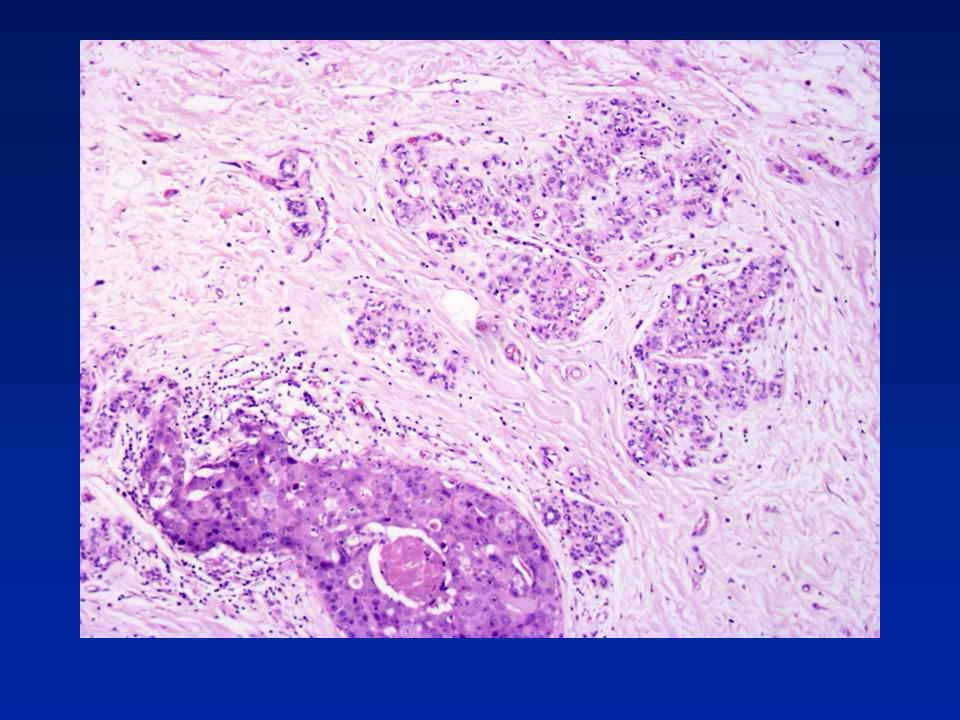
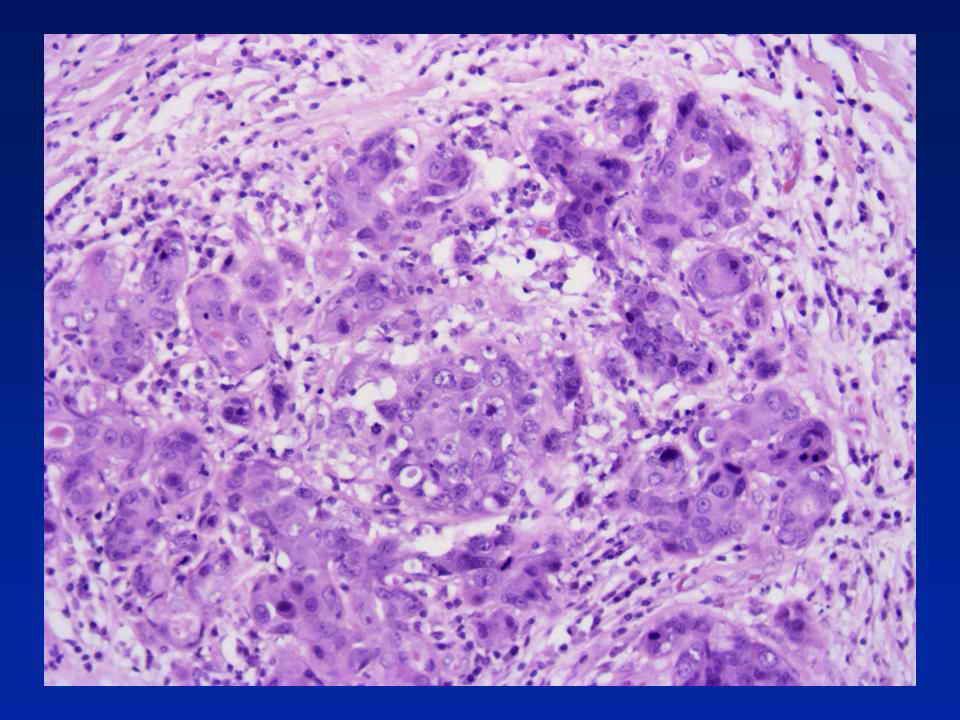
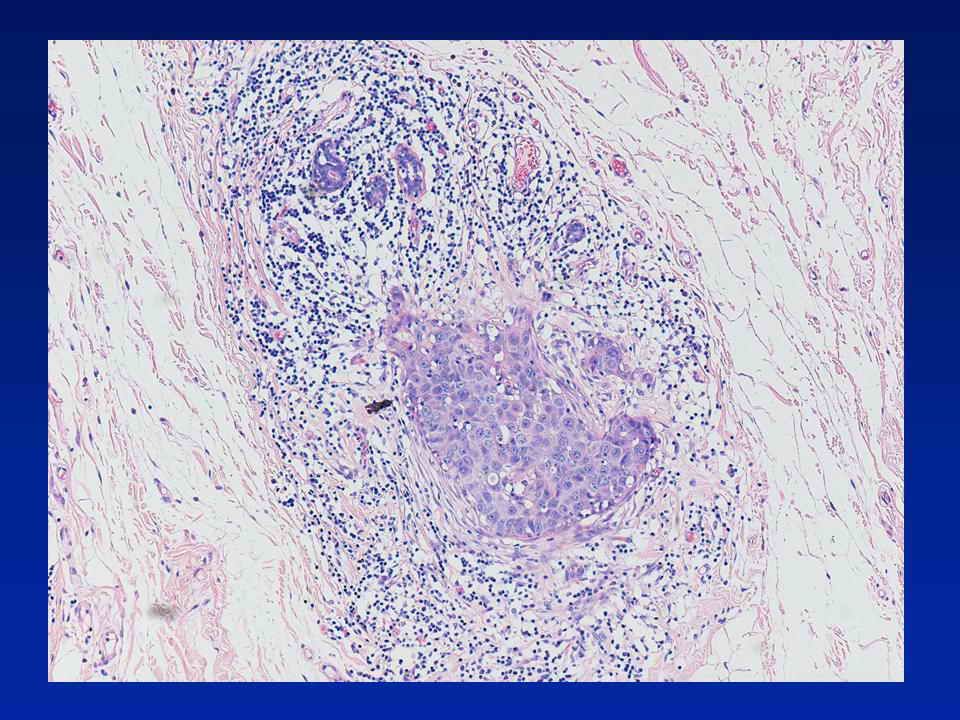
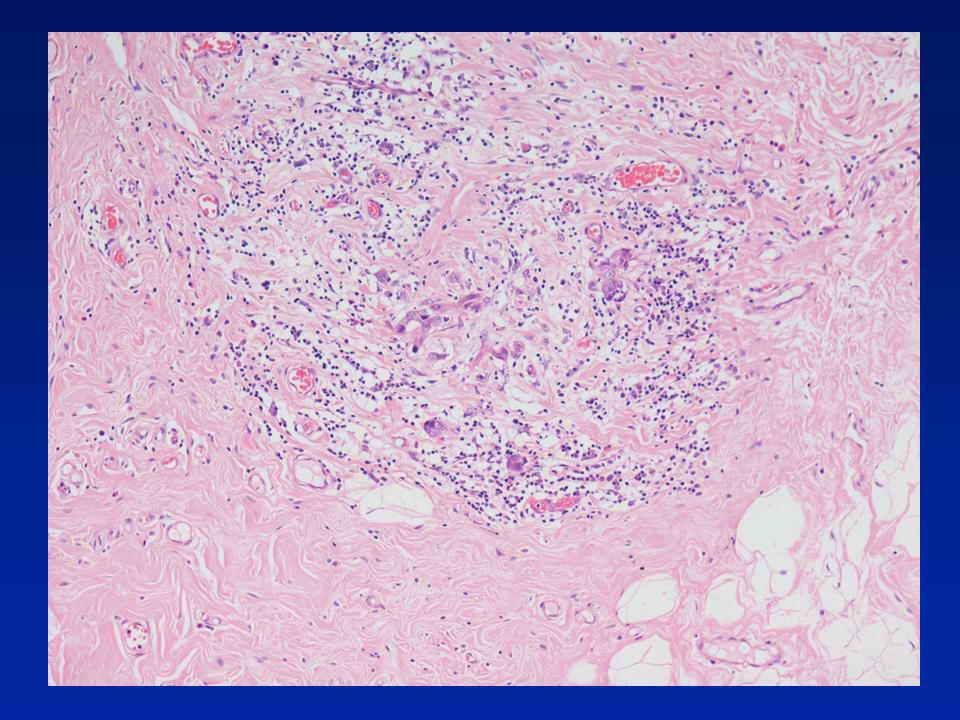
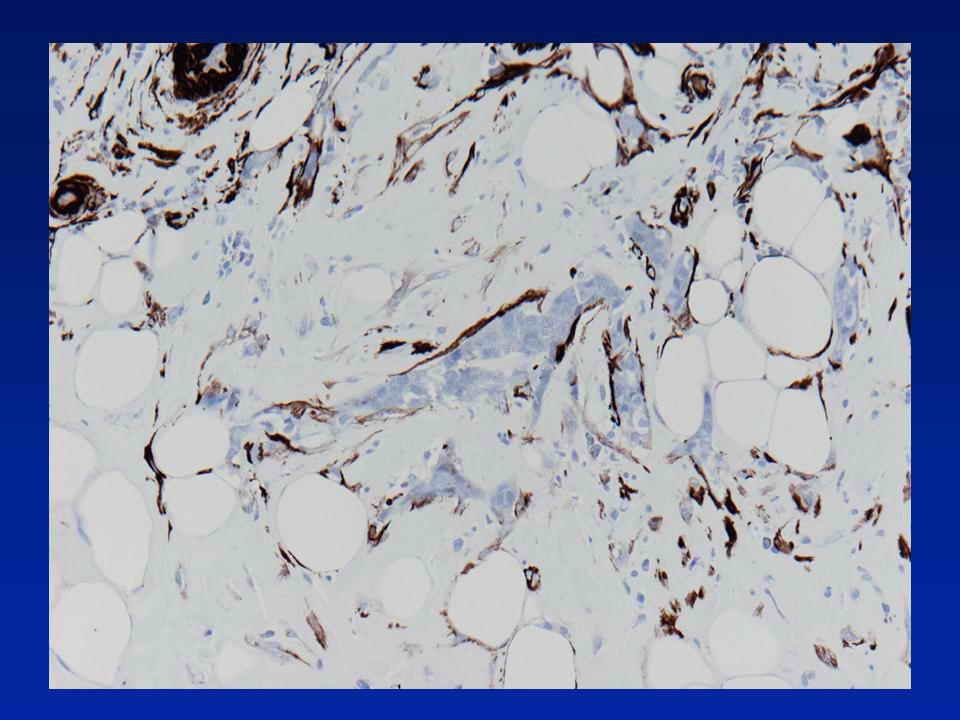
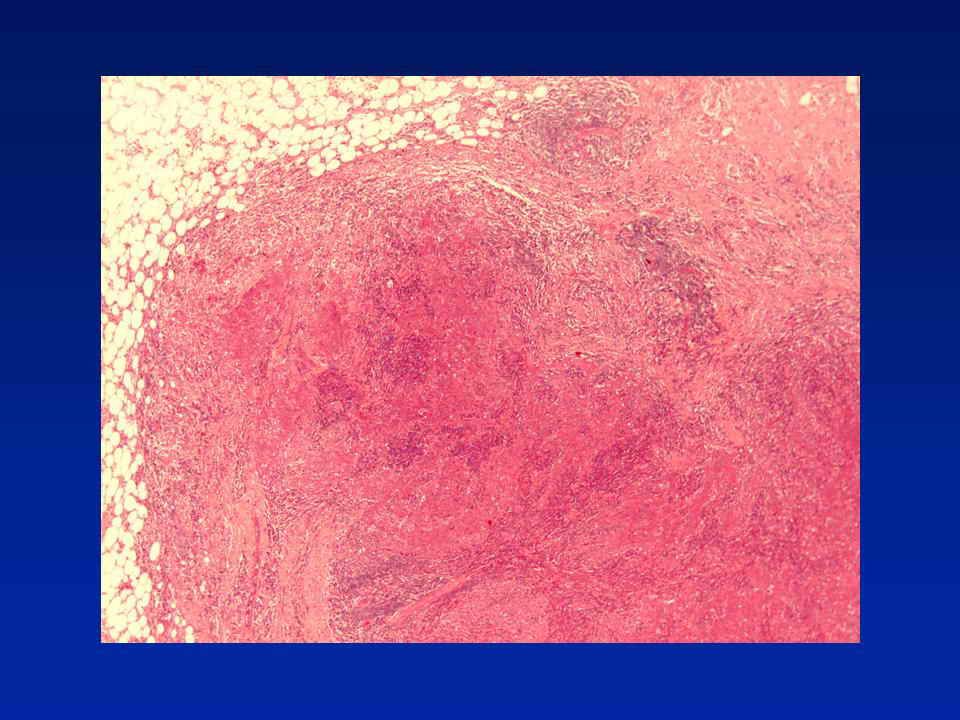
