Download presentation
Presentation is loading. Please wait.

1
Which of the following statements are true regarding access preparation?
1. The objective of entry is to give direct access to the pulp chamber, not merely the canal orifices. 2. Access cavity preparations are similar to operative occlusal preparations 3. The likely interior anatomy of a tooth under treatment need not be determined before entry since unroofing will reveal canal orifice locations. 4. The rubber dam should always be placed before initial access preparation. All of the above None of the above 1 and 4 1 and 3

2
Answer: B None of the above
The objective of entry is to gain direct access to the apical foramina, not merely to the canal orifices. Remember straight-line access. Access cavity preparations are different from typical operative occlusal preparations since operative preparations are based on the topography of occlusal grooves, pits and fissures, and the avoidance of the underlying pulp. The likely interior anatomy of a tooth under treatment must be determined. Each tooth has a typical length, number, and configuration of canals. Radiographs taken from two different angles must be studied. The information gained before initiation of penetration will greatly facilitate the entry as well as subsequent treatment. When canals are difficult to find, the rubber dam should not be placed until correct location has been confirmed. Determination of the angle of malposed or extensively restored teeth can sometimes be easier with the dam off.

4
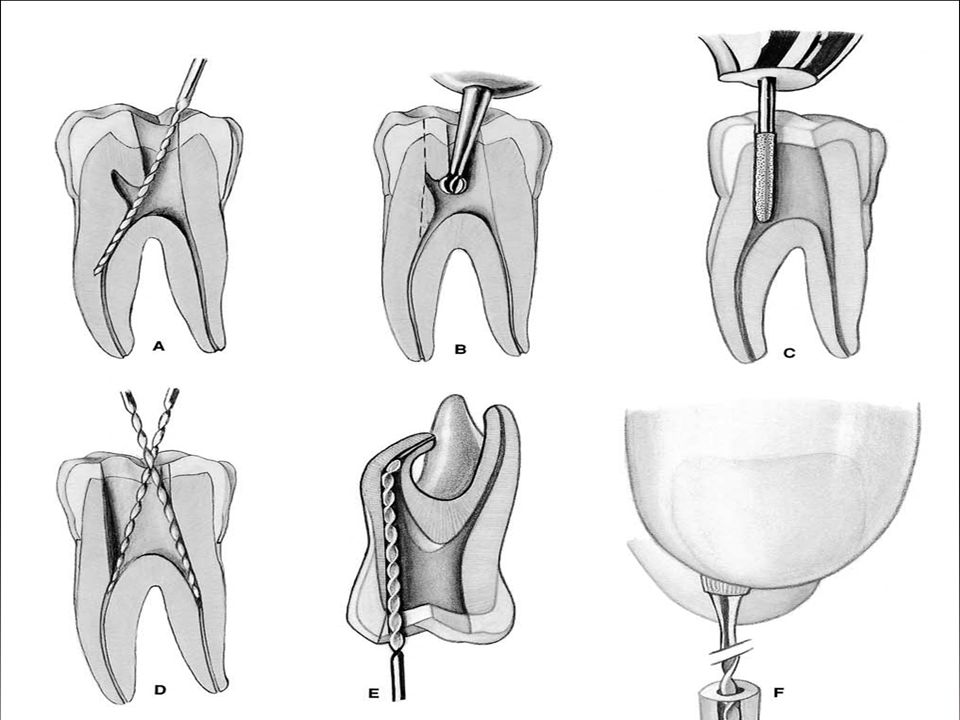
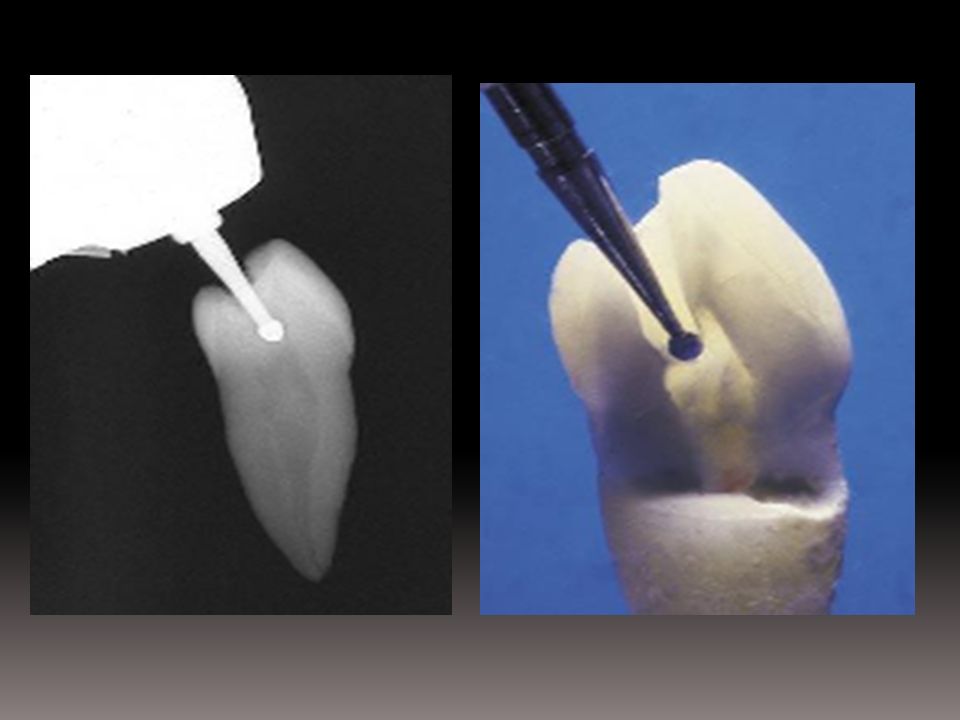
Basic steps in access preparation

