Download presentation
Presentation is loading. Please wait.

1
Lobna Al Juffali, Msc fall 2010
Osteomyelitis Lobna Al Juffali, Msc fall 2010

2
osteomyelitis Osteomyelitis represents an acute or chronic infection of the bone. Osteo refers to bone, myelo refers to the marrow cavity, both of which are involved in this disease. 20 cases per 100,000 The annual incidence : in sickle cell patients is 0.36%. foot puncture 16% patients with Diabetes 30-40%

3
Introduction Osteomyelitis is an inflammation of the bone marrow and surrounding bone caused by an infecting organism. It can occur in any bone of the body and often leads to serious morbidity, even with early diagnosis and treatment. Despite the continued refinement of diagnostic procedures advances in antimicrobial therapy, and the use of prophylactic antibiotics before orthopedic procedures, osteomyelitis continues to be a serious problem from both a diagnostic and therapeutic standpoint.

4
Introduction Osetomylitis may be caused by a wide variety of microorganisms introduced during injury, during operative procedures, or from the bloodstream. Once localized in bone, the microorganisms proliferate, produce cell death, and spread within the bone shaft, inciting a chronic inflammatory response with further destruction of bone.

5
Bone Anatomy The bone is divided into three sections:
the epiphysis, located at the end of the bone; the metaphysis The diaphysis. Epiphyseal growth plate is the rapidly growing area of the bone that separate the epiphysis and metaphysis Surrounding most of the bone is a fibrous and cellular envelope. Periosteum is The external portion of this envelope Endosteum is the internal portion

6
Bone Anatomy

8
The difference in bone structure regarding to age :
Variations exist in the vasculature of bone in different age groups, leading to different forms of osteomyelitis. In neonates and adults, vascular communications are present between the epiphysis and metaphysis, which may allow infection to spread from the metaphysis to the epiphysis and the adjacent joint. However, during childhood, this area often is protected from infection because the epiphyseal plate separates the vascular supply for these two regions.

9
Classification of osteomyelitis depending on severity
Osteomyelitis can occur as an acute evolves over several days or weeks. Subacute chronic condition evolve over months or even years .

10
Microbiology bacteria viruses Parasites fungi,
but infections caused by certain pyogenic bacteria and mycobacteria are the most common.

11
Most common Bacteria Staphylococcus aureus is the most common cause
Escherichia coli, Neisseria gonorrhoeae Haemophilus influenzae, Salmonella species are also seen.

12
S. aureus has two characteristics that favor its ability to produce osteomyelitis:
it has the ability to produce a collagen-binding adhesion molecule that allows it to adhere to the connective tissue elements of bone (2) it has the ability to be internalized and survive in osteoblasts, making the microorganism more resistant to antimicrobial therapy
 it has the ability to be internalized and survive in osteoblasts, making the microorganism more resistant to antimicrobial therapy.")
13
Microorganism depending on site of infection

14
Microorganism depending on age
Likely etiology Host Staphylococcus aureus Group B streptococci Gram-negative bacilli Neonate S. aureus Haemophilus influenzae type b <3 yr S. Aureus ≥3 yr P. aeruginosa After puncture wound through shoe Salmonella sp Child with sickle cell

15
Classification Hematogenous Spread seeding through the bloodstream
Childhood disease Vascular insufficiency skin infections in persons with vascular insufficiency. Contiguous Spread Spread of bacteria from adjacent tissue infection or by direct inoculation

16
Hematogenous Osteomyelitis
Hematogenous osteomyelitis originates with infectious organisms that reach the bone through the bloodstream. Acute hematogenous osteomyelitis occurs predominantly in children. In adults in debilitated persons those with a history of chronic skin infections, chronic urinary tract infections intravenous drug use Immunocomprimised patients Intravenous drug users are at risk for infections with Streptococcus and Pseudomonas

17
Pathogenesis. In children
In children, the infection usually affects the long bones of the appendicular skeleton. In children 1 year of age and younger, the adjacent joint is often involved because the periosteum is not firmly attached to the cortex. From 1 year of age to puberty, subperiosteal abscesses are more common

