Download presentation
Presentation is loading. Please wait.

1
Inflammatory Bowel Disease
Dr. Hagit Tulchinsky, Proctology Unit, Surgery B Tel Aviv Sourasky Medical Center

2
Epidemiology Developed countries
More common in Jewish population (3-5 folds), whites Equal distribution between genders Bimodal age distribution: 15-35y, 50-70y
, whites. Equal distribution between genders. Bimodal age distribution: 15-35y, 50-70y.")
3
Etiology-1 UC and Crohn`s – separate entities ?
10-15% of IBD - Indeterminate colitis 10% - diagnosis is changed Relatives – more likely to have the same disease as the proband Cluster within families

4
Etiology-2 Genetic predisposition + environmental factors (dietary intake) Complex genetic disorder UC - less significant genetic contribution than in Crohn`s d. Susceptibility locus, IBD 1, on chromosome 16 Molecular evidence of 2 forms of Crohn`s pANCA – in most UC patients (75%)
")
5
Etiology-3 Host – defective mucosal barrier function
NSAID`s exacerbate IBD Cigarette smoking: protective in UC, aggressive factor in Crohn`s d.

6
Etiology- Summary These diseases are due to aberrant host response to environmental antigens in genetically susceptible individuals

7
Pathology-UC-1 congested serosa From rectum proximally
Confined to colon and rectum Disease limited to the mucosa Macroscopic appearance congested serosa contracted and shortened bowel edema of the mesentery pseudopolyps 10% backwash ileities

8
Pathology-UC-2 Only the mucosa is affected Microscopic appearance
Cancer and dysplasia 3-5% develop cancer Increased risk if extensive disease for at least 8 years Surgery if low grade dysplasia

9
Pathology Crohn`s disease-1
May affect any part of the intestinal tract Usually affects the terminal ileum and cecum Small bowel alone – 1/3 Colon alone – 1/3 Perianal region or upper GI tract alone – less common

10
Pathology Crohn`s disease-2
Macroscopic appearance Skip lesions Segmental colitis Stenosis of terminal ileum Anal lesions in 75% Wrapping of mesenteric fat Thickened wall irregularly Thickened mesentery

11
Pathology Crohn`s disease-3
Microscopic appearance Patchy distribution 2/3 – noncaseating granulomas, Transmural chronic inflammation, Serositis, fibrous adhesions Deep ulcers into the muscle layers Cancer and dysplasia Increased risk in long standing disease

12
Pathology-Summery Pathologic features – more usually seen in chronic stages of the disease Cardinal feature of Crohn`s d. - patchiness The presence of small bowel disease should exclude UC High or complex perianal fistula / anal ulceration – more likely Crohn`s d. Crypt distortion – characteristic of UC Granulomas are less specific

13
Clinical findings Diarrhea, mucous discharge Rectal bleeding- more UC
Obstructive symptoms- more Crohn’s d. Anal/perianal d.- more Crohn’s d. Loss of body weight Anemia

14
Physical findings Reflect the severity of the disease
Abdominal tenderness (left side) Abdominal distention Fever, tachycardia Proctitis- urgency, tenesmus, fecal incontinence
 Abdominal distention. Fever, tachycardia. Proctitis- urgency, tenesmus, fecal incontinence.")
15
Extraintestinal manifestations
Peripheral arthritis, 15-20%, resolve after colectomy Ankylosing spondylitis Sacroiliitis Primary sclerosing cholangitis – more in UC, no resolution post op

16
Surgery-UC 20-45% eventually undergo surgery
Indications – elective / emergency Pre op. management: - Correct hypovolemia + electrolytes - Correct anemia - If on steroids – Hydrocortisone I.V. - Counseling and education on the outcome - Severe malnutrition – TPN - Prepare as for colon surgery

17
Indications for elective surgery UC
Intractability – most common Involvement of other organs Large bowel dysplasia/cancer

18
Indications for elective surgery UC
Intractability Failure of medical therapy Chronic complications of the disease Debilitating symptoms Poor nutrition Impaired quality of life Anemia Hypoproteinemia Children- failure to growth Side effects

19
Indications for elective surgery UC
Presence and risk of cancer When to consider prophylactic surgery/close surveillance program? Extensive and long standing colitis Onset at childhood/teenage + generalized colitis +10 or more yrs of disease – 2% will develop cancer each year PSC Dysplasia