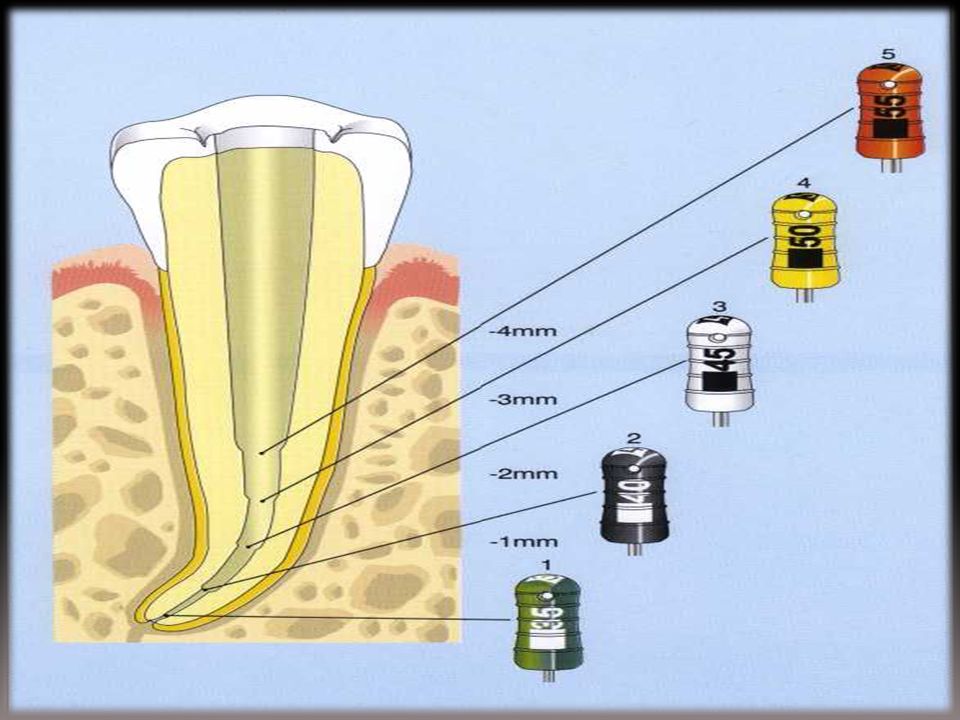
5
The D1/D16 distance is also constant (16 mm), so that the working portion of the instruments is always the same, despite the variability of the lengths of the available instruments: short (21 mm) for the molars of patients with small mouths, standard (25 mm), and long (31 mm) for the canines and any particularly long roots. D1 16 mm D16

6
Which are of the following are true of the balanced-force technique?
Balanced force uses three distinct phases that comprise the instrument cycle. Phase I involves the use of ultrasonic pre-debridement of the coronal 1/3. Phase III involves flute loading. The file is withdrawn after two to three dozen rapid rotations of the file. The balanced force involves file cutting at the apical extent of the file and not along its length 1 only 1, 2, 3 1, 3, 4, 5 2, 3, 4, 5 1, 3, 5

7
The correct answer is e. 1, 3, 5 as can be determined from reading of the below phases I-III of the balanced force technique.

8
In the balanced force technique the file is placed to working length and rotated clockwise 90 degrees with light pressure to engage dentin. The file is then rotated counterclockwise 120 degrees while apical pressure is maintained to cut and enlarge the canal. Debris is removed with a final clockwise rotation that loads the flutes with loosened debris.

9
The balanced force technique uses instruments in a step-back manner to initiate preenlargement of the canal and gain access to the apical third rapidly. This involves three distinct phases as follows: .

10
A prebent K file prior to apical instrumentation.
The instrument has become slightly straightened after being rotated apically.

11
80. Sterilization of Gutta percha points is done by:
A. Hot salt sterilizer B. Autoclaving C. Chemical solutions D. Dry heat. 80. Answer is: C- Chemical solutions.

12
5-minute treatment using sodium hypochlorite, Zephiran, and hydrogen peroxide.These agents were potent against gram-positive and gram-negative bacteria as well as endospore-forming microorganisms. Fungal spores were killed only by the first two. On the other hand, ethanol, chloroform, eugenol, betadine, and Gram's iodine solution were found not to be effective for surface sterilization.

13
Q- the accesses opening for amaxillary premolar is most frequently
a- oval b- square c- triangular d- non of the above a- oval

15
Q- the radiographic criteria used for evaluating the successes of endodontic therapy
a- reduction of the size of the periapical lesion b- no response to percussion and palpation test c- extension of the sealer cement through lateral canals d- non of the above a- reduction of the size of the periapical lesion

