Download presentation
Presentation is loading. Please wait.

1
Nwalozie J.C. 17/03/2014

2
Question A 50 year old man presents with sudden-onset breathlessness & feeling of impending doom. Discuss 3 differential diagnoses & describe the management of Acute Left Ventricular Failure.

3
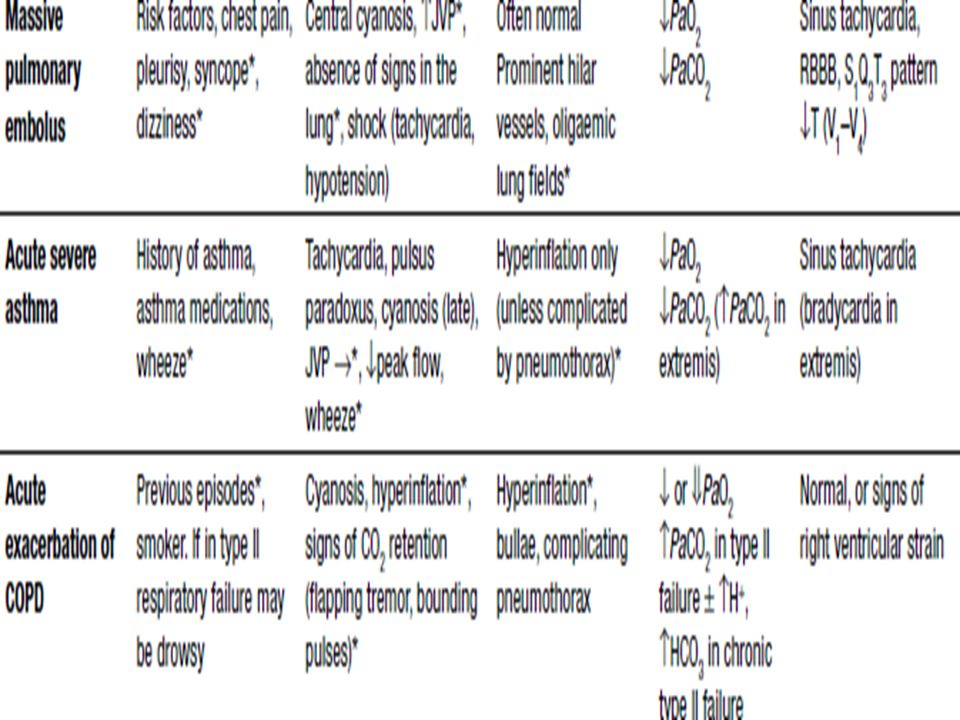
Answers 3 differential diagnoses: 1. Acute Severe asthma 2. Pulmonary Embolism 3.Acute exacerbation of COPD

7
MANAGEMENT OF ACUTE LEFT VENTRICULAR FAILURE

8
Outline Introduction Precipitating factors Pathophysiology Clinical features Investigations Management Treatment Prognosis & Monitoring Follow-up Conclusion

9
Introduction Inability of the left ventricle to effectively handle its pulmonary venous return with leakage of fluid from the pulmonary capillaries & venules into the alveolar space (secondary to increased hydrostatic pressure) leading to rapid onset of breathlessness. It is a medical emergency. It can arise de novo or on a background of chronic left ventricular failure.

10
PRECIPITATING FACTORS Dietary indiscretion Uncontrolled hypertension Non adherence to drugs Myocardial ischaemia or infarction Arrhythmias Thyrotoxicosis Fluid overload Anaemia Pulmonary & other infections Inappropriate medications- -ve inotropes, NSAIDS Acute valvular insufficiency

11
PATHOPHYSIOLOGY ↓ CARDIAC OUTPUT INCREASED PCWP ACTIVATION OF RENIN ANGIOTENSIN SYSTEM ACTIVATION OF S/S SYSTEM INCREASED HEART RATE INCREASED SYSTEMIC VASCULAR RESISTANCE INCREASED PRELOAD CARDIAC ISCHAEMIA ↓ LEFT VENTRICULAR FUNCTION SYMPTOMATIC DECOMPENSATION

