Download presentation
Presentation is loading. Please wait.

1
Canal Preparation Techniques

2
The primary goal of all these techniques is:
to shape the canals to the apical constriction of the canal space, regardless of the radiographic appearance of the actual tooth

3
the step-back technique
Telescopic or serial root canal preparation This instrumentation technique forms an apical stop and thereby avoids irritation of the periapical tissues by medicaments or filling material. Because there is very little canal enlargement and removal of dentin near the apex, the danger of perforation is reduced.

4
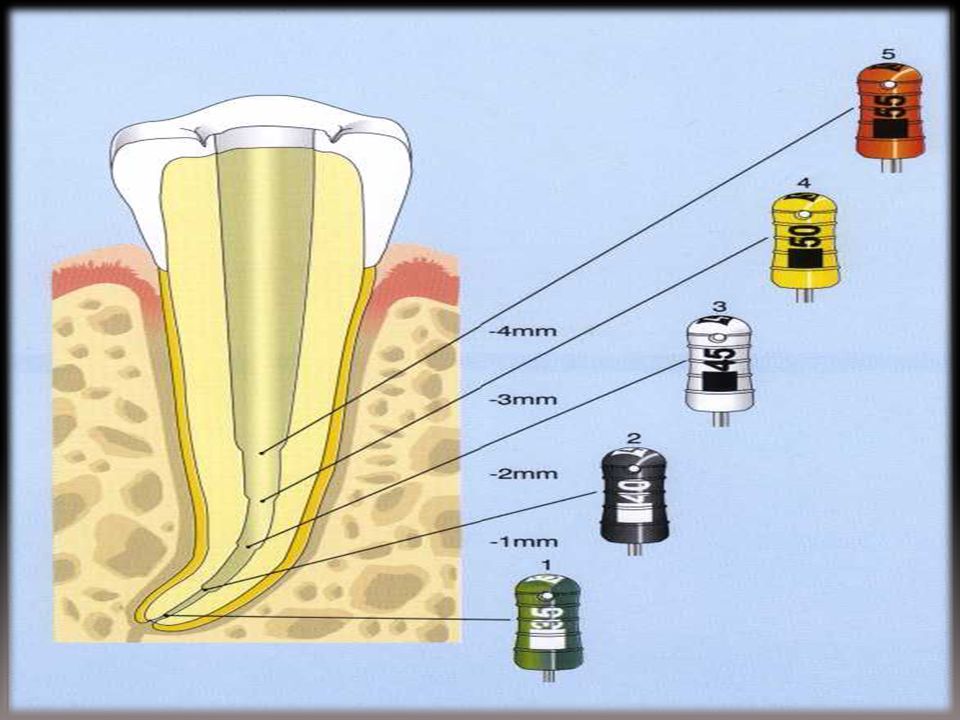
At the beginning of instrumentation, the length of the canal and the size of the initial apical file (IAF) are determined on a radiograph Starting with the IAF, the root canal is enlarged to the working length through four file sizes.

5
Step-back technique After the root canal has been enlarged throughout its entire length to the size of the apical master file, the subsequent files are each made 1 mm shorter than the previous file. The drawing clearly shows the tapered root canal preparation that is formed by this procedure. The steps are smoothed by the intermittent reintroduction of the AMF. This simultaneously prevents blockage of the apical canal by dentin chips and verifies accessibility to the apical constriction. K files are used exclusively in this preparation technique.