16
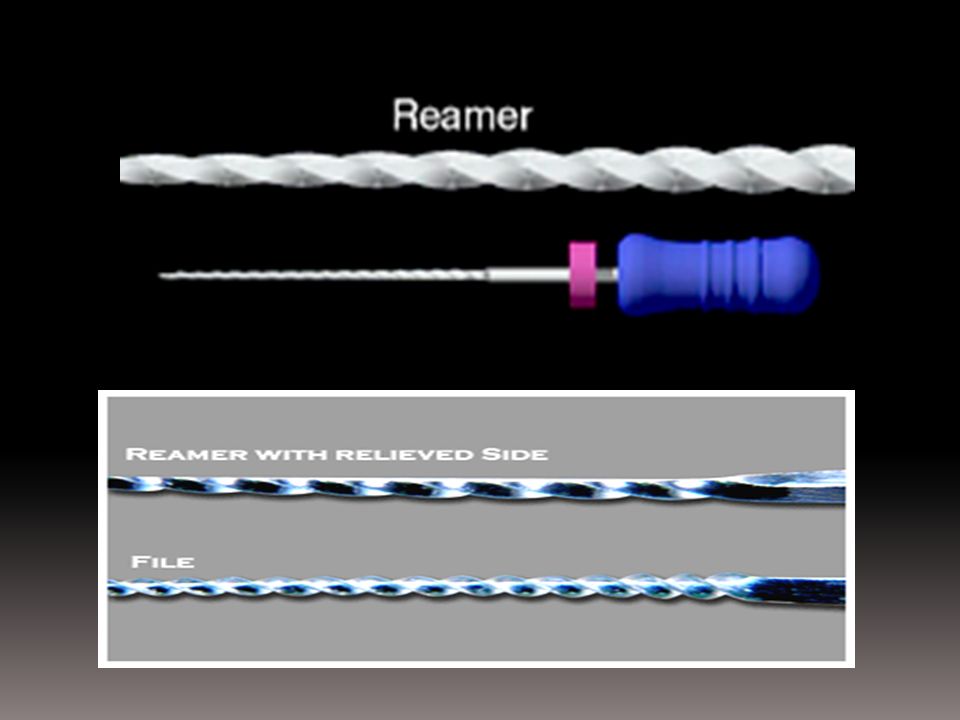
81. Difference between physical characteristics of a file & reamer is:
A. The cross-section of reamers is square and files are triangular in cross section. B. The numbers of flutes on the blade are more in files than in reamers. C. The reamers have more flutes in the blade. D. Files have two superficial grooves to produce flutes in a double helix design. 81. Answer is: B- The numbers of flutes on the blade are more in files than in reamers.

19
64.E.D.T.A. is chelating agent that:
1.lubricates 2.emulsifies 3.hold debris in suspension 4.remove smear layer 5.all of the above ANS. 5

20
66.Files are used in endodontic preperation to:
1.clean 2.shape 3.improve access 4.facilitate obturation a. all b. 1,2,3 c. 1,2,4 d. 2,3,4 ANS : c

21
1. For lower premolars, the purpose of inclining the handpiece lingually is to
A. Avoid buccal pulp horn B. Avoid lingual pulp horn C. Remove unsupported enamel D. Conserve lingual dentine Q1 = A

23
18. In which direction does the palatal root of the upper first molar usually curve towards
A. Facial / buccal/ B. Lingual C. Mesial D. Distal Q18= A

25
102. Tooth under occlusal trauma shows
A. Bone resorption B. Necrosis of the pulp C. Hypercementosis D. Triangulation E. All of the above Q102=E

26
119. The BEST treatment for alveolar abscess
A. Endontic treatment or extraction B. Incision and drainage alone C. Extraction D. Endodontic Q119=B

27
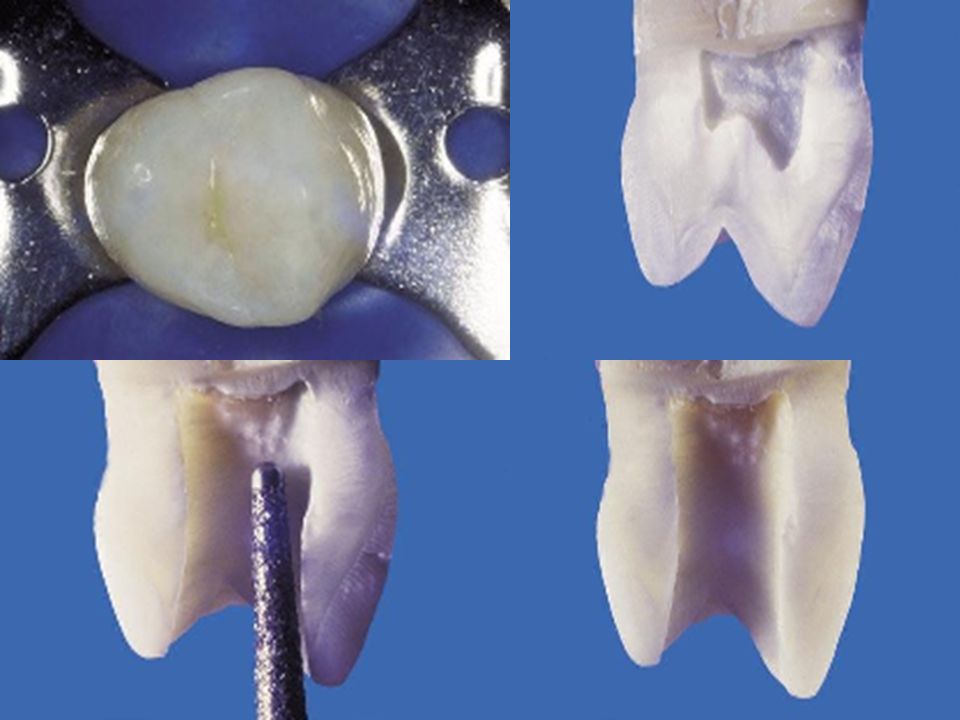
132. How do you prepare floor of pulp chamber in molars
A. Swab and dry with cotton wool and excavate B. Use round bur to flatten the floor C. Under cut walls D. Use flat end fissure bur to make it levelled Q132=A

