Download presentation
Presentation is loading. Please wait.

1
Chronic Lymphocytic Leukemia: Clinical Correlates and Issues Daniel A. Nikcevich, MD, PhD Duluth Clinic Cancer Center May 13, 2008

2
Chronic lymphocytic leukemia (CLL) –Diagnosis –Clinical features –Pathophysiology –Therapy
 –Diagnosis –Clinical features –Pathophysiology –Therapy")
3
Chronic lymphocytic leukemia Most common leukemia in adults Median age diagnosis 65 years Median survival 9 years Allogeneic stem cell transplant only curative therapy Decision to treat based on age, performance status, symptoms, disease stage

4
Pathophysiology CLL is an uncontrolled clonal accumulation of mature lymphocytes. Unclear mechanisms of initiation Molecular characterization of CLL correlates with clinical outcomes Mutated Ig V H genes Unmutated Ig V H genes

5
Diagnosis istory and physical examination CBC and peripheral blood film –Need absolute lymphocytosis > 5000/ml Flow cytometry Cytogenetics (FISH) CT C/A/P (as indicated) Bone marrow biopsy (as indicated)
 CT C/A/P (as indicated) Bone marrow biopsy (as indicated)")
6
Diagnosis Flow cytometry: –CD5 + CD19 + CD20 + CD23 + DDx: follicular lymphoma or mantle cell lymphoma with leukemic phase, prolymphocytic leukemia, SLVL, HCL Mantle cell lymphoma is a nasty, aggressive NHL –CD5 + CD23 - cyclinD1 + What’s the difference between CLL and SLL (small lymphocytic lymphoma)? –the tissue phase of CLL.