12
CLINICAL FEATURES Extreme SOB with use of accessory muscles of respiration Sensation of drowning, chest pain, palpitations Cough(with pink, frothy sputum) Previous history: Of cardiac disease Restlessness, Profuse sweating
 Previous history: Of cardiac disease Restlessness, Profuse sweating")
13
CLINICAL FEATURES Orthopnoea(patient noticed to be sitting up in bed) - sensitivity 5% - specificity 77% PND Pulse(Tachycardia, Pulsus Alternans) BP S3 Wheezing (Cardiac ‘asthma’) – sensitivity 22% - specificity 58% Crepitations - sensitivity 6% - specificity 78%
 - sensitivity 5% - specificity 77% PND Pulse(Tachycardia, Pulsus Alternans) BP S3 Wheezing (Cardiac ‘asthma’) – sensitivity 22% - specificity 58% Crepitations - sensitivity 6% - specificity 78%")
14
Other features: -Cyanosis -Cold skin -Features of underlying heart disease/precipitating factor -Features of right heart failure

15
INVESTIGATIONS 1.Pulse oximetry 2. Blood 3. Electrocardiography 4. Radiologic 5.Others- eg. Pulmonary arterial catheterisation

16
BLOOD INVESTIGATIONS ABG FBC – anaemia, infection U & Es CARDIAC MARKERS

17
CARDIAC MARKERS CARDIAC ENZYMES OTHER CARDIAC MARKERS

18
IMPORTANCE OF BNP IN HF 1. Useful in Diagnosis 2. Assessing Severity 3. Predicting short & long-term CVS mortality

19
WHAT LEVELS ? NO HEART FAILURE -BNP < 100pg / dl -NT PRO-BNP < 300pg / dl HEART FAILURE -BNP >500pg / dl -NT PRO-BNP > 1000pg / dl *80% Sensitivity for heart failure

20
ELECTROCARDIOGRAM Ischaemia / infarction Arrhythmia – A fib LVH Prolonged QRS

21
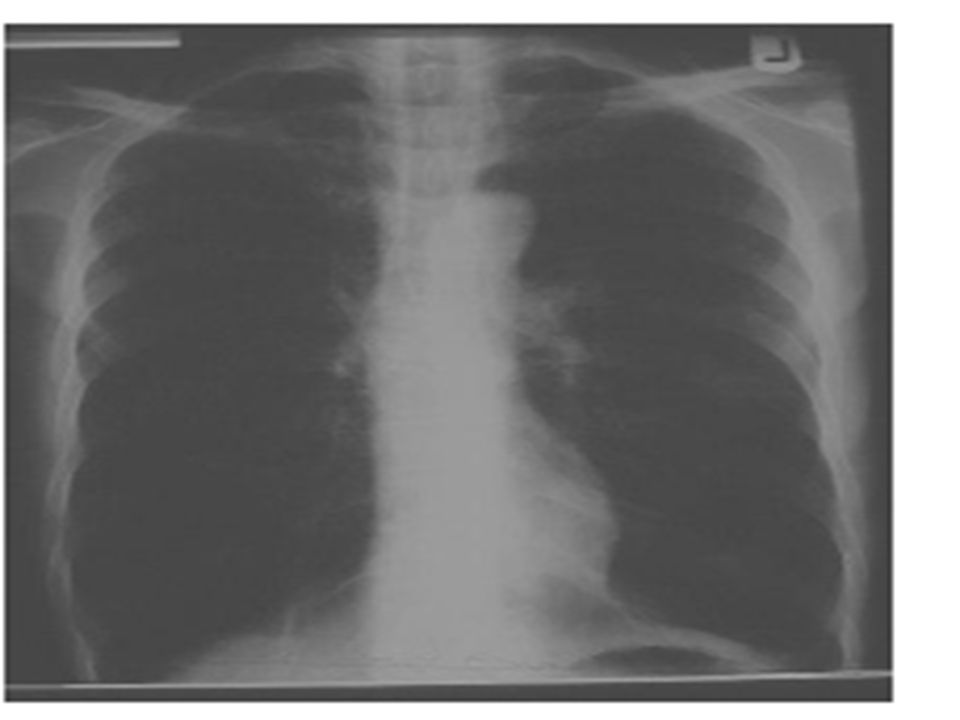
CHEST RADIOGRAPH FINDINGS IN HEART FAILURE Cardiomegaly – 74% sensitive, 78% specific Vascular redistribution Interstitial oedema Alveolar oedema Pleural effusions (right sided/bilateral)
")
23
Others Echocardiography 1.Identify reversible cause eg MI, valvular insufficiency,tamponade 2.Distinguish between systolic and diastolic dysfunction Monitor urine output

24
Treatment A medical emergency Begin treatment before investigations ABC of resuscitation, Patient to sit up Treatment can be medical, radiological/surgical

