Download presentation
Presentation is loading. Please wait.

1
Chemotherapy Review Daniel A. Nikcevich, MD, PhD Duluth Clinic Cancer Center March 31, 2009

2
Chemotherapy Review What should we talk about in 1 hour? Ad nauseum review of drugs? Real patient stories?

3
Chemotherapy Review Who is this patient? Stage of disease –Molecular profile –Genetic profile –Immunophenotype What are the goals of therapy? –Curative –Palliative When to start/stop therapy Follow-up –Role of the primary-care physician

4
Chemotherapy Review Who is this patient? Performance status Comorbidities –Ability to tolerate side-effects Social/cultural/religious issues The patient’s wishes and desires

5
Mackler NJ and Pienta KJ (2005) Drug Insight: use of docetaxel in prostate and urothelial cancers. Nat Clin Pract Urol 2: 92–100 doi:10.1038/ncpuro0099 Table 2 Eastern Cooperative Oncology Group (ECOG) performance status
 performance status.")
6
Mackler NJ and Pienta KJ (2005) Drug Insight: use of docetaxel in prostate and urothelial cancers. Nat Clin Pract Urol 2: 92–100 doi:10.1038/ncpuro0099 Table 3 Karnofsky performance status

7
Chemotherapy Review Breast cancer Colon cancer Chronic lymphocytic leukemia

8
Chemotherapy Review 60 yo female in excellent health presents to your office with a left breast mass. Mammogram shows 2 cm spiculated lesion in UOQ. What’s the next step? Biopsy Grade 1 infiltrating ductal carcinoma She’s now s/p lumpectomy and sentinel lymph-node biopsy

9
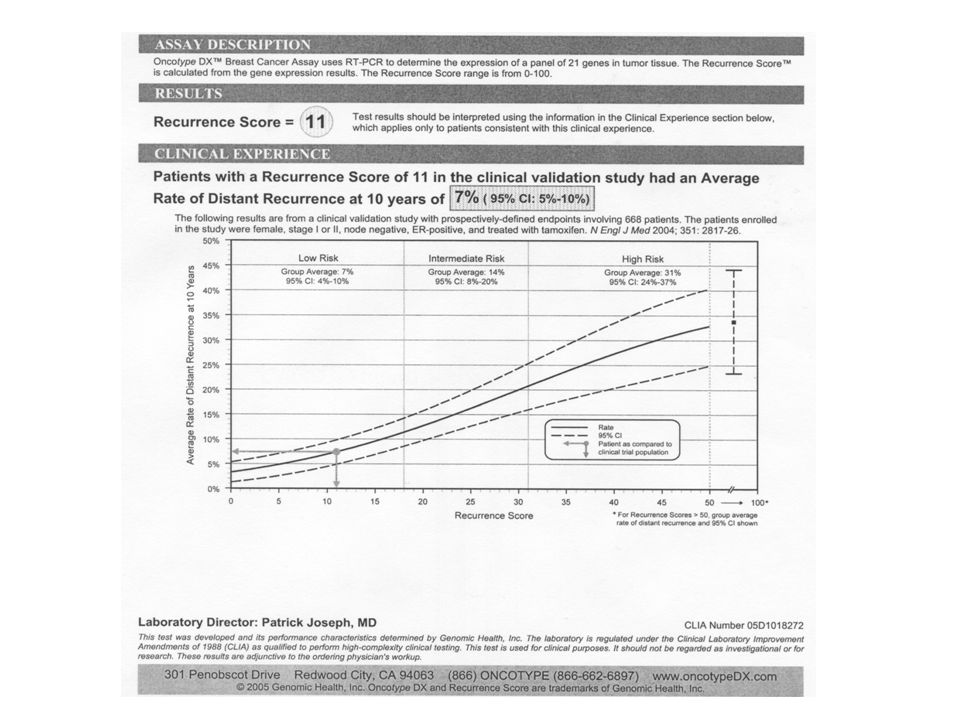
Chemotherapy Review Stage 1 (T1N0M0) infiltrating ductal carcinoma. ER + /PR +, her-2-neu negative, grade 1. How should she be treated? Hormonal/endocrine therapy –Tamoxifen –Aromatase inhibitor Chemotherapy –Doxorubicin/cyclophosphamide –Cyclophosphamide/methotrexate/flurouracil –Cyclophosphamide/docetaxel