20
Indications for elective surgery UC
Debilitating extra intestinal manifestations May improve after surgery Cutaneouos, peripheral arthicular, ocular, hematological,vascular Ankylosing spondilitis and rheumatoid arthritis will not regress PSC may progress to cirrhosis or cholangio ca. after surgery

21
Indications for emergency surgery UC
Fulminant colitis Tachycardia, fever, WBC > 10,500, low albumin First – aggressive conservative treatment Failure – surgery Goal – operate before colonic perforation Toxic megacolon Pain, fever, toxicity, abdominal tenderness and distention, transverse colon >7cm Perforation, hemorrhage and obstruction

22
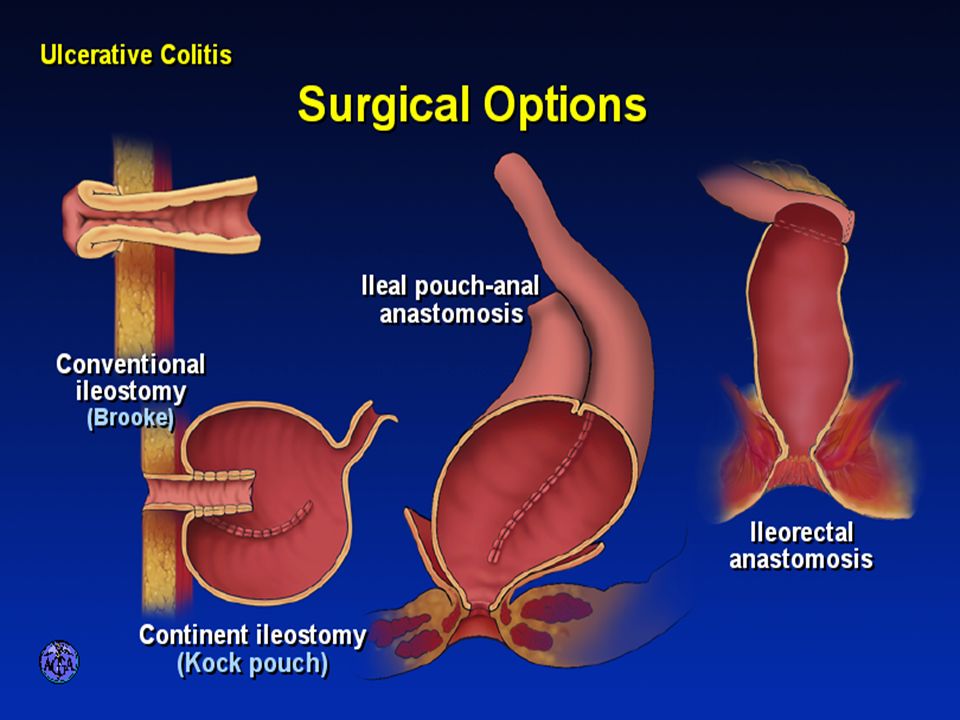
Choice of Operation-UC
Restorative proctocolectomy Treatment of choice if elective CI – Crohn`s, incompetent sphincter, cancer in distal rectum Proctectomy with continent ileostomy Brooke ileostomy, poor sphincter Proctectomy with Brooke ileostomy Colectomy and ileorectal anastomosis Rarely used today only if relative rectum sparing, young males

23
Normal anatomy

24
Proctocolectomy

25
Colectomy with ileorectal anastomosis

27
Elective treatment of choice
Choice of Operation Elective treatment of choice Restorative proctocolectomy with ileal reservoir The ileal pouch anal anastomosis

28
The pouch procedure Removes all of the colon and rectum
Preserves the anal canal Aim – to avoid permanent ileostomy The decision is up to the patient Information on the pros and cons

29
The pouch procedure WHO IS ELIGIBLE ?
Ulcerative colitis and not Crohn`s disease Patients who had no operation Patients who had a colectomy with ileostomy or ileorectal anastomosis Good anal sphincter control

30
The pouch procedure Technique
Stage 1- The pouch operation Abdomen opened Colon and rectum are freed Rectum is cut above the anal sphincter Small bowel and anus left in place