8
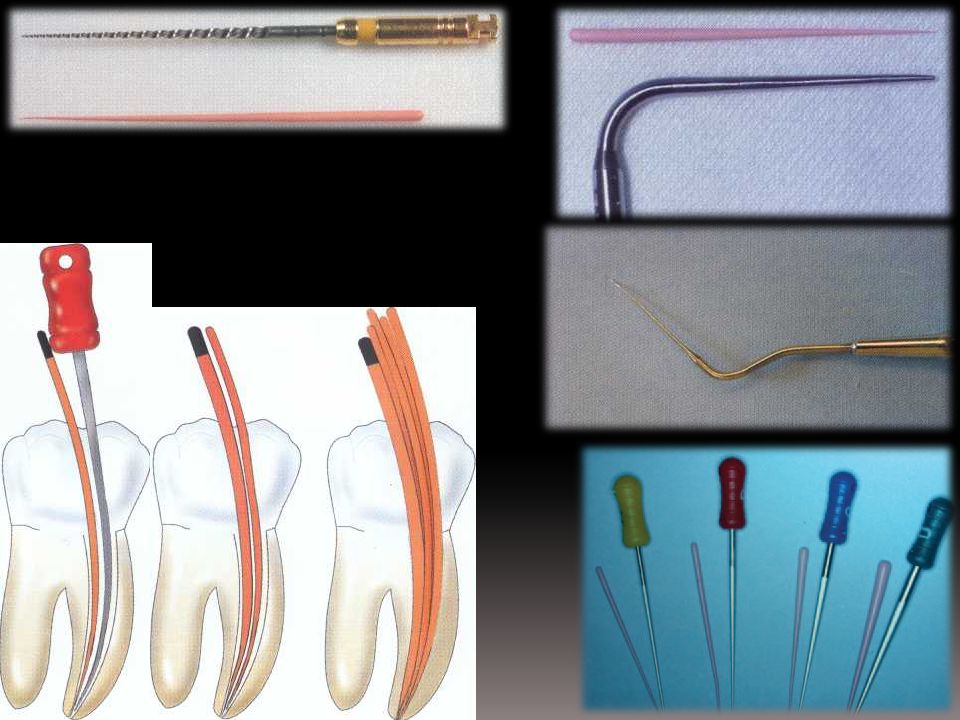
In the step-back technique, the apical portion is instrumented first, and then the coronal portion is shaped. After the access opening is made, the working length is determined on a measurement radiograph. The first file that binds in the canal at the working length is considered (the initial apical file IAF). The root canal must then be enlarged by circumferential filing through an additional four instrument sizes. During this initial phase of preparation, no instrument sizes may be skipped or a blockage may be created.
. The root canal must then be enlarged by circumferential filing through an additional four instrument sizes. During this initial phase of preparation, no instrument sizes may be skipped or a blockage may be created.")
9
The last file manipulated to the working length should remove only white dentin shavings, and is designated the apical master file (AMF). Its size determines the size of the gutta-percha master point that will be used later. Next, the coronal portion of the root canal is instrumented in step-back fashion through four additional sizes. Each subsequent larger size K file is set I mm shorter than the preceding size so that a conical canal configuration with a definite apical stop is formed. Frequent recapitulation with the AMF ensures that the canal remains patent.

10
Recapitulation Canal patency must be maintained at all times.
This is accomplished, after each successively larger file, by irrigating and then returning to a file smaller than the file which prepared the apical portion of the canal (No. 15 is frequently used). Irrigation is used between each file also to remove debris. Failure to recapitulate will result in canal blockage. Frequently blockage can be difficult to clear and attempts to do so may result in a ledge or even perforation
. Irrigation is used between each file also to remove debris. Failure to recapitulate will result in canal blockage. Frequently blockage can be difficult to clear and attempts to do so may result in a ledge or even perforation.")
11
Apical patency A patency file is a small flexible instrument (08, 10) that will move passively through the terminus of a root canal without binding or enlarging the apical constricture. The aim is to prevent apical blockage, which will, in turn, reduce the incidence of ledge formation and transportation of the root canal. The use of a patency file also helps remove vital or necrotic pulpal remnants from the end of the canal. To use a patency technique, therefore, infers an intention to clean to the full canal length.
 that will move passively through the terminus of a root canal without binding or enlarging the apical constricture. The aim is to prevent apical blockage, which will, in turn, reduce the incidence of ledge formation and transportation of the root canal. The use of a patency file also helps remove vital or necrotic pulpal remnants from the end of the canal. To use a patency technique, therefore, infers an intention to clean to the full canal length.")
12
Glide Path (Canal Patency) Canal Shaping (Repeat until 25 to WL)
")
13
Step-Down Technique Narrow, curved root canals are prepared by means of the coronal-apical ("crown down") instrumentation technique. In this method the coronal portion is enlarged first, and only then is the apical region of the root canal prepared. An advantage of this technique over the apical-coronal technique is that the coronal enlargement makes it possible to insert the irrigating canula quite deeply into the root canal. During the final instrumentation of the apical region necrotic pulp tissue is thus loosened and flushed away with sodium hypochlorite.