28
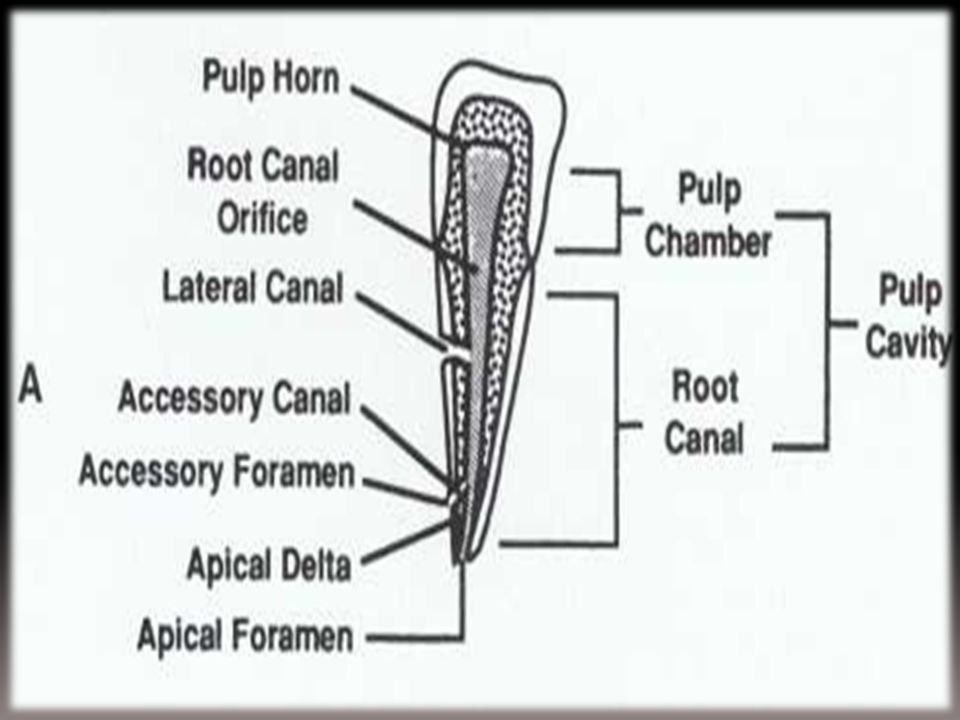
170. Lateral canals are usually found
A. The middle of the root B. Fist third of the root close to the crown C. The apical third Q170= A

30
176. Swelling after RCT is mainly caused by “Being asked as What is the most frequent cause of pain which occurs several days after obturation” too A. Entrapped Bacteria, or the presence of bacteria in the periapical region. B. Under filling the root canal system C. Over filled root canal Q176=A

31
183. To remove the pulp tissue from narrow canal, you can use
A. Barbed broach B. Small K-Type file C. Smooth broach D. Reamer Q183=B

32
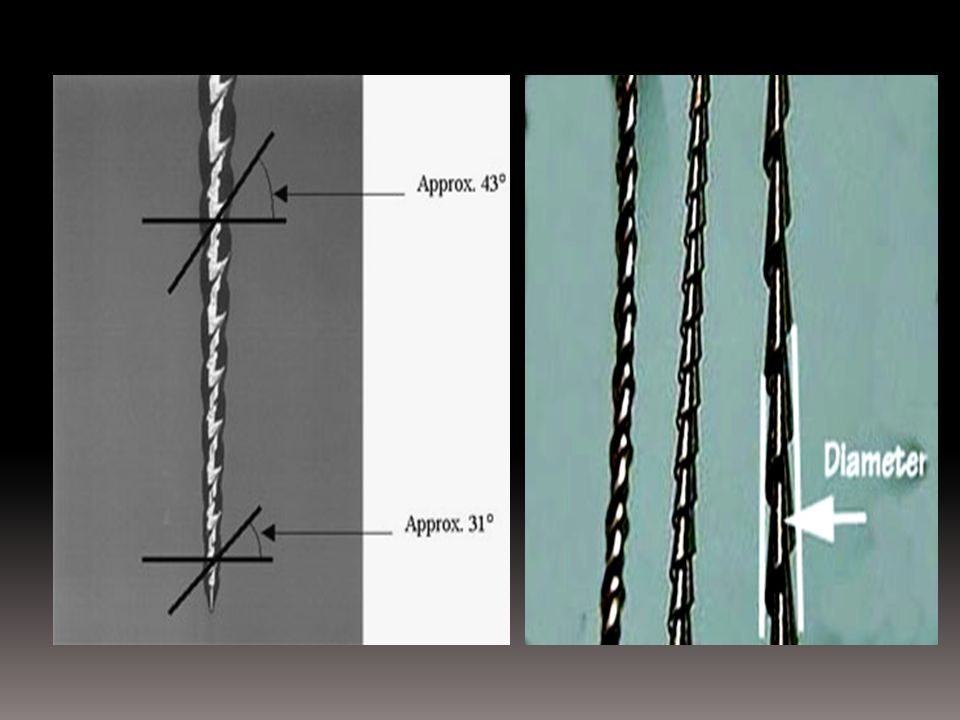
B. K-FILE K-file: Design & Structure
Manufactured from square or sometimes triangular steel wire that is twisted to give the typical shape of a K-file. The angle between the long-axis and the cutting blade is greater than in a reamer, and therefore preparation by a K-file is effective both in rotary and filing motion.