31
Abdominal incision

32
Proctocolectomy

33
The pouch procedure Technique
Stage 1- The pouch operation J pouch Pouch joined to the anus Protective loop ileostomy

34
ILEAL POUCH-ANAL ANASTOMOSIS
The ileal pouch-anal anastomosis (IPAA) has become the conventional operation for ulcerative colitis with 90% of procedures for ulcerative colitis in many series involving IPAA. The operation can be done as a primary two stage procedure, a total procto-colectomy, and IPAA with temporary loop ileostomy, multistage with subtotal colectomy, oversow of rectal stump, and ileostomy followed by completion proctectomy and loop ileostomy closure or as a one stage procedure without loop ileostomy. The procedure can be done by a total mucosal proctectomy with hand suturing of the pouch to the anal canal or by leaving the anal transitional zone with stapling of the pouch to the anal canal. Long-term follow-up of pouch function and quality of life have indicated a high degree of success with an acceptable rate of complications. The standard Brooke ileostomy and in limited situations a straight ileal-rectal anastomosis continue to be important alternative to IPAA for some patients with ulcerative colitis. • Remzi FH, Fazio VW. Ileal anal pouch anastomosis. In: Bayless TM, Hanauer SB. eds. Advanced Therapy of Inflammatory Bowel Disease. London, BC Decker Inc., 2001; • Fazio VW, O’Riordon MG, Lavery IC et al. Long-term functional outcome and quality of life after stapled restorative procto-colectomy. Ann Surg 1999;230: • McIntyre PB, Pemberton JH, Wolff BG et al. Comparing functional results one year and 10 years after ileal pouch anal anastomosis for chronic ulcerative colitis. Dis Colon Rectum 1994;37:303-7.
 has become the conventional operation for ulcerative colitis with 90% of procedures for ulcerative colitis in many series involving IPAA. The operation can be done as a primary two stage procedure, a total procto-colectomy, and IPAA with temporary loop ileostomy, multistage with subtotal colectomy, oversow of rectal stump, and ileostomy followed by completion proctectomy and loop ileostomy closure or as a one stage procedure without loop ileostomy. The procedure can be done by a total mucosal proctectomy with hand suturing of the pouch to the anal canal or by leaving the anal transitional zone with stapling of the pouch to the anal canal. Long-term follow-up of pouch function and quality of life have indicated a high degree of success with an acceptable rate of complications. The standard Brooke ileostomy and in limited situations a straight ileal-rectal anastomosis continue to be important alternative to IPAA for some patients with ulcerative colitis. • Remzi FH, Fazio VW. Ileal anal pouch anastomosis. In: Bayless TM, Hanauer SB. eds. Advanced Therapy of Inflammatory Bowel Disease. London, BC Decker Inc., 2001; • Fazio VW, O’Riordon MG, Lavery IC et al. Long-term functional outcome and quality of life after stapled restorative procto-colectomy. Ann Surg 1999;230: • McIntyre PB, Pemberton JH, Wolff BG et al. Comparing functional results one year and 10 years after ileal pouch anal anastomosis for chronic ulcerative colitis. Dis Colon Rectum 1994;37:")
36
The pouch procedure Technique
Stage 2 – Closure of ileostomy Relatively minor procedure Cut around the ileostomy Bowel closed The hole in the abdomen closed

37
The pouch procedure Results
Early complications Obstruction Infection

38
The pouch procedure Results
Late complications Obstruction Pouchitis Defecation problems Anal skin soreness Pouch fistula

39
The pouch procedure Results
Function Frequency Urgency Continence Anti diarrheal medications

40
The pouch procedure Results
Quality of life 90% - better Failure Up to 15%

41
Surgery Crohn`s disease
Typical presenting symptoms: Abdominal pain, diarrhea, weight loss Reserved for patients whose quality of life is significantly impaired despite appropriate medical therapy or after disease associated complications develop The probability of undergoing surgery is 78-90% after 20 and 30 yrs, respectively Elective / emergent indications

42
Indications for elective surgery Crohn`s disease
Fistula ± abscess The most common indication Different types of fistula Rarely heal with corticosteroids 6-MP will promote closure in 30-40% Obstruction Chronic/acute Single/multiple sites of stricture

43
Indications for elective surgery Crohn`s disease
Failed medical therapy Incomplete response Maintenance medications cannot be stopped Significant side effects Intra abdominal abscess/fistula Carcinoma Growth retardation 15-30% of children with Crohn`s Op. is indicated only in the pre pubertal child

44
Indications for emergency surgery Crohn`s disease
Fulminant colitis and Toxic megacolon Acute flare and at least 2 of the following: Tachycardia >100 , fever >38.6, WBC > 10,500, albumin<3 Initial therapy –correct physiological deficits, high dose steroids or immunosuppresants, bowel rest, antibiotics Any worsening during the initial 48h - surgery Free perforation, massive hemorrhage, peritonitis, septic shock – emergent op.