12
Chemotherapy Review 5 years of adjuvant hormonal therapy = risk of recurrence of approximately 7% in 10 years. 5 years of adjuvant hormonal therapy plus chemotherapy = risk of recurrence of approximately 6% in 10 years. Absolute benefit of chemotherapy ~ 1% So how should your patient be treated? Hormonal therapy –Tamoxifen –Aromatase inhibitor –Consider bisphosphonate (zoledronic acid)
.")
13
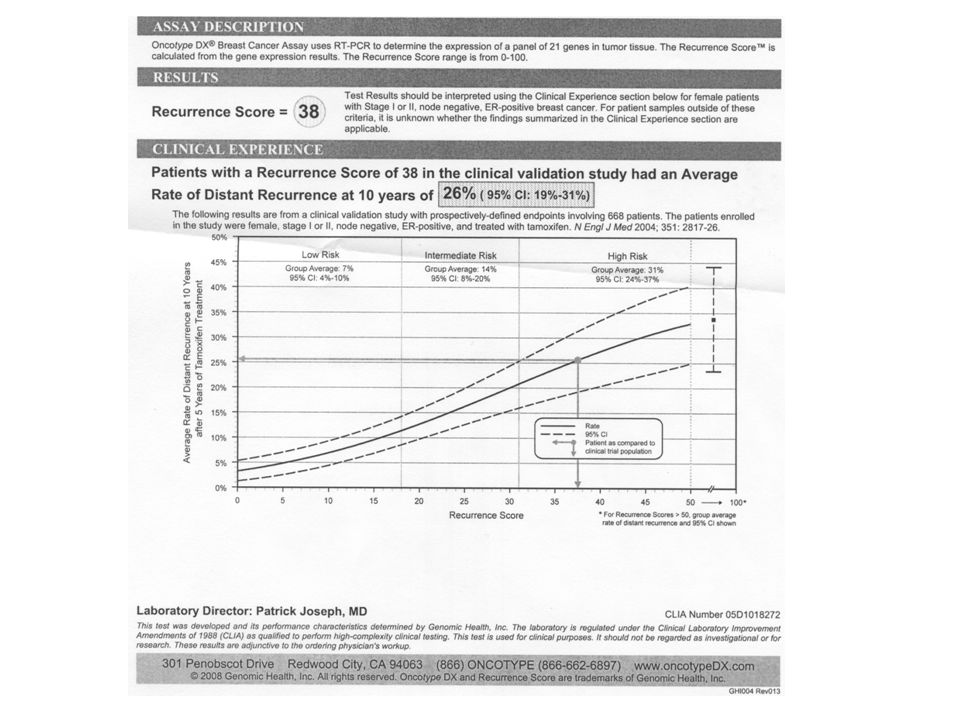
Chemotherapy Review 38 yo female with a strong family history of breast cancer presents with mastalgia that developed shortly after the birth of her daughter. The breast exam is unremarkable and the mammogram reveals a vague density in the right breast which cannot be identified on ultrasound. What is the next step? MRI 3 cm mass in the central breast with enlarged right axillary lymph nodes. Grade 3 infiltrating lobular carcinoma

14
Chemotherapy Review Your patient undergoes a right modified radical mastectomy and axillary lymph node dissection. Stage IIIA (T2N1M0) infiltrating lobular carcinoma. –ER + /PR - and her-2-neu 3+ (positive) How should she be treated?
 infiltrating lobular carcinoma. –ER + /PR - and her-2-neu 3+ (positive) How should she be treated .")
15
Chemotherapy Review Hormonal/endocrine therapy –Tamoxifen –Aromatase inhibitor Chemotherapy –Doxorubicin/cyclophosphamide/paclitaxel –Cyclophosphamide/methotrexate/fluorouracil –Cyclophosphamide/docetaxel Trastuzumab

16
Chemotherapy Review Estimate of recurrence in 10 years with no therapy = 70% Estimate recurrence with tamoxifen = 40% Estimate recurrence with tamoxifen plus chemotherapy = 30% Estimate recurrence with tamoxifen, chemotherapy, and trastuzumab = 15% What therapy would you recommend for your patient?

