Download presentation
Presentation is loading. Please wait.

1
Laparoscopic Recognition of Endometriosis D an C. Martin, M.D. University of Tennessee Health Science Center Memphis, Tennessee ---------------------- IX Congreso Nacional de Endoscopia Ginecológica July 4 to 7, 2007 Puerto Vallarta, Jalisco, Mexico, California

2
Diagnosis of Endometriosis These may be clinical or research. History –Is “pain” adequate? Physical Examination –Is “focal tenderness” adequate? Laboratory (Immunology) Radiology (Sonography, MRI) Laparoscopy Laparotomy Histology* –* Please see the $100 reward information.
 Radiology (Sonography, MRI) Laparoscopy Laparotomy Histology* –* Please see the $100 reward information..")
3
Blind Spots Clarification of purposes –Research –Clinical Decisions on endometriosis therapy are based on several definitions that are not always related. –We do not know if this is reasonable. –It implies we can ignore or discount patients who have a laparoscopic diagnosis but are histologically negative. There is a large body of literature on accuracy of confirmation of endometriosis but not a corresponding literature on histologic diagnosis of peritoneal and pelvic abnormalities. –Psammoma bodies, endosalpingiosis, Walthard Rests, low malignant potential tumor and other pathology have been identified as endometriosis. –If we think it is endometriosis then other significant pathology may not be detected if we fail to do biopsies.

4
Confirmation at a Research Level Year 19821983198419851986.11986.2 Cumulative Number 97188279376426495 of Patients by One Gyn Positive for Endo 62%50%91%93%96%99% when Excised NOTE: My 99% was in the last 69 of 495 cases over 60 months (8.2 per month) Martin 1987, Stripling 1988, Martin 1990 45% Positive Predictive Value in 44 cases over 20 months (2.2.per month) Walter, 2001 61% of lesions in first 46 cases over 34 months (1.4 per month) 68% of lesions in next 56 cases over 36 months (1.6 per month) Stratton 2003, Stegmann 2005, the NIH group 88% in Webb’s study in 72 cases over 7 months (10.1 cases per month) Webb presented at AAGL 2006 and a paper is in preparation.
 Martin 1987, Stripling 1988, Martin % Positive Predictive Value in 44 cases over 20 months (2.2.per month) Walter, % of lesions in first 46 cases over 34 months (1.4 per month) 68% of lesions in next 56 cases over 36 months (1.6 per month) Stratton 2003, Stegmann 2005, the NIH group 88% in Webb’s study in 72 cases over 7 months (10.1 cases per month) Webb presented at AAGL 2006 and a paper is in preparation.")
5
Research Confirmation Protocol Anticipation of a high histologic clinical confirmation rates requires attention to many of the steps used in a research protocol. The research protocol is more demanding than clinical protocols. Data is needed before we conclude that research protocol need to be applied clinically.

6
Research Confirmation Protocol No Expectation of Appearance Biopsy Techniques Adequate Number of Biopsies Signal to Noise Ratio Tagging the Specimen Location Marking the Specimen Side Notations on Pathology Request Uniform Specimen Size in Container Cell Block Transferring the Specimen to Container Processing by the Surgeon Communications with the Cutters Communications with the Pathologist Re-cutting Specimens Requiring Histologic Description Histologic Criteria (Batt 1989) Reviewing Slides Surgeon Experience Fixed Protocol with Blinding
 Reviewing Slides Surgeon Experience Fixed Protocol with Blinding")
7
What Can We Do with a Biopsy? Rule Out Cancer Determine a Histologic Diagnosis Research This does not include deciding on therapy of endometriosis. –Therapeutic conclusions in the literature are based on appearance or history but not histology. –The literature says to treat it like endometriosis if it looks like endometriosis. –Histology is used to clarify other concerns. –See $100 reward information.

8
Clinical Purpose of Biopsy Rule out cancer Establish diagnosis in confusing cases May guide further evaluation or therapy

9
Research Purpose of Biopsy Add to science Establish histologic diagnosis in all cases Develop conclusions Develop additional research

10
Limitations of Biopsy Biopsy results do not commonly help with decisions on therapy.* –* Please see the $100 reward information. A negative biopsy does not exclude endometriosis or other pathology. Biopsies can create complications.