18
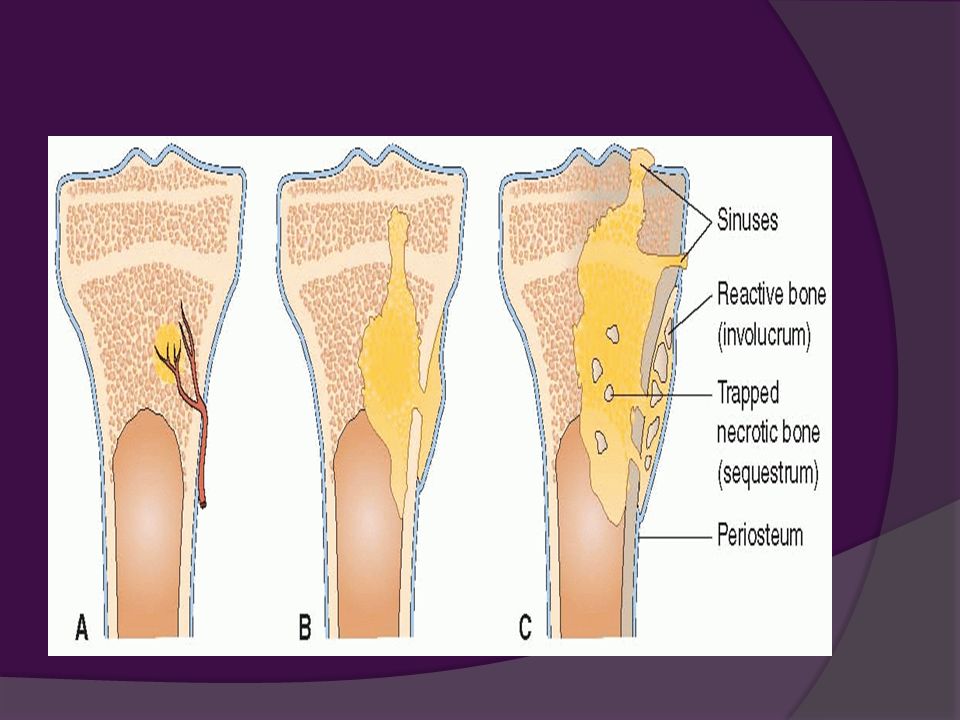
Pathophysiology Infectious organisms reach the metaphysis through a nutrient blood vessel. Bacterial growth results in bone destruction and abscess formation. From the abscess cavity, the infection spreads between the trabeculae into the medullary cavity of compact bone and then through the cortex to the outside. The purulent exudate finds its way beneath the periosteum, due to the rigid structure of the bone shearing off the perforating arteries that supply the cortex with blood, thereby leading to necrosis of cortical bone and formation of devascularized fragments, called sequestra. Eventually, the purulent drainage may penetrate the periosteum and skin to form a draining sinus.

20
Pathopysiology sequestrum involucrum
necrotic bone, often denser than surroundings may be resorbed, discharged thru a sinus tract, or persist as a focus of continued infection involucrum bone formed beneath elevated periosteum surrounds sequestrum

21
Manifestations. The signs and symptoms of acute hematogenous osteomyelitis are those of bacteremia accompanied by symptoms referable to the site of the bone lesion. Bacteremia is characterized by chills, fever, and malaise. There often is pain on movement of the affected extremity loss of movement, and local tenderness followed by redness and swelling

22
Treatment. The treatment of hematogenous osteomyelitis begins with identification of the causative organism through blood and bone aspiration cultures. Antimicrobial agents are given first parenterally and then orally. The length of time the affected limb needs to be rested and pain control measures used is based on the person's symptoms. Debridement and surgical drainage also may be necessary.

23
Direct Penetration and Contiguous Spread Osteomyelitis
Direct penetration or extension of bacteria from an outside (exogenous) source is now the most common cause of osteomyelitis in the United States. Bacteria may be introduced directly into the bone by a penetrating wound an open fracture surgery.
 source is now the most common cause of osteomyelitis in the United States. Bacteria may be introduced directly into the bone. by a penetrating wound. an open fracture. surgery.")
24
Risk factors The following increase the bone's susceptibility to infection. Inadequate irrigation or debridement introduction of foreign material into the wound extensive tissue injury

25
Microorganisms Staphylococci and streptococci are still commonly implicated, but in 25% of postoperative infections, gram-negative organisms are detected.

26
Measures to prevent these infections
preparation of the skin to reduce bacterial growth before surgery or insertion of traction devices or wires; strict operating room protocols; prophylactic use of antibiotics immediately before and for 24 hours after surgery and as a topical wound irrigation; maintenance of sterile technique after surgery when working with drainage tubes and dressing changes.

27
Manifestations. Osteomyelitis after trauma or bone surgery usually is associated with persistent or recurrent fever, increased pain at the operative or trauma site, poor incisional healing, which often is accompanied by continued wound drainage and wound separation. Prosthetic joint infections often present with joint pain, fever, and cutaneous drainage.

28
Osteomyelitis With Vascular Insufficiency
In persons with vascular insufficiency, osteomyelitis may develop from a skin lesion. It is most commonly associated with chronic or ischemic foot ulcers in persons with long-standing diabetes. Neuropathy causes a loss of protective reflexes, and impaired arterial circulation and repetitive trauma are the major contributors to skin fissure and ulcer formation.