17
Chemotherapy Review She enrolled into a clinical trial and received chemotherapy with doxorubicin, cyclophosphamide, and paclitaxel. Also received trastuzumab and lapatinib (an oral drug similar to trastuzumab). Now on tamoxifen and doing well 2 years out from her surgery.
. Now on tamoxifen and doing well 2 years out from her surgery..")
18
Chemotherapy Review 58 yo retired nurse comes to your clinic with a c/o persistent right shoulder pain. Plain films show a lytic lesion in proximal right humerus, and bone scan indicates other sites of suspected disease. Biopsy of right humerus shows moderately- differentiated adenocarcinoma –ER + /PR +, her-2-neu negative Mammogram shows 1 cm lesion in left breast –Biopsy shows similar findings to bone biopsy

19
Chemotherapy Review What is the stage of disease? Stage IV (T1NXM1) Metastatic breast cancer is incurable What are the goals of therapy? Palliation –Symptom relief –QOL Prolong survival
 Metastatic breast cancer is incurable What are the goals of therapy. Palliation –Symptom relief –QOL Prolong survival.")
20
Chemotherapy Review How should your patient be treated? Hormonal/endocrine therapy –Tamoxifen –Aromatase inhibitor –Fulvestrant Chemotherapy –Doxorubicin/cyclophosphamide –Cyclophosphamide/methotrexate/fluorouracil –Epirubicin –Paclitaxel –nab-paclitaxel –Docetaxel –Carboplatin –Gemcitabine –Vinorelbine –Capecitabine –Ibexapilone –Bevacizumab –Trastuzumab

21
Chemotherapy Review Bone-only breast cancer is often an indolent disease. Does she have a clinical trial option? This patient has been treated on study with anatrozole, an aromatase-inhibitor. She is pain-free and with excellent QOL, four years from diagnosis. I use chemotherapy for metastatic breast cancer in setting of visceral crisis and/or rapidly progressive disease.

22
Chemotherapy Review Breast cancer Colon cancer Chronic lymphocytic leukemia

23
Chemotherapy Review 60 yo male who is in good health presents for a screening colonoscopy. He is found to have a mass at 30 cm. Biopsy shows moderately differentiated adenocarcinoma. He goes to surgery for a sigmoid colectomy. Stage 3B (T3N1M0) colon cancer.
 colon cancer..")
24
Chemotherapy Review How should your patient be treated? Chemotherapy is standard of care for stage 3 colon cancer. Chemotherapy options –5-FU/leucovorin –5-FU/leucovorin/oxaliplatin (FOLFOX) –Clinical trial Estimate of recurrence within 5 years if no chemotherapy = 60%. Estimate of reurrence within 5 years with FOLFOX = 30%.
 –Clinical trial Estimate of recurrence within 5 years if no chemotherapy = 60%. Estimate of reurrence within 5 years with FOLFOX = 30%..")
25
Chemotherapy Review How should your patient be treated? He opted for participation in a clinical trial –NCCTG trial N0147 (FOLFOX +/- cetuximab) –He is KRAS wild-type –Only KRAS wild-type predict response to EGFR inhibitors He completed chemotherapy (FOLFOX), but incurred a persistent, mild peripheral neuropathy. Disease-free 4 years from diagnosis.
 –He is KRAS wild-type –Only KRAS wild-type predict response to EGFR inhibitors He completed chemotherapy (FOLFOX), but incurred a persistent, mild peripheral neuropathy. Disease-free 4 years from diagnosis..")
26
Chemotherapy Review 64 yo retired nurse in excellent health presents to your office with a c/o of constipation. Fecal occult blood test is positive. Colonoscopy shows 2 cm cecal mass; a well-differentiated adenocarcinoma. She has a right hemicolectomy. Stage 2 (T3N0M0) colon cancer.
 colon cancer..")
27
Chemotherapy Review How should your patient with stage 2 colon cancer be treated? Does he need chemotherapy? –5-FU/leucovorin –5-FU/leucovorin/oxaliplatin (FOLFOX) –Chemotherapy not necessarily standard of care for stage 2 disease –Clinical trial Can we distinguish between “high-risk” and “low- risk” stage 2 colon cancer?
 –Chemotherapy not necessarily standard of care for stage 2 disease –Clinical trial Can we distinguish between high-risk and low- risk stage 2 colon cancer .")
28
Chemotherapy Review Average risk of recurrence at 5 years for stage 2 colon cancer = 15% (w/o chemo) Range of risk recurrence = <10% - 40%. Patients with tumors that exhibit 18q LOH and MSI with much higher risk. –Subject of current clinical trial (ECOG 5202) This patient enrolled into the study. Has low-risk disease (<10% recurrence). Did not receive chemotherapy and is followed with observation alone.
 This patient enrolled into the study. Has low-risk disease (<10% recurrence). Did not receive chemotherapy and is followed with observation alone..")
29
Chemotherapy Review 78 yo male presents to the ER with increasing abdominal pain. He is found to have a bowel obstruction. Surgical exploration reveals large cecal mass with multiple liver metastases. Stage 4 (T3N2M1) colon cancer.
 colon cancer..")
31
Chemotherapy Review How should your patient with stage 4 colon cancer be treated? Does he need chemotherapy? –Yes. –5-FU/leucovorin/oxaliplatin (FOLFOX) –FOLFOX plus bevacizumab –Capecitabine plus oxaliplatin (XELOX) –FOLFIRI –FOLFIRI plus cetuximab (k-ras wild-type predicts response to cetuximab) –Clinical trial
 –FOLFOX plus bevacizumab –Capecitabine plus oxaliplatin (XELOX) –FOLFIRI –FOLFIRI plus cetuximab (k-ras wild-type predicts response to cetuximab) –Clinical trial.")
32
Chemotherapy Review What are the goals of therapy? –Palliation –QOL –Prolong life –Cure? What are the patient’s goals? –QOL –Wishes to live at his retirement cabin and cut wood, fish, ski, and spoil his grandchildren.