33
The tip of the instrument is cutting which makes the K-file best suited for the preparation of straight canals. Small K-files (ISO ) can be also used in curved canals without the risk of ledging. Small K-files are particularly good for the initial preparation of very narrow canals.
 can be also used in curved canals without the risk of ledging. Small K-files are particularly good for the initial preparation of very narrow canals.")
34
A. Lateral Condensation B. One major Gutta Percha point
199. The technique of placing Gutta-Percha cones against the root canal walls providing space for additional Gutta Percha is termed A. Lateral Condensation B. One major Gutta Percha point C. Laterally above condensed Q199=A

35
215. In young children what is the commonest finding after dental complaint
A. Acute periodontal abscess B. Chronic periodontal abscess C. Apical abscess D. Chronic alveolar abscess Q215=C

36
226. Electrical pulp testing is least useful in /or does not detect in some papers
A. Traumatised teeth B. Just erupted teeth C. Multi-rooted teeth D. Capped teeth E. Necrotic pulp Q226=D

37
227. The palatal pulp horn of maxillary molars is located
A. In the pulpchamber under mesiolingual cusp B. In the pulpchamber opposite the mesio distal fissure of the buccal cusp C. Under the disto lingual cusp Q227=A

38
251. How would you diagnose a periapical abscess
A. Pain on percussion B. Pain when eating hot food C. Pain when eating cold food D. The thickness of periodontal ligament on X-Ray Q251=A

39
270. The term TUGBEN?? is related to : “When used in connection with a master Gutta Percha cone in endodontics” A. Tensile strength of the gutta percha B. Consistency of gutta percha C. Size of the cone D. Fit of the cone in the apical 1 or 2 mm E. Length of the cone Q270=D

40
271. In root canal therapy it is generally accepted that the ideal root filling
A. Should extend to the level of the apex to minimize irritation B. Should extend slightly through the apex to ensure a complete seal C. Should extend to the dento cemental junction for healing D. The extension of the filling is not critical Q271=C

42
Chronological cementum deposition with subsequent deviation of the apical foramen.

43
272. Mesiobuccal root of maxillary first molars MOST COMMONLY have
A. One canal with one foreman B. One or two canals with one foreman C. Two canals with one foreman D. Two canals with two foremen Q272=C

44
314. The method you will use to fill root canal of maxillary lateral incisor is
A. One major Gutta Percha cone B. Laterally condensed C. Laterally above condensed Q314=B

45
338. Which is NOT characteristics of canal filing materials “obturation material”
A. Tacky adhesive to walls B. Radio opaque C. Not irritating D. Quick in setting Q338=D

46
367. The most prominent feature of acute apical periodontitis is
A. Tenderness of tooth to pressure B. Extra oral swelling C. Intermittent pain Q367=A

47
431. Which of the following factors can affect the shape and size of the pulp canal
A. Chemical irritation and caries B. Trauma and function C. Attrition, wear and aging of the patient D. All of the above Q431=D

48
459. Where does the bone resorption show in a necrosis pulp of deciduous molar
A. At the root apex B. At the bifurcation C. On the buccal side of the tooth D. On the lingual side of the tooth Q459=B

49
Soft tissue exam swelling = nonvital tooth
exudate usually tracks buccally, resulting in either intra or extra oral swelling intraoral swelling more common in primary teeth because furcations are usually occlusal to the muscle attachments

50
A. Replace with similar dressing and prescribe antibiotic
495. While doing RCT you gave dressing with a paper point wetted with..??...solution. The patient arrives the next day with severe pain. There is no swelling but the tooth is tender to percussion. You will** A. Replace with similar dressing and prescribe antibiotic B. Replace with corticosteroid past C. Retrieve paper point surgically D. Remove the dressing and leave for several days before replacing it. E. Provide incision and drainage Q495=B. Ledermix is the best option

51
518. A 10 year old boy presents with non-vital, non-mobile tooth
518. A 10 year old boy presents with non-vital, non-mobile tooth. Treatment is A. Pulpectomy with calcium hydroxide B. Pulpectomy with Zinc oxide eugenol C. Pulpotomy with formocresol D. No treatment is required if tooth is asymptomatic Q518=D

52
519.A patient suffers a blow to his maxillary central incisor without resulting in fracture. The pulp A. Immediate necrosis B. Becomes non-vital but only if treatment is delayed too long C. Becomes non vital irrespective of treatment D. No changes is seen later if fracture does not occur Q519=C

53
546. Size of pulp chamber within the tooth is influenced by
A. Age B. Parafunctional C. History of the tooth /abrasion, erosion, caries/ D. All of the above Q546=D

54
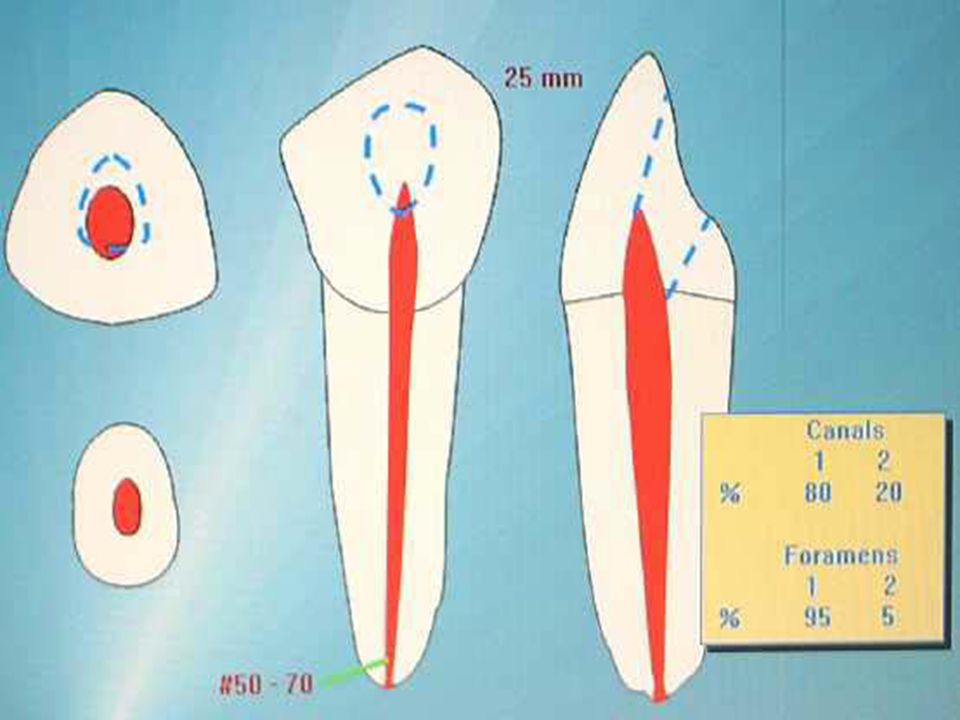
553. What is true in regards to lateral mandibular incisor
A. 20% have 2 canals with one foramen B. 20% have 2 canals with two foramina C. 40% have two canals with 10% ending in two foramina D. 40% have two canals with only one ending in two foramina Q553=D