7
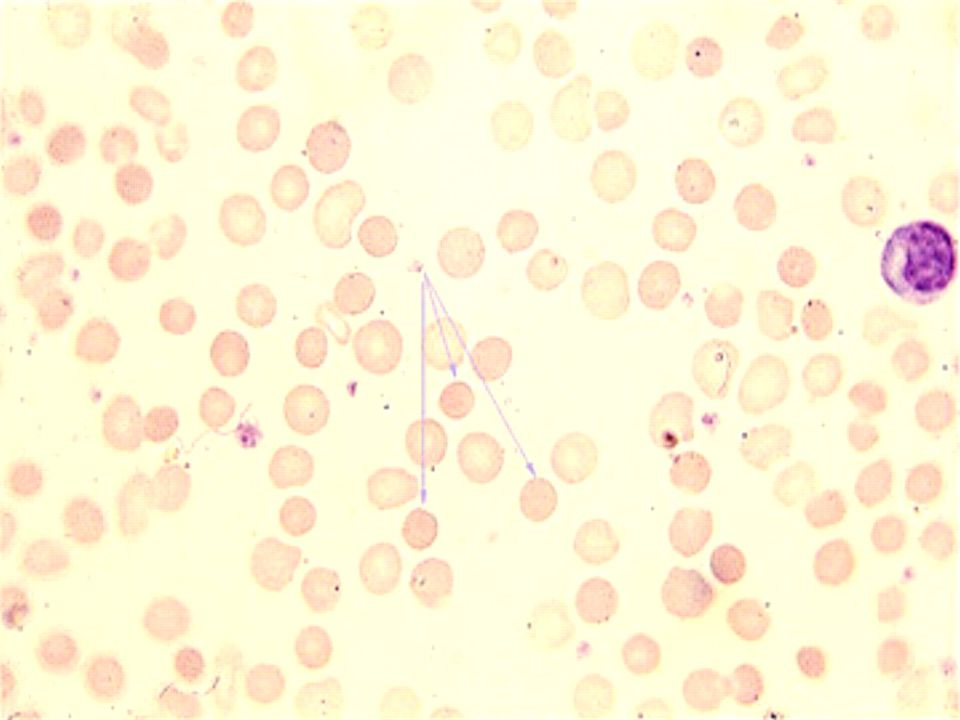
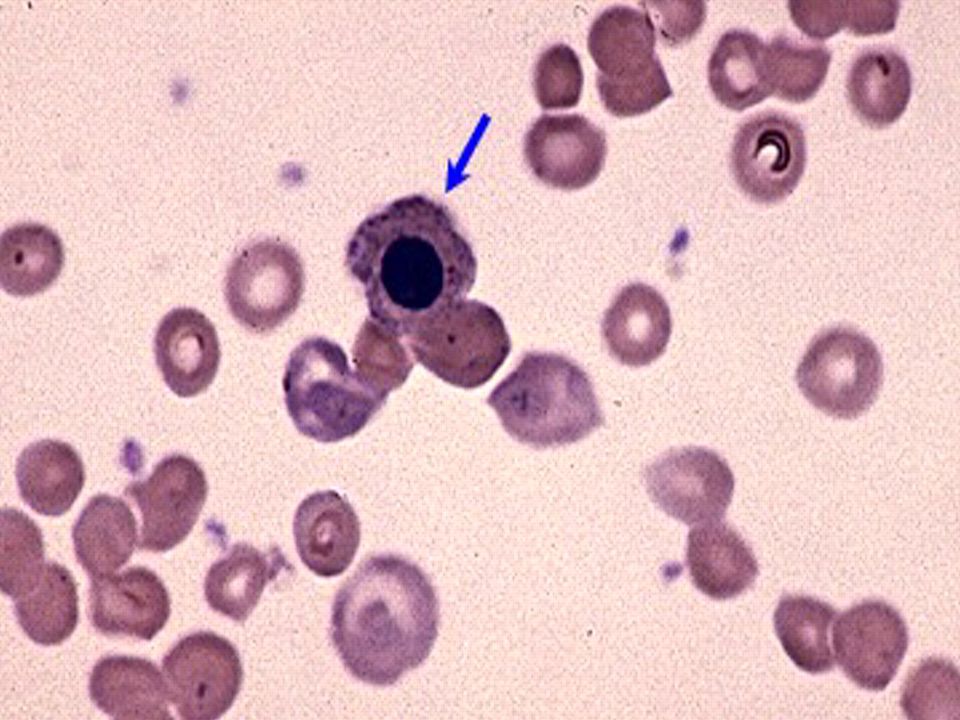
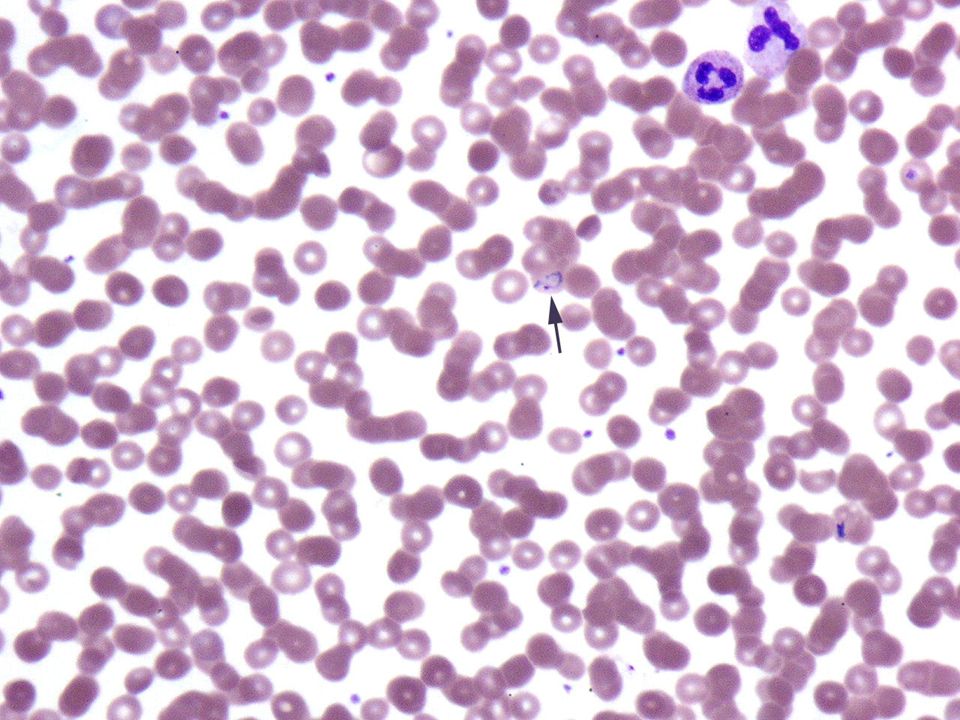
Copyright ©2003 American Society of Hematology. Copyright restrictions may apply. Maslak, P. ASH Image Bank 2003;2003:100690 Figure 1. This peripheral smear shows that there can be heterogeneity in the appearance of the abnormal lymphocytes in CLL