45
Indications for emergency surgery Crohn`s disease
Perforation Most are sealed Massive bleeding Rare – 1% of patients of patients

46
Principles of operative treatment Crohn`s disease
PALLIATIVE, CONSERVATISM Minimal procedure with maximal effect Mechanical and antibiotic preparation I.V. Steroids Stop immunosuppressive therapy Correction of deficits Stoma marking of patients

47
Operative options Crohn`s disease
Bypass Rarely recommended – high recurrence rate and malignancy risk Resection Macroscopic healthy margins Anastomosis Stapled or handsewn Same principles as for any anastomosis of patients

48
Operative options Crohn`s disease
Stricturoplasty - Small bowel strictures, fibrotic recurrence at ileocolic or ileoractal anastomosis - Not for colonic narrowing - Indications and contra indications - Technique of patients

49
STRICTUROPLASTY (HEINEKE-MIKULICZ)
For short strictures (less than or equal to 10 cm), a Heineke-Mikulicz technique is employed. This involves a linear anti-mesenteric incision extending about 2 cm beyond the stricture proximally and distally. The mucosa is biopsied to exclude unrecognized malignancy. Stay sutures and lateral traction are applied to convert the longitudinal enterotomy into a transverse defect. The wound is then closed transversely. • Strong, SA. Surgery for Crohn’s disease: Stricturoplasty. In: Bayless TM, Hanauer SB. eds. Advanced Therapy of Inflammatory Bowel Disease. London, BC Decker, Inc., 2001;pp:
, a Heineke-Mikulicz technique is employed. This involves a linear anti-mesenteric incision extending about 2 cm beyond the stricture proximally and distally. The mucosa is biopsied to exclude unrecognized malignancy. Stay sutures and lateral traction are applied to convert the longitudinal enterotomy into a transverse defect. The wound is then closed transversely. • Strong, SA. Surgery for Crohn’s disease: Stricturoplasty. In: Bayless TM, Hanauer SB. eds. Advanced Therapy of Inflammatory Bowel Disease. London, BC Decker, Inc., 2001;pp:")
50
STRICTUROPLASTY (FINNEY)
The side-to-side stricturoplasty (Finney) is utilized for long strictures greater than 10 cm. This procedure requires that the intestine be supple enough to bend into a U-shape and still allow for a tension-free anastomosis. To initiate the Finney stricturoplasty, an incision is made along the anti-mesenteric margin. The intestine is then folded in a U-shape configuration. The posterior portion is closed with continuous sutures as is the anterior layer with inversion of the mucosal layer. Concerns about bacterial overgrowth in the diverticulum-like sac extending from the intestine, and about recurrent stricturing within the afferent limb just proximal to the diverticulum, have led to several proposed modifications of this technique. • Strong, SA. Surgery for Crohn’s disease: Stricturoplasty. In: Bayless TM, Hanauer SB. eds. Advanced Therapy of Inflammatory Bowel Disease. London, BC Decker, Inc., 2001;pp: • Faziio VW, Tjondra J. Stricturoplasty for Crohn’s disease with multiple long strictures. Dis Colon Rectum 1993;36:71-2. • Hurst RD, Michelassi F. Stricturoplasty for Crohn’s disease: techniques and long-term results. World J Surg 1998;22:
 is utilized for long strictures greater than 10 cm. This procedure requires that the intestine be supple enough to bend into a U-shape and still allow for a tension-free anastomosis. To initiate the Finney stricturoplasty, an incision is made along the anti-mesenteric margin. The intestine is then folded in a U-shape configuration. The posterior portion is closed with continuous sutures as is the anterior layer with inversion of the mucosal layer. Concerns about bacterial overgrowth in the diverticulum-like sac extending from the intestine, and about recurrent stricturing within the afferent limb just proximal to the diverticulum, have led to several proposed modifications of this technique. • Strong, SA. Surgery for Crohn’s disease: Stricturoplasty. In: Bayless TM, Hanauer SB. eds. Advanced Therapy of Inflammatory Bowel Disease. London, BC Decker, Inc., 2001;pp: • Faziio VW, Tjondra J. Stricturoplasty for Crohn’s disease with multiple long strictures. Dis Colon Rectum 1993;36:71-2. • Hurst RD, Michelassi F. Stricturoplasty for Crohn’s disease: techniques and long-term results. World J Surg 1998;22:")
51
Thank You

Similar presentations









 Kristina Blaslov Mentor: A. Žmegač Horvat.>")





 Idiopathic IBD is comprised of CD+UC and is characterized by chronic bowel inflammation. Idiopathic IBD is comprised of.>")