29
Microorganism S. aureus coagulase-negative staphylococci Gram-negative
anaerobic organisms usually mixed infection

30
Manifestations Persons with vascular insufficiency osteomyelitis often present with seemingly unrelated problems such as ingrown toenails cellulitis, a perforating foot ulcer making diagnosis difficult. pain is often muted by peripheral neuropathy. Osteomyelitis is confirmed when bone is exposed in the ulcer bed or after debridement. Radiologic evidence is a late sign.

31
Treatment Treatment depends on the oxygen tension of the involved tissues. Debridement and antibiotic therapy may benefit persons who have good oxygen tension in the infected site. Hyperbaric oxygen therapy may be used as an adjunctive treatment. Amputation may be indicated when oxygen tension is inadequate.

32
Chronic Osteomyelitis
Chronic osteomyelitis usually occurs in adults. Generally, these infections occur secondary to an open wound, most often to the bone or surrounding tissue. it is a long-standing infection that evolves over months or even years, characterised by the persistence of microorganisms, low-grade inflammation, and the presence of dead bone (sequestrum)
")
33
Chronic osteomyelitis
It may be the result of delayed or inadequate treatment of acute hematogenous osteomyelitis or osteomyelitis caused by direct contamination of bone by exogenous organisms. Relapses in the same area and with accompanying fever are a clear sign of chronic osteomyelitis. Clinical signs persisting for longer than 10 days are associated with the development of necrotic bone and chronic osteomyelitis.

34
Chronic osteomyelitis
The hallmark feature of chronic osteomyelitis is the presence of infected dead bone, a sequestrum, that has separated from the living bone. A sheath of new bone, called the involucrum, forms around the dead bone.

36
Diagnostic test for chronic osteomyelitis
Radiologic techniques such as x-ray films, bone scans, and sinograms are used to identify the infected site. Chronic osteomyelitis or infection around a total joint prosthesis can be difficult to diagnose because the classic signs of infection are not apparent and the blood leukocyte count may not be elevated. A subclinical infection may exist for years. Bone scans are used with bone biopsy for a definitive diagnosis.

37
Diagnosis Laboratory tests Diagnostic tests WBC ESR C-Reactive Protein
Bone biopsy Diagnostic tests Radiographs findings of chronic osteomyelitis Magnetic resonance imaging (MRI) is the best modality Computed tomography (CT) Nuclear imaging
 is the best modality. Computed tomography (CT) Nuclear imaging.")
38
General treatment consideration
Antibiotics used should have good penetration to the bone. High doses should be used Parental therapy in the first two weeks then depending on patient condition change it to oral. Duration of therapy Acute osteomylitis 4-6 wks Chronic osteomylitis 6-8 wks of parentral therapy 3-12 months of oral therapy

39
Characteristic of osteomyelitis
Vascular insufficiency Contiguous Spread Hematogenous spread Infection results from insufficient blood supply to fight the bacteria Spread of bacteria from adjacent tissue infection or by direct inoculation Spread of bacteria through the blood stream from a distant site Definition Adults >50 Feet Adults from yrs Femur, tibia, Skull Children< 16 yrs and >50 yrs Femur, tibia, humerus ,vertebrae Patient Population DM Pulmonary Vasculary disease Post CABG (Sternum) Open reduction of fractures Gun shot wound Dental/Sinus infections Soft tissue infections Bacteriemia Sickle cell anemia Predisposing factors Pain, swelling, drainage, ulcer formation Fever, warmth, swelling unstable joint Fever, chills, local tenderness, swelling; limitation of motion Clinical findings Usually polymicrobial S.Aureus S.Epidermidis Streptococcus Gram –ve bacilli Anerobic Bacteroides fragilis gp Infected prosthesis Usually mixed Infection Usually monomicrobial Children S.Aureus,S.Epidermidis ,S.Pyogenes H.Influenzae ,P.auerginosa ,Enterobacter, Ecoli Adults salmonella ,S.pneumoniae Common pathogens
 Open reduction of fractures. Gun shot wound. Dental/Sinus infections. Soft tissue infections. Bacteriemia. Sickle cell anemia. Predisposing factors. Pain, swelling, drainage, ulcer formation. Fever, warmth, swelling unstable joint. Fever, chills, local tenderness, swelling; limitation of motion. Clinical findings. Usually polymicrobial. S.Aureus. S.Epidermidis. Streptococcus. Gram –ve bacilli. Anerobic. Bacteroides fragilis gp. Infected prosthesis. Usually mixed Infection. Usually monomicrobial. Children. S.Aureus,S.Epidermidis ,S.Pyogenes. H.Influenzae ,P.auerginosa ,Enterobacter, Ecoli. Adults. salmonella ,S.pneumoniae. Common pathogens.")
Similar presentations







 FRACTURES. An open fracture can be defined as a broken bone that is in communication through the skin with the environment.>")








. >")