14
After the access preparation is made, the canal preparation is begun by assuring complete patency of the canal. This is done by inserting a size 15 Hedstrom file, employing one-eighth circle rotations and only light pressure. Next the root canal is enlarged coronally with a Gates-Glidden drill to the beginning of the canal's curvature using the step-back technique. It is important to coat the tip of the instruments with a lubricant (e. g. RC-Prep) in order to prevent binding within the canal.
 in order to prevent binding within the canal.")
15
Following enlargement of the coronal portion, the working length is determined radiographically with a size 15 K file in place. If the instrument tip falls more than 2 mm short, a second measurement radiograph is made after further careful instrumentation. If the root canal is too narrow to allow the K file to be inserted to the working length, passage to the apex must be carefully established with a Hedstrom file also. Only then can the size of the initial apical file be determined and the canal enlarged by four sizes.

16
Apical preparation is accomplished by alternating instruments-first a Hedstom file is used for circumferential filling and this is followed by a K file (noncutting tip) in a rotating working movement (balanced force technique). Following this, the canal is widened coronally with a size 20 Hedstrom file, and finally the entire root canal is instrumented to the working length with a prebent size 20 K file. If this file does not reach the working length, under no circumstances should any attempt be made to advance the instrument apically by rotating it.

17
Balanced force: The root canal is enlarged along its entire length by using the balanced force technique: first the instrument is introduced into the canal with rotations to the right. Then the file is rotated to the left to cut dentin from the canal wall.

18
A prebent K file prior to apical instrumentation.
The instrument has become slightly straightened after being rotated apically.

19
Creating a conical form:
Following preparation of the apical region, the canal is tapered by circumferential filing with Hedstrom files.

20
Finally, the entire canal is smoothed by using the #35 AMF with balanced force rotations.

21
Root Canal Obturation The last step in root canal treatment is to create the best possible hermetic seal with a filling material that is nonirritating to the tissues. The basic mechanical instrumentation and shaping of the canal is the most important prerequisite for endodontic success. The root canal filling should leave the tooth in the most biologically inert condition possible, and it must prevent reinfection as well as growth of any microorganisms remaining in the canal Filling the root canal with gutta-percha points and a sealer is the most biologically favorable and surest method in the long term