8
Clinical Features of CLL Often an incidental diagnosis in an asymptomatic patient. Indolent disease common Progressive adenopathy often correlates with symptoms: fatigue, malaise, weight loss, fevers Progressive bone marrow involvement leads to severe cytopenias, increase risk infection Autoimmune sequelae and Richter’s transformation are long-term complications

9
Autoimmune Complications of CLL AIHA –Coombs’ positive Pure red cell aplasia ITP Neutropenia

10
Staging Rai system Rai 0: lymphocytosis Rai 1: lymphadenopathy Rai 2: splenomegaly Rai 3: HgB < 11 g/dL Rai 4: platelets < 100K Binet system A: lymphocytosis +/- 1-3 sites lymphadenopathy B: lymphocytosis with > 3 sites lymphadenopathy C: lymphocytosis + anemia and/or thrombocytosis

11
Why is staging important? Rai staging Rai 0: lymphocytosis Rai 1: lymphadenopathy Rai 2: splenomegaly Rai 3: HgB < 11 g/dL Rai 4: platelets < 100K Median survival > 10 years 7 years 2-5 years

12
Poor Prognostic Factors Advanced stage at diagnosis Rapid lymphocyte doubling time Diffuse marrow infiltration Advanced age/male gender CLL-PLL (secondary PLL) Abnormal karyotype Elevated 2 -microglobulin, soluble CD23 CD38 + or ZAP-70 +
 Abnormal karyotype Elevated 2 -microglobulin, soluble CD23 CD38 + or ZAP-70 +")
13
CLL-cytogenetic abnormalities 13q- Normal karyotype Trisomy 12 11q- 17p- ALWAYS get FISH studies with CLL

14
Fig 1. Kaplan-Meier survival curve comparing CLL patients with mutated and unmutated VH genes. CLL: 117 months; median survival for mutated CLL: 293 months. The difference is significant at the P =.001 level (log-rank test).
..")
15
What if our lab is unable to perform Ig gene mutation studies? CD38 may be a surrogate marker for Ig gene mutations. –Detect via flow cytometry (easily) –CD38 + = unmutated Ig genes = poorer prognosis –CD38 - = mutated Ig genes = better prognosis CD38 + : 9 year median survival CD38 - : >20 years median survival
 –CD38 + = unmutated Ig genes = poorer prognosis –CD38 - = mutated Ig genes = better prognosis CD38 + : 9 year median survival CD38 - : >20 years median survival.")
16
ZAP-70 expression Correlates with Ig V H gene mutations Correlates CD38 + expression ZAP-70 + = Poorer prognosis

17
Crespo, M. et. al. N Engl J Med 2003;348:1764-1775 Correlation of the Level of Expression of ZAP-70 and Immunoglobulin Heavy-Chain Variable- Region (IgVH) Mutational Status (Panel A) and IgVH Sequence Homology (Panel B)
 Mutational Status (Panel A) and IgVH Sequence Homology (Panel B).")
18
Therapy of CLL: When to Treat? Constitutional symptoms Progressive lymphocytosis Progressive lymphadenopathy Progressive splenomegaly Progressive bone marrow failure Autoimmune complications Richter’s transformation or secondary PLL Your patient is uncomfortable with observation