26
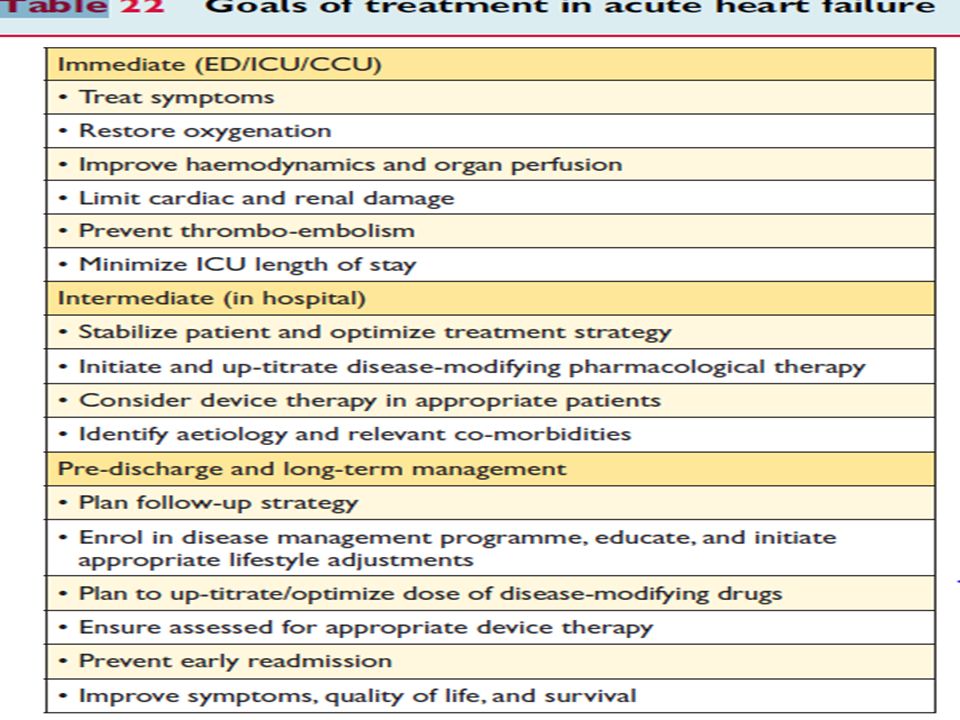
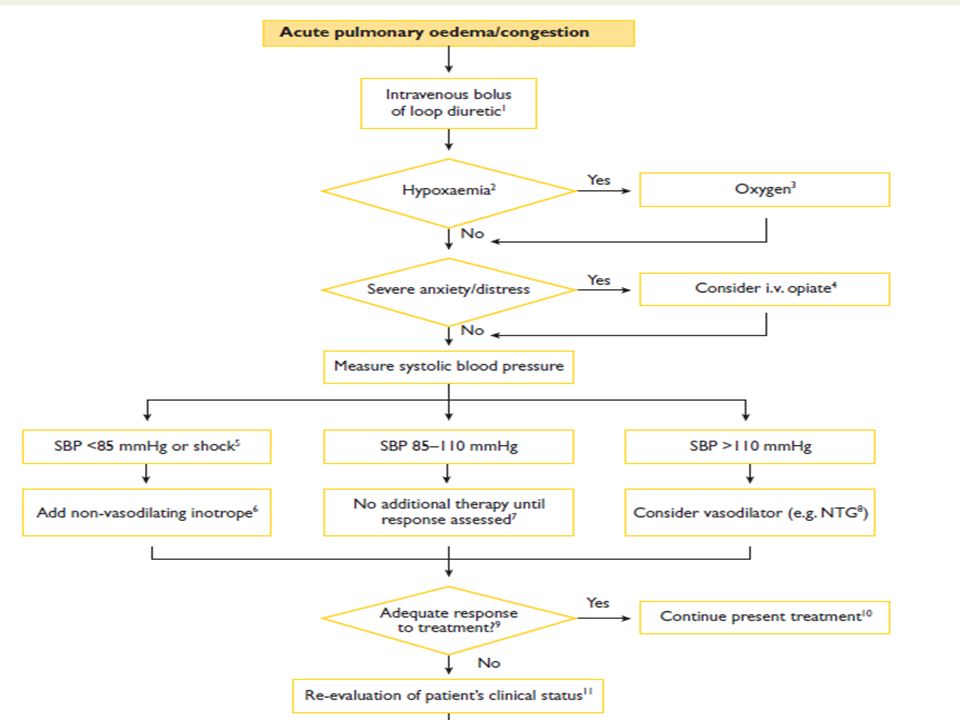
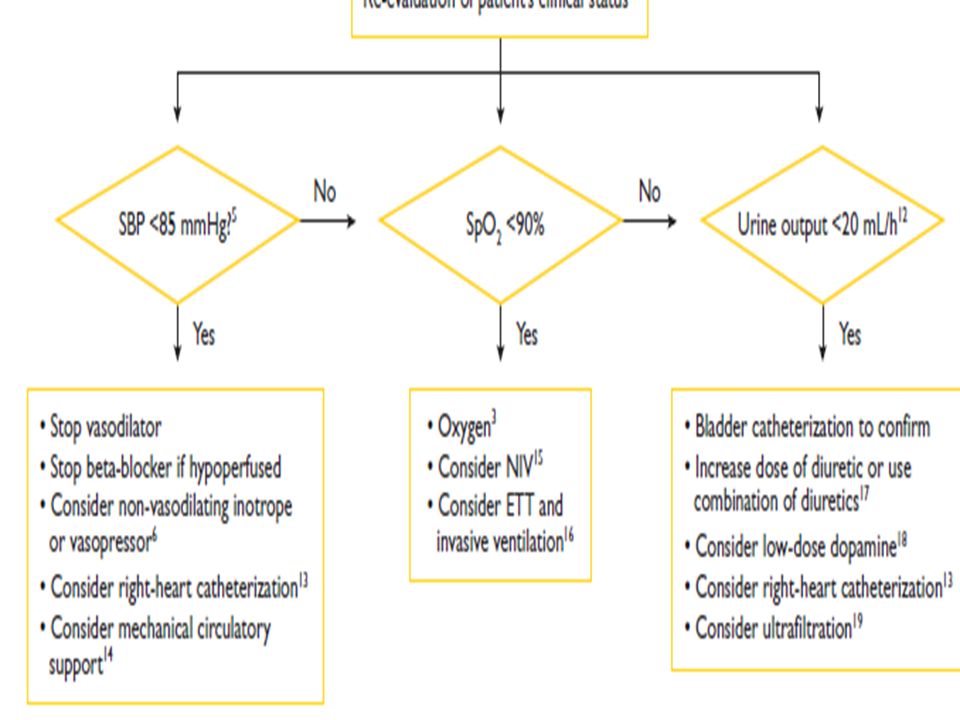
TREATMENT AIMS OF IMMEDIATE MANAGEMENT Overall aim- Redistribute fluid out of lungs! -Decrease Preload (right-sided filling) eg loop diuretics,morphine,tolvaptan -Increase left-sided emptying eg ACE- I,NTG,nitroprusside ↓ Afterload, Cardiac output -± improve LV contractility – inotropes eg dopamine,dobutamine,milrinone,levosimendan
 eg loop diuretics,morphine,tolvaptan -Increase left-sided emptying eg ACE- I,NTG,nitroprusside ↓ Afterload, Cardiac output -± improve LV contractility – inotropes eg dopamine,dobutamine,milrinone,levosimendan.")
29
Other measures-diet, fluid restriction, ultrafiltration, treat precipitating cause eg infection Radiological-IABP,LV assist device, CRT Surgical-Valve repairs, transplantation

30
Prognosis & monitoring Poor prognostic factors include: -Underlying heart disease/precipitating factor -BNP>500 pg/dl -K <3mmol/l -Na < 133mmol/l -Frequent ventricular extrasystoles Monitoring for vital signs, other signs, symptoms,urine output,renal function,electrolytes.

31
Follow Up

32
Conclusion ALVF is a life-threatening medical emergency that is as a result of LV compromise leading to accumulation of fluid in the lungs with resultant acute onset of symptoms. It is essential to make a diagnosis( ie differentiate it from similar conditions) so that necessary interventions can be instituted as soon as possible Management is multidisciplinary and should be individualised according to how each patient presents.
 so that necessary interventions can be instituted as soon as possible Management is multidisciplinary and should be individualised according to how each patient presents..")
33
THANK YOU FOR LISTENING !

Similar presentations









 Class IV: symptoms at rest Class III: symptoms on less-than-ordinary exertion Class.>")
 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")








) Dr. Walaa Nasr Lecturer of Adult Nursing Second year Second.>")