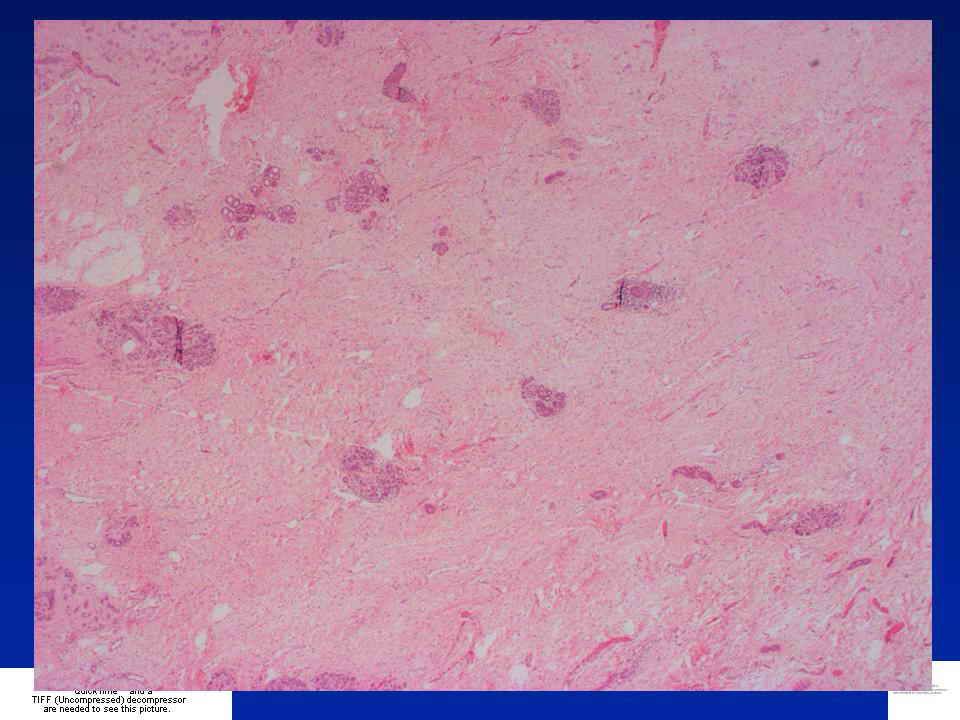
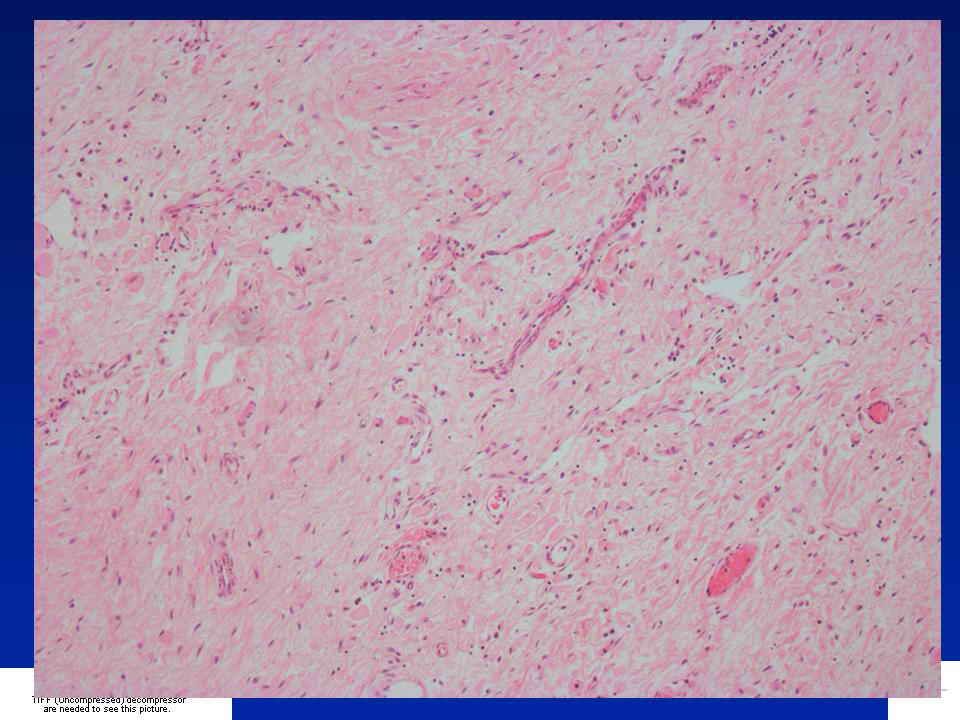
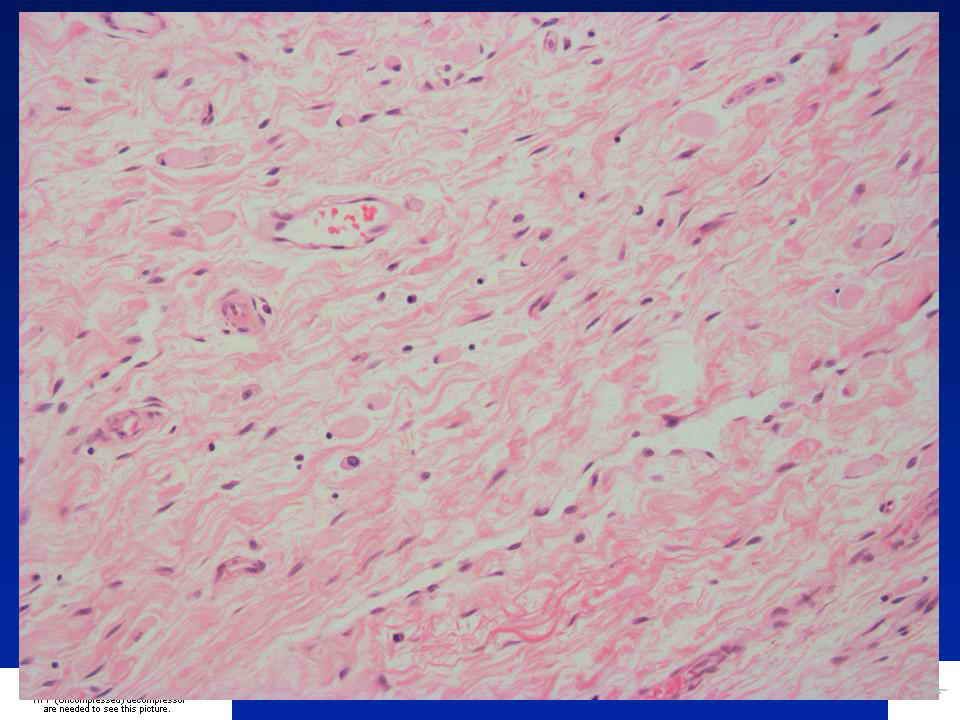
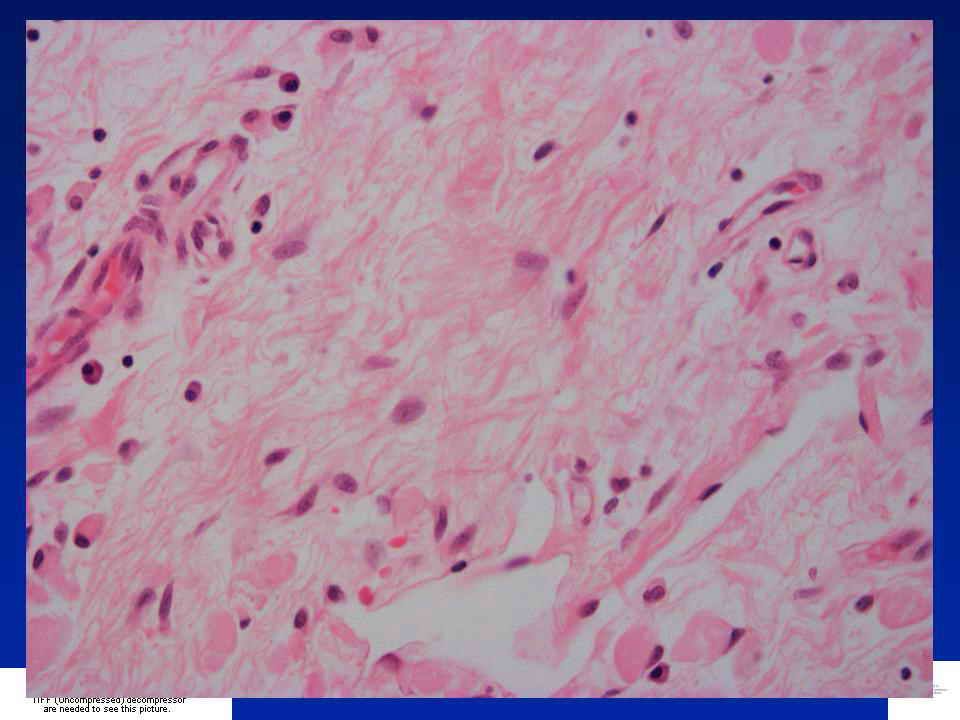
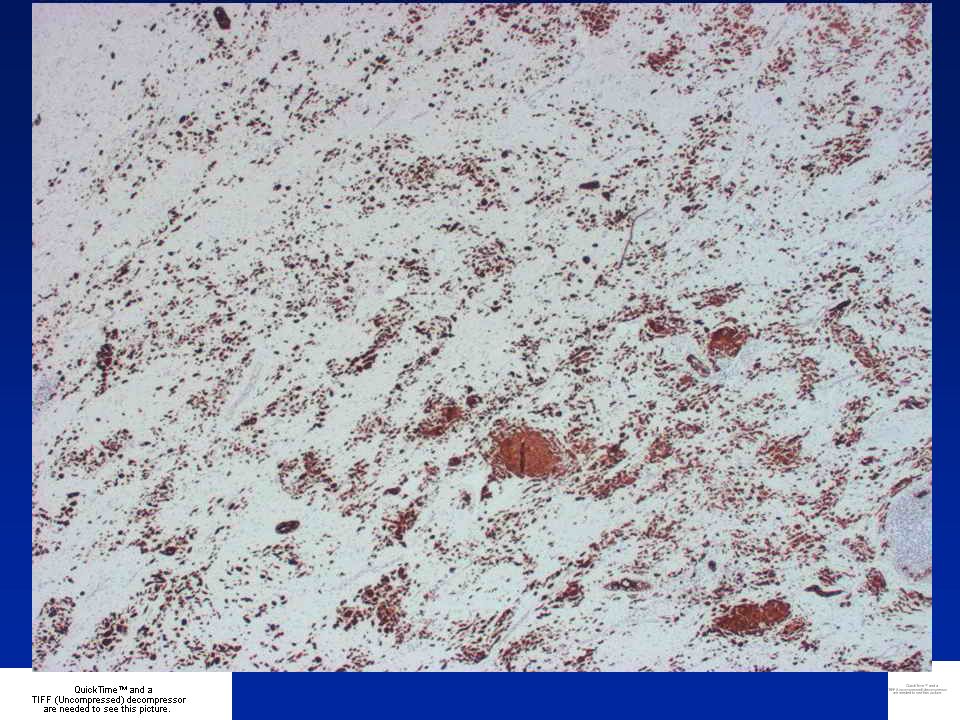
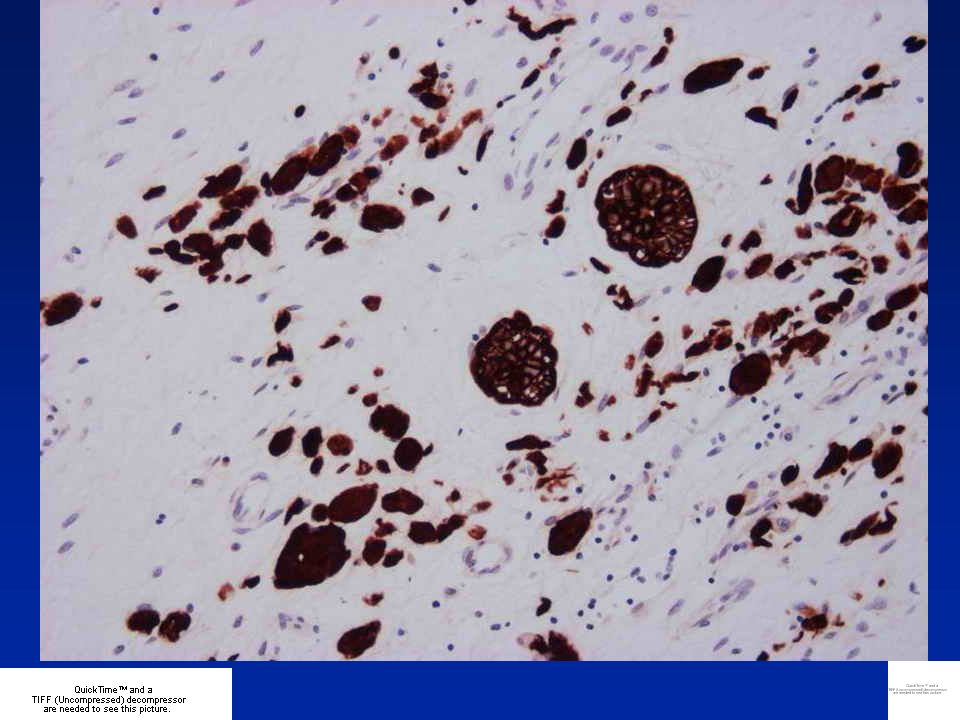