11
Who Needs a Biopsy? Dark Scarred Puckered Pigmented Mixed Color - > No biopsy needed. Dark Scarred Puckered Pigmented and Vesicles. - > Biopsy! Asymptomatic patient having tubal sterilization. (Moen)
.")
12
Who Needs a Biopsy? Endometriosis Endosalpingiosis Psammoma Bodies - > Biopsy needed? Same plus LMPT and Cancer - > Biopsy! Asymptomatic patient having tubal sterilization. (Moen)
.")
13
Who Needs a Biopsy? Psammoma Bodies Endosalpingiosis - > Biopsy needed? Same plus LMPT and Cancer - > Biopsy! Asymptomatic patient having tubal sterilization. (Moen)
.")
14
Who Needs a Biopsy? Clear and Opaque Tubal Nodules - > Biopsy needed? Asymptomatic patient having tubal sterilization. (Moen)
.")
15
Who Needs a Biopsy? Clear and Opaque Tubal Nodules - > Biopsy needed? Walthard Rest - > Biopsy? What if infertility patient? - > No! Asymptomatic patient having tubal sterilization. (Moen)
.")
16
Other Pathology

17
Hemangiomatosis

18
Psammoma Bodies Endosalpingiosis Low Malignant Potential Tumor Cancer Other Pathology

19
Psammoma Bodies Endosalpingiosis Low Malignant Potential Tumor Cancer

20
Other Pathology Metastatic breast cancer

21
Other Pathology Metastatic breast cancer

22
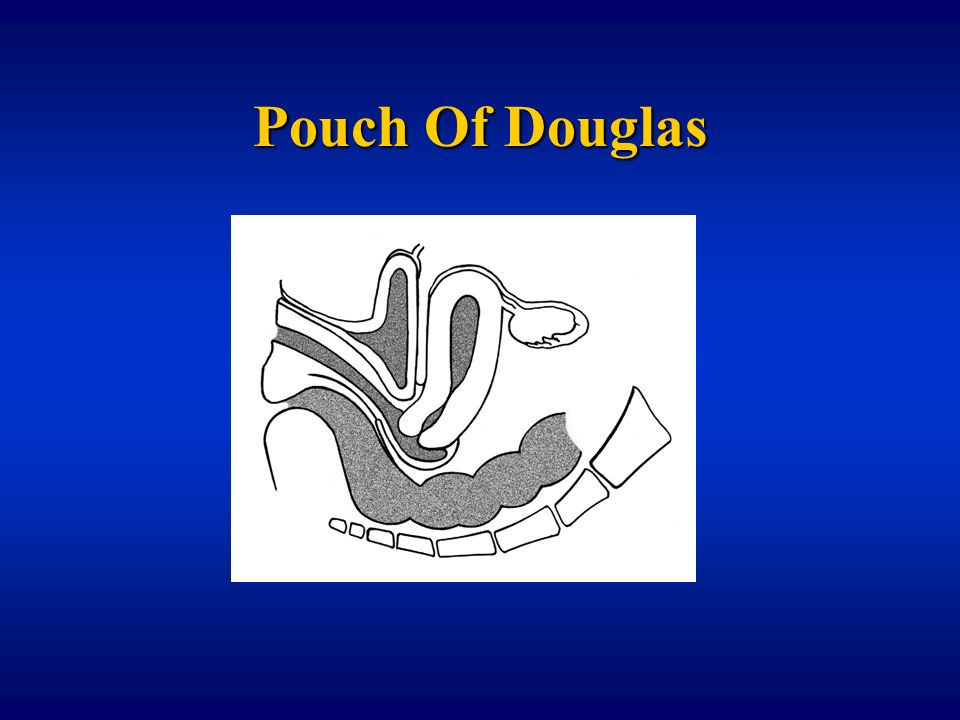
Pouch Of Douglas O

24
Vagina is generally in the upper half of the Pouch of Douglas. Bowel is generally in the lower half of the Pouch of Douglas.

25
Ring Forceps Test Harry Reich

26
Ring Forceps Test Harry Reich

27
Ring Forceps Test Harry Reich

28
Ring Forceps Harry Reich Endometriosis with Forceps in Vagina Rectum

29
Conclusions

30
Purpose of Biopsy Clinical Care –Laparoscopy is the gold standard –Exceptions Vaginal Endometriosis Sciatic, pulmonary, etc. endometriosis Research –Laparoscopy has been the gold standard –Histology is needed

31
Biopsy White nodules Clusters of vesicles Mixed color endometriosis. Anything you do not recognize.

32
Bowel Rectovaginal endometriosis is often retrocervical. These may not involve the bowel. Ring forceps test

33
Web Updates IX Congresso National de Endoscopia Ginecológica http://danmartinmd.com/cneg2007.htm Reward Information http://www.memfert.com/reward.htm

Similar presentations










 ”.>")