22
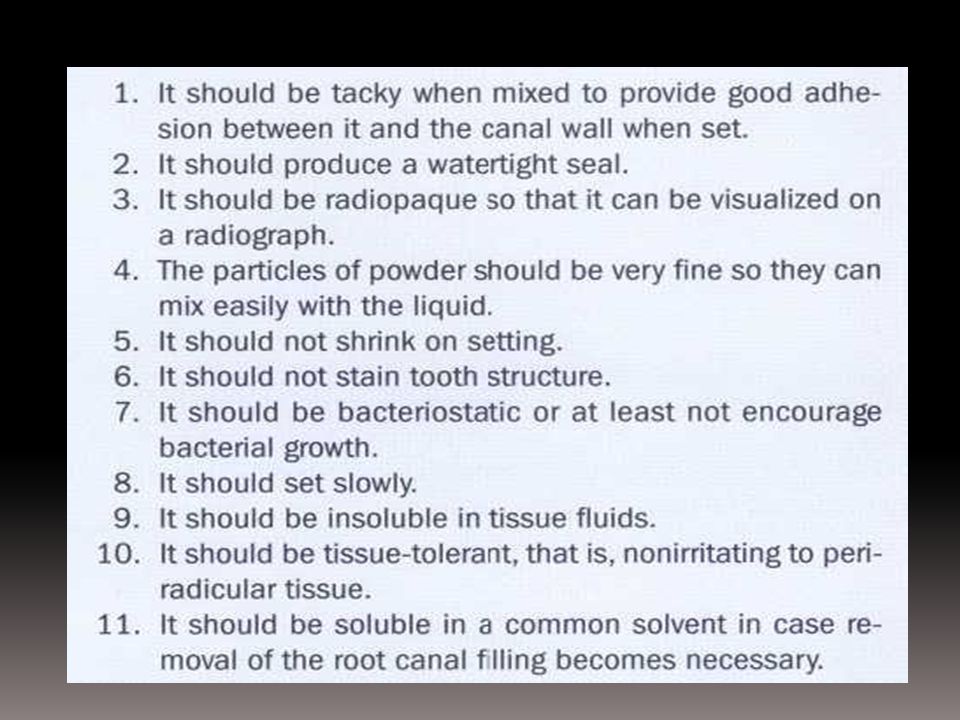
The ideal root canal filling material :
Nonirritating to the pulp tissue. Tightly seal the canal both laterally and vertically. Dimensionally stable so as not to shrink within the canal. Should not support bacterial growth and should even be bacteriostatic. Biologically compatible and nontoxic. Easy to sterilize before use. Radiopaque . Should not discolor the tooth. Should not harden too quickly and after hardening should exhibit good adhesion to both the dentin and the root canal filling. Insoluble in tissue fluids and have a slight expansion.

23
– Easily manipulable with ample working time
– Easily mixable in very fine powder particles and liquid form – Taky when mixed and adhesive to the canal walls – Biocompatible – Expansible while setting – Absolutely inert – Physically stable (unshrinkable after setting) – Non-resorbable – Insoluble in tissue fluids – Radiopaque – Not staining the tooth structure – Bacteriostatic – Easily removable with common solvents, if necessary – Non-immunogenic in the periapical tissues 8,10,152 – Neither mutagenic nor carcinogenic
 – Non-resorbable. – Insoluble in tissue fluids. – Radiopaque. – Not staining the tooth structure. – Bacteriostatic. – Easily removable with common solvents, if necessary. – Non-immunogenic in the periapical tissues 8,10,152. – Neither mutagenic nor carcinogenic.")
26
Lateral Condensation of Gutta-percha
The root canal filling procedure starts with the selection of the gutta-percha master point. Before the gutta-percha master point is tried in the canal, a suitable spreader is selected.

27
The apical half of the master point is coated with sealer and inserted into the canal to the predetermined depth. The cement is mixed and given the spatula test to determine the desired consistency.