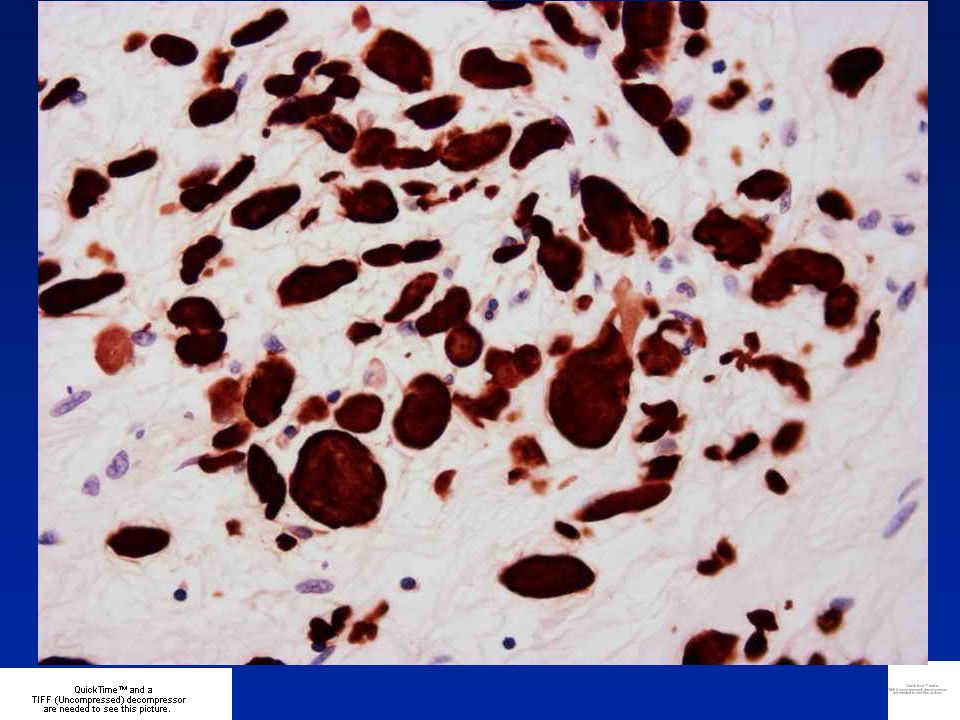
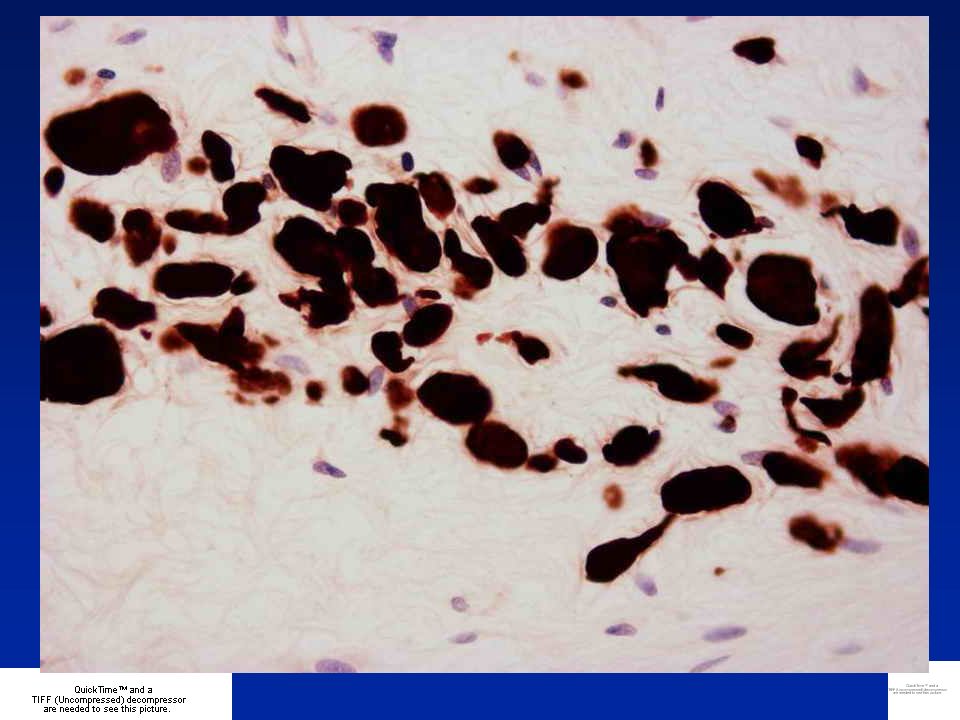
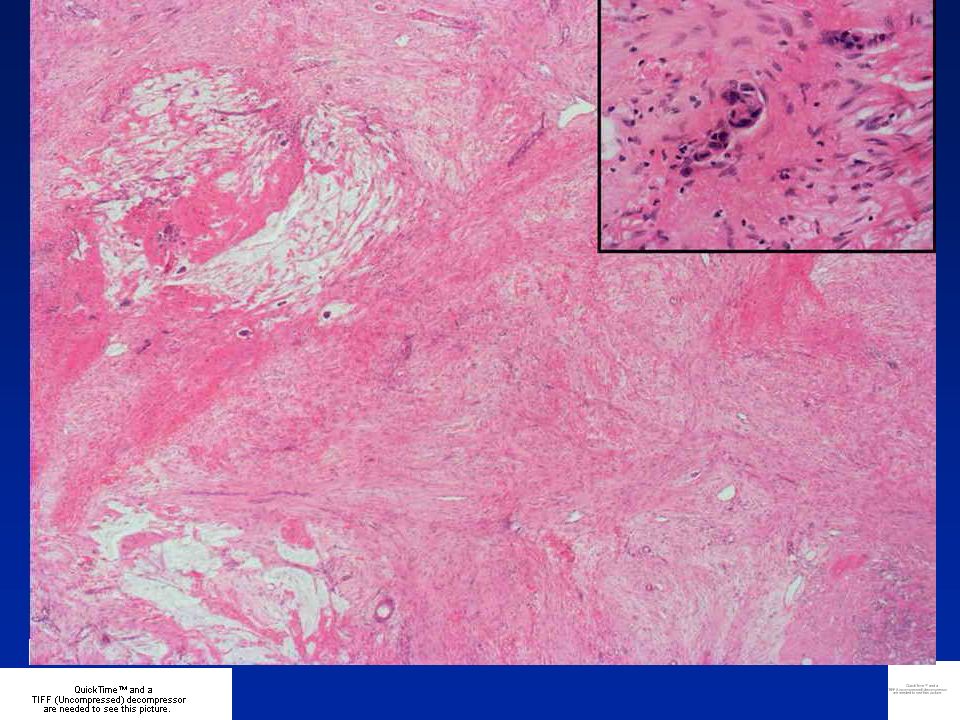
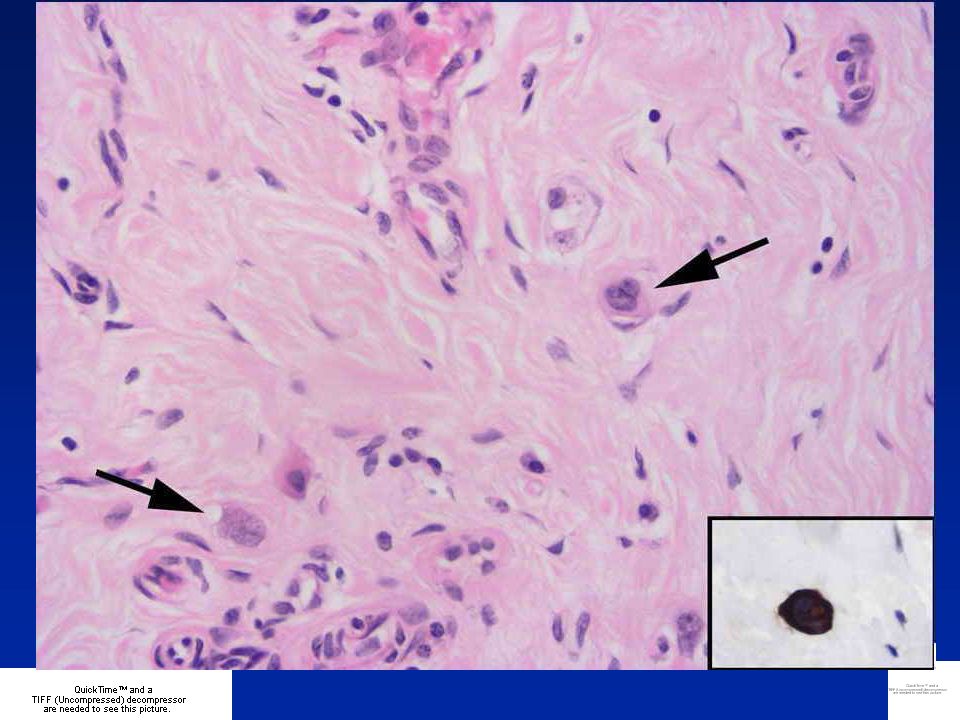
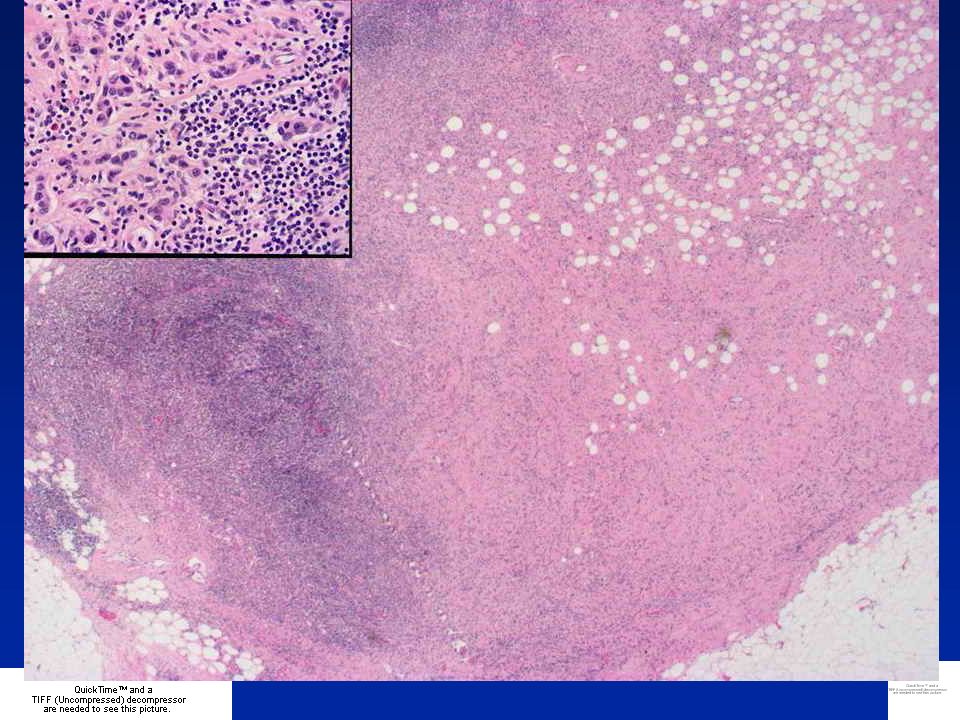
Diagnosis Residual carcinoma cells mimicking histiocytes

106
Central fibrotic scarring usually seen Patchy chronic inflammation within and around fibrosis Oedema or mucinous or myxoid changes to stroma or even areas of necrosis Cancer cells may mimic histiocytes, and vice versa, but collections of macrophages may also be present Cytokeratin IHC invaluable Post-Chemotherapy Changes

110
Grade 1 Some alteration to individual cells but no overall reduction in numbers compared to pre- treatment core Grade 2 Mild loss of invasive cells, still high cellularity Grade 3 Considerable reduction, up to 90% loss Grade 4 Marked reduction - only small clusters of widely dispersed cells detected Grade 5 No invasive carcinoma, in situ carcinoma or tumour stroma may still be noted Bonadonna G et al. J Natl Cancer Inst. 1990 3;82:1539-45 Smith IC et al. J Clin Oncol 2002;20:1456-66 Response to Chemotherapy

111
1.Disappearance of all tumour 2.Presence of in situ carcinoma but no residual invasive tumour & no metastatic carcinoma found in the lymph nodes 3.Invasive carcinoma present with stromal changes, such as sclerosis or fibrosis 4.Few modifications of appearance of tumour Chevallier B et al. Am J Clin Oncol 1993;16:223–228

Similar presentations