19
Therapeutic Options for CLL Corticosteroids Alkylating agents –Chlorambucil –Cyclophosphamide Nucleoside analogs –Fludarabine –Pentostatin Monoclonal antibodies –Rituximab (anti-CD20) –Alemtuzumab (anti-CD52) Combination chemotherapy –PCR –FCR Allogeneic stem cell transplantationcell transplantation
 –Alemtuzumab (anti-CD52) Combination chemotherapy –PCR –FCR Allogeneic stem cell transplantationcell transplantation")
20
What’s the best way to treat CLL? Indication to treat Prognostic factors (stage, CD38 expression, ZAP-70, etc.) Younger, good PS patients –Clinical trial –PCR or FCR –Best response rates and chance of molecular remission –CAMPATH for purine-analog resistant disease Older, more frail patients –Chlorambucil (+/- prednisone) Allogeneic transplant the only curative modality for CLL –Need matched-sib donor –Substantial morbidity/mortality –The price of curing CLL is GVHD. Is that acceptable?
 Younger, good PS patients –Clinical trial –PCR or FCR –Best response rates and chance of molecular remission –CAMPATH for purine-analog resistant disease Older, more frail patients –Chlorambucil (+/- prednisone) Allogeneic transplant the only curative modality for CLL –Need matched-sib donor –Substantial morbidity/mortality –The price of curing CLL is GVHD. Is that acceptable .")
21
Patient L.P. 60 yo female in excellent health Routine exam with new primary care physician. CBC –WBC 43K –HgB 14.0 g/dL –Plts 350K –Flow cytometry shows CLL, CD38- –FISH with 13q-

23
Now what? Observation

24
Patient H.S. 57 yo male previously in good health 3 months of fevers, night sweats What’s next? HISTORY Exam Speaks with hoarse voice Adenopathy in submandibular, submental, anterior cervical, supraclavicular, axillary regions. No splenomegaly

25
Any tests that you wish to order? CBC WBC 35K HgB 13.7 g/dL Plts 135K Flow cytometry shows CLL, CD38+ FISH trisomy 12

27
Thoughts? Symptomatic disease. Needs treatment. Clinical trial option? I treated him with PCR Entered into complete remission with resolution of trisomy 12

28
Patient W.E. 47 yo male with known h/o CLL Initial treatment with FCR and entered into complete remission for 3 years Relapse and then treatment with Campath with complete remission obtained. Feels well, asymptomatic Exam normal CBC –WBC 26K –HgB 11.3 g/dL –Plts 175K

29
What’s next?

31
Secondary prolymphocytic leukemia –Richter’s transformation –New 17p- Poor prognostic sign Demonstrated refractory disease with BM failure and severe cytopenias

32
Patient W.S. 65 yo female with known CLL Previous treatment with fludarabine and entered into CR PMHx CAD, COPD, DM, HTN Notes fatigue, DOE What’s next? HISTORY

33
Generalized fatigue. No PND or orthopnea. No cough. No F/C/NS. No change in medications. What’s next? Exam Pale, appears tired. Afebrile, 116/76, HR 102, RR 14 Neck veins flat, lungs CTA, RRR, no murmur, no S3, no HJR, no LE edema

34
Any tests? CBC –WBC 5.4 –Hgb 8.8 g/dL –Plts 274K

37
Diagnosis? Autoimmune hemolytic anemia Common auto-immune sequel of CLL Presence of AIHA does NOT necessarily correlate with disease activity Treated successfully with prednisone

38
Patient W.B. 52 yo male with known CLL Treated with PCR x 6 cycles. Obtains complete remission with absence of presenting 11q- Arrives to office w/o app’t with cc of fevers HISTORY Drenching sweats, fevers. Recent return to Duluth from travel to Australia, Africa, Europe

39
40 o C, 122/86, HR 116, RR 18 No adenopathy, no splenomegaly CBC –WBC 15K –HgB 12.9 g/dL –Plts 307K Normal chemistries What’s next?

41
Diagnosis?

42
questions? dnikcevich@smdc.org

Similar presentations













.>")



>")
 DEFINITION CLL is a neoplastic disease characterized by proliferation and accumulation (blood, marrow and lymphoid.>")



:>")