56
A. Over instrumentation extending into area
567. After completing pulp extirpation, debridement and placing adressing; apical periodontitis is because A. Over instrumentation extending into area B. Irritation from chemicals used C. Entrapped bacteria D. One or any combination of the above Q567=D

57
771. At the end of four years, the x rays reveal calcification of
A. All deciduous and first permanent molars B. All permanent except of 3rd molars C. All deciduous D. All permanent Q771=B, 3rd molars calcify about the age of 7 to 8

58
789. Irrigation in root canal treatment, should be undertaken at frequent intervals during instrumentation to** A. Removes cementum falling from the canal B. Remove noxious material since it may be forced to the apical foramen resulting in periapical infection C. Destroy all micro organism in the canal D. Stop instruments from going beyond the apical foramen E. None of the above

59
Q789=B, Abbot Page 42: It is necessary to use irrigating solutions to,
1.Lubricate the canals walls. 2. Remove debris. 3. Act as solvent (organic and morganic matter) 4.Act as anti-microbial agent. 5. Aid cleansing in areas that are inaccessible to mechanical cleansing methods.
 4.Act as anti-microbial agent. 5. Aid cleansing in areas that are inaccessible to mechanical cleansing methods.")
60
4) The earliest and most common of an acute pulpitis :
a) a dull throbbing pain. b) pain upon chewing. c) thermal sensitivity. d) discomfort, particularly on palpation Question 4=c
 a dull throbbing pain. b) pain upon chewing. c) thermal sensitivity. d) discomfort, particularly on palpation. Question 4=c.")
61
8)Which of the following are contraindication to endodontic therapy
a) a non restorable tooth. b) a tooth with insufficient periodontal support. c) a tooth with vertical tooth fracture. d) all of the above. Question 8=d
 a non restorable tooth. b) a tooth with insufficient periodontal support. c) a tooth with vertical tooth fracture. d) all of the above. Question 8=d.")
62
10) Which of the following the is the main function of dental pulp :
a) nutritive . b) formative. c) sensory. d) protective. Question 10=b
 nutritive . b) formative. c) sensory. d) protective. Question 10=b.")
63
Pain on percussion before endodontic treatment indicates:
A. Reversible pulpitis. B. Irreversible pulpitis. C. Pulp necrosis. D. Inflammation of periodontal tissues. E. Exposed dentine. Key: D

64
In RCT, over preparation of the outer wall of the optical curvature of the canal with inflexible instrument will cause: A. Zipping. B. Perforation. C. Elbow formation. D. Ledge formation. E. Crazing.

65
Key: A

66
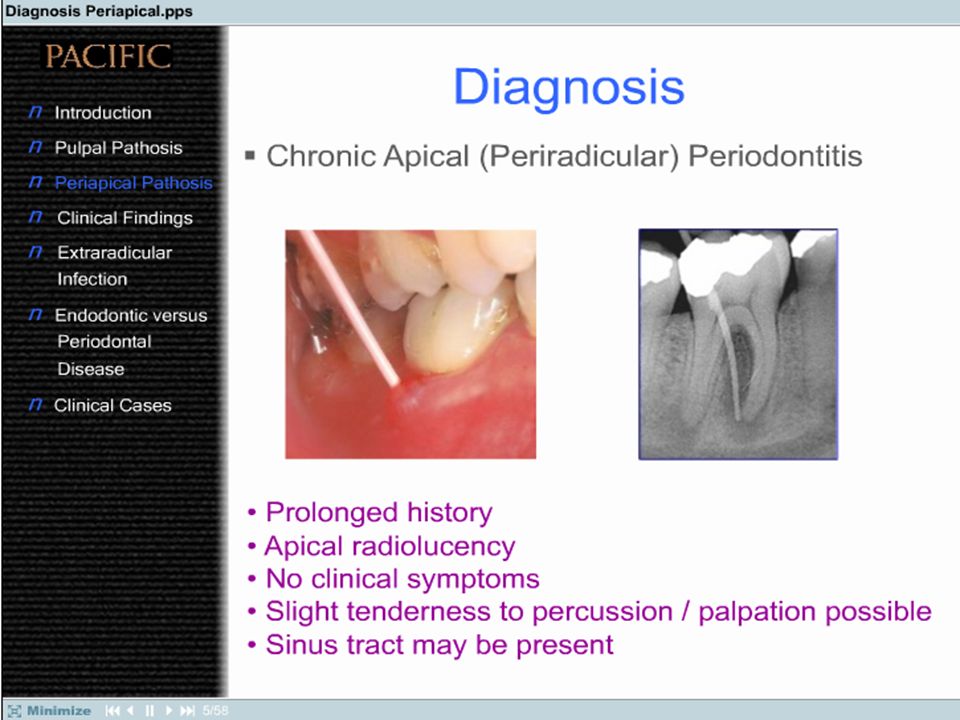
Diagnosis of Periapical Lesions
Distinguish between pulpal and pericpical disease. Discuss the effects of overinstrumentation and overfilling. Discuss the categories of periapical disease states, e.g. –AAP,AAA, CAP, Phoenix abscess and osteoscerosis, correlating the clincal disease state and the underlying microscopic features. Discuss a purely clinical classification for endodontic disease Discuss the dangers of periapical infection. Discuss history taking as it pertains to endodontic diagnosis and treatment. Distinguish between endodontic and periodontal infections. Diagnosing clinical cases – review via sample test questions.