33
Chemotherapy Review How should your patient with stage 4 colon cancer be treated? He received FOLFOX plus bevacizumab. –Standard of care for stage 4 colon cancer Responded well with reduction in liver metastases. Surgical excision of liver disease. Remains well 3 years from liver resection.

34
Chemotherapy Review Breast cancer Colon cancer Chronic lymphocytic leukemia

35
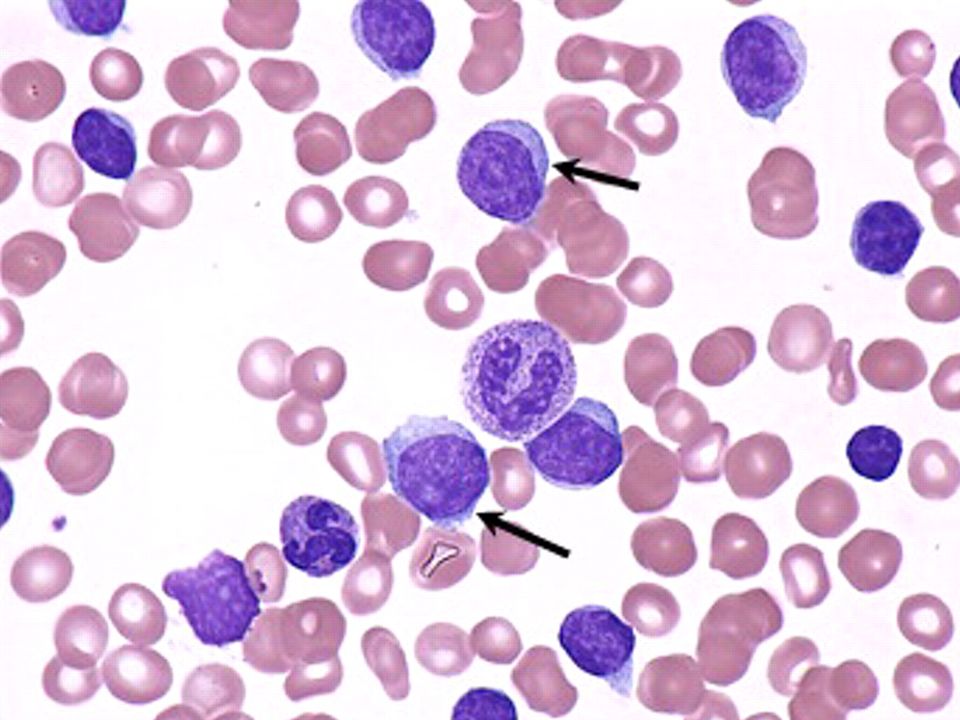
Chemotherapy Review 44 yo male in excellent health is noted to have WBC 40K (HgB and platelets normal) during routine life-insurance examination What is the first step? What is the second step? What is the third step? Look at the blood film.