28
Root canal cement should be mixed to a thick, creamy consistency that may be strung off the slab for 2.5 cm (1 inch).
.")
29
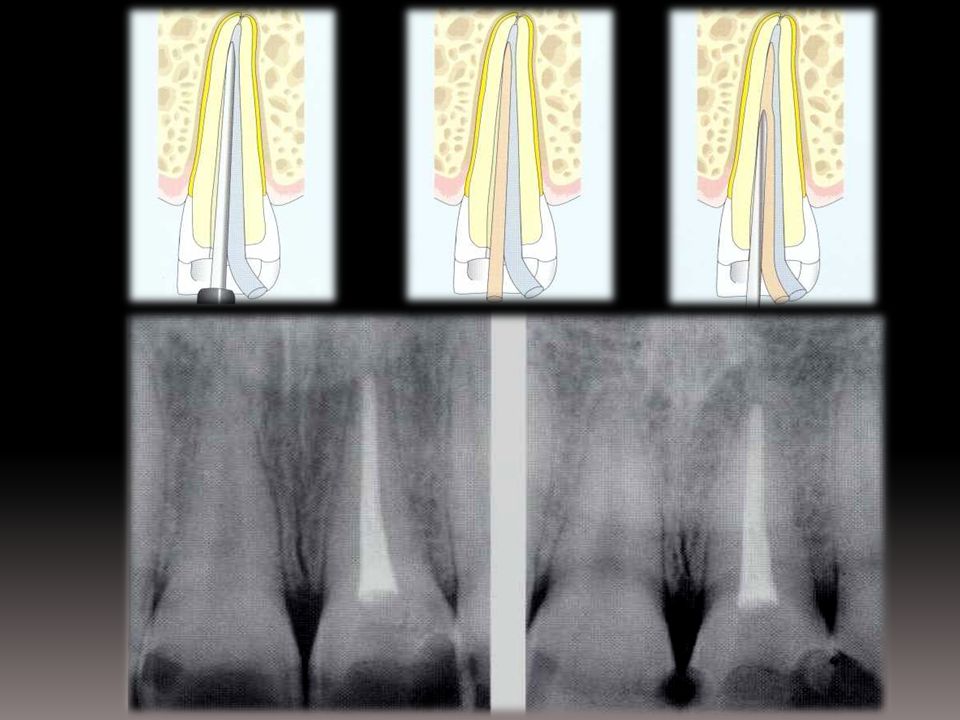
The spreader has been tested previously to reach within 1 mm of the apical constriction. A thin layer of sealer lines the canal walls, and the tip of the primary point is coated with cement. The primary point is carried fully to place to within 1 mm of the “apical stop.” Excess in the crown is severed at the cervical with a hot instrument. The spreader is inserted to the full depth, allowed to remain 1 full minute as gutta-percha is compacted laterally and somewhat apically.

30
A master point is selected that allows a friction fit in the apical portion of the root canal.
When this is marked it is called 'tug back' (like pulling a dart out of a dart board). This may be difficult to achieve with small size gutta-percha points; therefore, it is usual to accept a friction fit in narrow canals. A point one size larger than the master apical file is usually selected.
. This may be difficult to achieve with small size gutta-percha points; therefore, it is usual to accept a friction fit in narrow canals. A point one size larger than the master apical file is usually selected.")
31
If it is not possible to place the point to working length, select a point that passes to full length and trim 0.5 mm off the end using a scalpel (this has the effect of making the point slightly larger). Retry the point and adjust as necessary.

32
Mark the length of the point by nipping it with tweezers at the reference point and take a check radiograph with the cone in place.

33
The spreader is removed by rotation and immediately replaced by the first auxiliary point previously dipped in sealer. The spreader is returned to the canal to laterally compact the mass of filling. Secondary vertical compaction seals the apical foramen. The spreader is again removed, followed by the matching auxiliary point. The process continues until the canal is totally obturated. All excess gutta-percha and sealer are removed from the crown to below the free gingival level. Vertical compaction with a larger plugger completes root canal filling.

35
Cut off the gutta-percha 1 mm below the cementoenamel junction or gingival level (whichever is the more apical) using a hot instrument and vertically condense the gutta-percha. This is important as remaining root-filling material may stain the tooth.

36
The finger spreader is inserted between the canal wall and the point to a depth 1 mm short of the working length. When the working length is reached, the spreader is left in place for 15 seconds before being withdrawn. This will prevent rebounding of the gutta-percha The accessory point, coated with a small amount of sealer, is condensed against the master point with the finger spreader.

38
Once the fit of the gutta-percha master point has been verified radiographically, it is removed from the canal, rinsed, and dried. Then the AMF is inserted into the dried root canal and, using balanced force rotating movements, a few more dentin shavings are removed. In one-third of root canals studied, less than 50% of the walls in the apical third were covered with sealer.

39
The sealer does not coat the wall uniformly, regardless of the method used to carry it into the canal. When the sealer was introduced on a K file, which was then removed while being rotated counterclockwise, only one-third of the canal walls were covered. Application with an ultrasonic file did not improve the results. The sealer could be applied well in half of the cases with a Lentulo spiral. When the gutta-percha point was coated with sealer and pushed into the canal, the highest success rate was observed at 70%.

Similar presentations