67
The tip of the instrument is cutting which makes a reamer suitable for the preparation of straight canals only without the risk of ledging.

68
Danger zone is defined by Abou-Rass, Frank and Glick as the thin area in the root canal wall that is vulnerable to stripping by injudicious filling. Danger zone is located at mandibular first molar mesial root, 1.5mm below the furcation about 1.3mm thick on the distal surface. Both statements are true. Both statements are false. The first statement is true, second statement is false. The first statement is false, second statement is true.

69
The danger zone where care needs to be taken in order to avoid strip perforation.
Answer: a

70
A patient presents wet a draining sinus tract in labial vestibule of a maxillary central incisor. To confirm your diagnosis about the origin of pathoses you should: A. Open the concerned root chamber. B. Taking the bite-wing radiograph. C. Thread gutta-percha through the root canal and expose the radiograph. D. Thread the gutta-percha through the tract and expose a radiograph. E. Measure the periodontal packet.

71
Key: D

73
The pulp chamber in milk teeth in proportion to that of permanent teeth is :
A. Bigger in milk teeth. B. Smaller in milk teeth. C. Same in both teeth. D. Absent in milk teeth. E. Less vascular in milk teeth. Key: A

74
Recapitulation is: A. Uses successively larger files to flare the canals. B. Removing the debris with smaller instruments than the instruments that go to apex. C. Circumferential filing with H files. D. Using various types of files and reamers to enlarge canals. E. Irrigation of canals with sodium hypochlorite. Key: B

76
Canal patency must be maintained at all times.
This is accomplished, after each successively larger file, by irrigating and then returning to a file smaller than the file which prepared the apical portion of the canal (No. 15 is frequently used).
.")
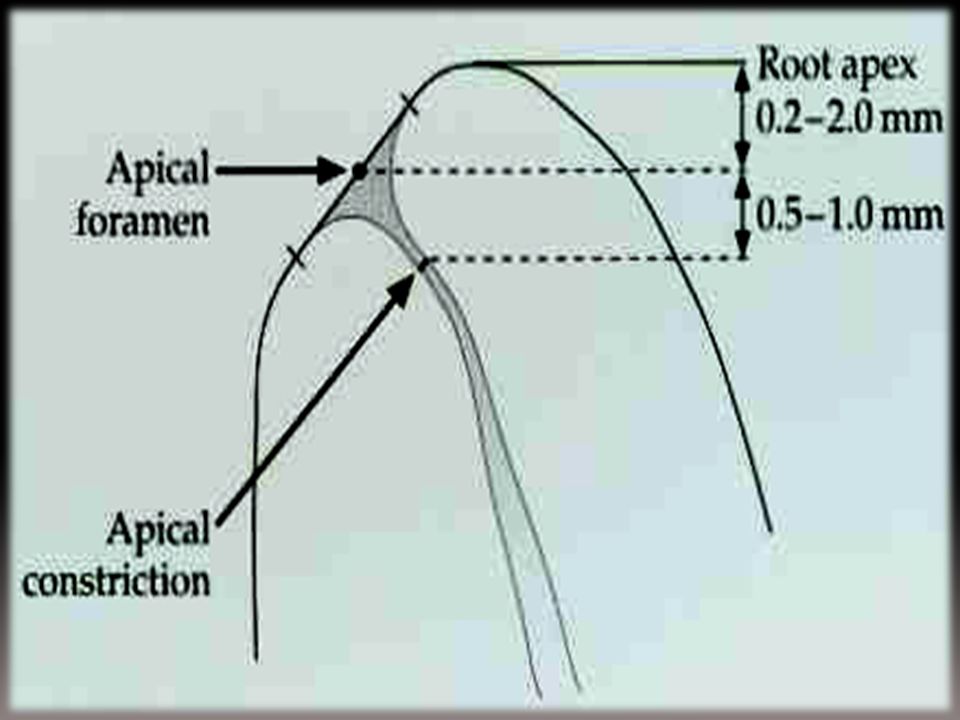
77
Apical patency A patency file is a small flexible instrument (08, 10) that will move passively through the terminus of a root canal without binding or enlarging the apical constricture. The aim is to prevent apical blockage, which will, in turn, reduce the incidence of ledge formation and transportation of the root canal. The use of a patency file also helps remove vital or necrotic pulpal remnants from the end of the canal. To use a patency technique, therefore, infers an intention to clean to the full canal length.
 that will move passively through the terminus of a root canal without binding or enlarging the apical constricture. The aim is to prevent apical blockage, which will, in turn, reduce the incidence of ledge formation and transportation of the root canal. The use of a patency file also helps remove vital or necrotic pulpal remnants from the end of the canal. To use a patency technique, therefore, infers an intention to clean to the full canal length.")
78
Biologically active sealer which promote peri-apical healing contain:
A. 2nO Engenol. B. Cortico-steroids. C. Ca(OH)2. D. Silver-points. E. Zinc phosphate. Key: C
2. D. Silver-points. E. Zinc phosphate. Key: C.")
79
Calcium hydroxide low solubility in water high pH (approximately 12.5–12.8) insoluble in alcohol Calcium hydroxide paste kills bacteria by direct contact through pH effects

80
The release and diffusion of hydroxyl ions (OH-) leading to a highly alkaline environment which is not conducive to the survival of micro-organisms. The role of calcium ions in cell stimulation, migration, proliferation and mineralization is well established. Calcium hydroxide also inactivates LPS and in so doing can assist periapical tissue repair.