37
Chemotherapy Review Flow cytometry confirms clinical suspicion of CLL (CD5 + CD19 + CD20 + CD23 + CD38 - ) FISH shows 13q- He is asymptomatic and has no lymphadenopathy or splenomegaly. He has Rai stage 0 disease with favorable prognostic features (CD38 - and 13q-)
.")
38
Chemotherapy Review How should this patient be treated? Does he need any treatment? What is the natural history of CLL? What is the significance of staging? What is the significance of the molecular markers documented at diagnosis?

39
Clinical Features of CLL Often an incidental diagnosis in an asymptomatic patient. Indolent disease common Progressive adenopathy often correlates with symptoms: fatigue, malaise, weight loss, fevers Progressive bone marrow involvement leads to severe cytopenias, increase risk infection Autoimmune sequelae and Richter’s transformation are long-term complications

40
Staging Rai system Rai 0: lymphocytosis Rai 1: lymphadenopathy Rai 2: splenomegaly Rai 3: HgB < 11 g/dL Rai 4: platelets < 100K Binet system A: lymphocytosis +/- 1-3 sites lymphadenopathy B: lymphocytosis with > 3 sites lymphadenopathy C: lymphocytosis + anemia and/or thrombocytosis

41
Why is staging important? Rai staging Rai 0: lymphocytosis Rai 1: lymphadenopathy Rai 2: splenomegaly Rai 3: HgB < 11 g/dL Rai 4: platelets < 100K Median survival > 10 years 7 years 2-5 years

42
Fig 1. Kaplan-Meier survival curve comparing CLL patients with mutated and unmutated VH genes. Median survival for unmutated CLL: 117 months; median survival for mutated CLL: 293 months. The difference is significant at the P =.001 level (log-rank test).
..")
43
Chemotherapy Review So how should this patient be treated? Corticosteroids Alkylating agents –Chlorambucil –Cyclophosphamide Nucleoside analogs –Fludarabine –Pentostatin Monoclonal antibodies –Rituximab (anti-CD20) –Alemtuzumab (anti-CD52) Combination chemotherapy –PCR –FCR Allogeneic stem cell transplantationcell
 –Alemtuzumab (anti-CD52) Combination chemotherapy –PCR –FCR Allogeneic stem cell transplantationcell.")
44
Chemotherapy Review Mutual decision reached to not treat, but to observe and monitor with serial exams and blood tests. 6 years later, he remains asymptomatic with WBC 44K, HgB 14 g/dL, and plts 150K.

45
Chemotherapy Review 57 yo accountant comes to your office at the insistence of his wife. He describes fatigue, night sweats, and a 10 lb weight loss. Exam shows multiple enlarged (2 cm) cervical and axillary lymph nodes. WBC 102K, HgB 10 g/dL, plts 95K What to do next?
 cervical and axillary lymph nodes. WBC 102K, HgB 10 g/dL, plts 95K What to do next .")
47
Chemotherapy Review Diagnosis of CLL established. Rai stage 4 (plts < 100K) CD38+ and FISH shows trisomy 12 A symptomatic patient with unfavorable molecular markers and immunophenotype How should this patient be treated?
 CD38+ and FISH shows trisomy 12 A symptomatic patient with unfavorable molecular markers and immunophenotype How should this patient be treated .")
48
Chemotherapy Review Corticosteroids Alkylating agents –Chlorambucil –Cyclophosphamide Nucleoside analogs –Fludarabine –Pentostatin Monoclonal antibodies –Rituximab (anti-CD20) –Alemtuzumab (anti-CD52) Combination chemotherapy –PCR –FCR Allogeneic stem cell transplantationcell
 –Alemtuzumab (anti-CD52) Combination chemotherapy –PCR –FCR Allogeneic stem cell transplantationcell")
49
Chemotherapy Review Clinical trial option? –Nothing available I treated him with PCR –Pentostatin, cyclophosphamide, rituximab –Well-tolerated, but leads to marked immunosuppression Entered into complete remission with resolution of trisomy 12

50
Chemotherapy Review Who is the patient? What is the disease? What are the treatment goals? –Of the patient? –Of the physician? What are the treatment options? What will the treatment do? What will the treatment not do?

51
Chemotherapy Review Questions? dnikcevich@smdc.org

Similar presentations

















>")

 DEFINITION CLL is a neoplastic disease characterized by proliferation and accumulation (blood, marrow and lymphoid.>")