81
• Biocompatibility (due to its low solubility in water and limited diffusion),
• The ability to encourage periapical hard tissue healing around teeth with infected canals • Inhibition of root resorption and stimulation of periapical healing after trauma.

89
Anesthetic testing is most effective in localizing pain to which of the following?
a. Specific tooth b. Mandible or maxilla c. Across the midline of the face d. Posterior tooth

90
Irreversible pulpitis is often defined by which of the following?
a. Moderate response to percussion b. Painful, lingering response to cold c. Short, painful response to cold d. Short, painful response to heat

91
The majority of patients with symptoms of severe odontogenic pain have a diagnosis of which of the following? a. Periodontal abscess b. Irreversible pulpitis c. Acute apical periodontitis d. Acute apical abscess

92
The best approach for diagnosis of odontogenic pain is which of the following?
a. Radiographic examination b. Percussion c. Visual examination d. A step-by-step, sequenced examination and testing approach

93
Of the following, which is the most likely to have referred pain?
a. Irreversible pulpitis b. Reversible pulpitis c. Acute apical periodontitis d. Phoenix abscess

94
Which of the following statements regarding a test cavity is accurate?
a. It is the first test in diagnostic sequence. b. It often results in a dull-pain response. c. It is used when all other test findings are equivocal. d. It should be performed with local anesthetic.

95
Percussion of a tooth is a test for which of the following?
a. Pulpal inflammation b. Pulpal necrosis c. Acute periradicular inflammation d. Chronic periradicular inflammation

96
Pulp stones are consistent indicators of which of the following?
a. Periodontal inflammation impacting the pulp b. Pulpal inflammation c. Older patient d. Pulp that has been injured in the past but has recovered e. None of the above

97
Which of the following statements regarding the degree of pulp pathosis is accurate?
a. It can be determined by the level of pain a patient experiences. b. It can be related to the level of response of the electrical pulp tester. c. It can be correlated best when a diagnosis of irreversible pulpitis is established. d. It does not correlate well with the level of pain a patient perceives.

98
A key measure as to the degree (i. e
A key measure as to the degree (i.e., intensity) of pain is to determine which of the following? a. Painful stimulus with cold b. Painful stimulus with heat c. Painful stimulus on biting d. Increasing pain e. Pain affecting patient's lifestyle
 of pain is to determine which of the following a. Painful stimulus with cold. b. Painful stimulus with heat. c. Painful stimulus on biting. d. Increasing pain. e. Pain affecting patient s lifestyle.")
99
In describing the sensory innervation of the dental pulp, which of the following statements is accurate? a. A-delta fibers are high-threshold, myelinated fibers that transmit sharp, momentary pain. b. C fibers are low-threshold, unmyelinated fibers that produce pain in response to inflammatory mediators. c. The domination of C-fiber stimulation produces pain that is not well localized. d. The sharp, well-localized pain to cold testing is conducted by both A-delta and Cfiber stimulation.

100
Which of the following most likely indicates pain that is not of pulpal origin?
a. Unilateral pain that radiates over the face to the ear b. Pain that has paresthesia as a component c. Pain that is described as throbbing and intermittent d. Pain that is increased during mastication

101
Treatment of severe, throbbing pain associated with the maxillary, left, first molar(tooth no. 14) is best managed by which of the following? a. Pulpotomy b. Partial pulpectomy c. Pulpectomy d. Analgesic agents e. Analgesic and antibiotic agents

102
Which of the following statements regarding leaving a tooth open for drainage in cases of an acute, apical abscess is accurate? a. It is the recommended method of managing the emergency patient. b. It may adversely affect the outcome of treatment. c. It is appropriate, providing the patient is also placed on an antibiotic.

103
Elective endodontic treatment is contraindicated in which of the following?
a. Patient is a borderline diabetic. b. Patient has had a heart attack within the last 6 months. c. Patient has had numerous opportunistic infections secondary to HIV infection. d. Patient has an implanted pacemake

104
When is endodontic treatment is contraindicated?
a. The patient has no motivation to maintain the tooth. b. The canal appears to be calcified. c. A large periapical lesion is present. d. The tooth needs periodontal crown lengthening before restoration.

105
A preoperative finding that predisposes to a decreased prognosis (i. e
A preoperative finding that predisposes to a decreased prognosis (i.e., lowersuccessrate) is which of the following? a. The tooth is in hyperocclusion. b. The pulp is vital. c. The pulp is necrotic with no periradicular lesion. d. The pulp is necrotic with a periradicular lesion present. e. Treatment is in an elderly patient.
 is which of the following a. The tooth is in hyperocclusion. b. The pulp is vital. c. The pulp is necrotic with no periradicular lesion. d. The pulp is necrotic with a periradicular lesion present. e. Treatment is in an elderly patient.")
Similar presentations
>")









. All rights reserved. Endodontics Chapter 54 Copyright 2003, Elsevier Science (USA). All rights reserved. No part.>")








