Download presentation
Presentation is loading. Please wait.

1
DIABETES MELLITUS Rachel S. Natividad RN, MSN, NP

2
Review A&P Review A&P

3
Role of Insulin Insulin: – –Counters metabolic activity that would increase blood glucose levels – –Enhances transport of glucose into body cells – –Lowers blood glucose levels

4
Physiology Cont: Insulin Basal (continuous) Prandial (Bolus) *Blood glucose increases within 10 minutes of the beginning of a meal*
 Prandial (Bolus) *Blood glucose increases within 10 minutes of the beginning of a meal*")
5
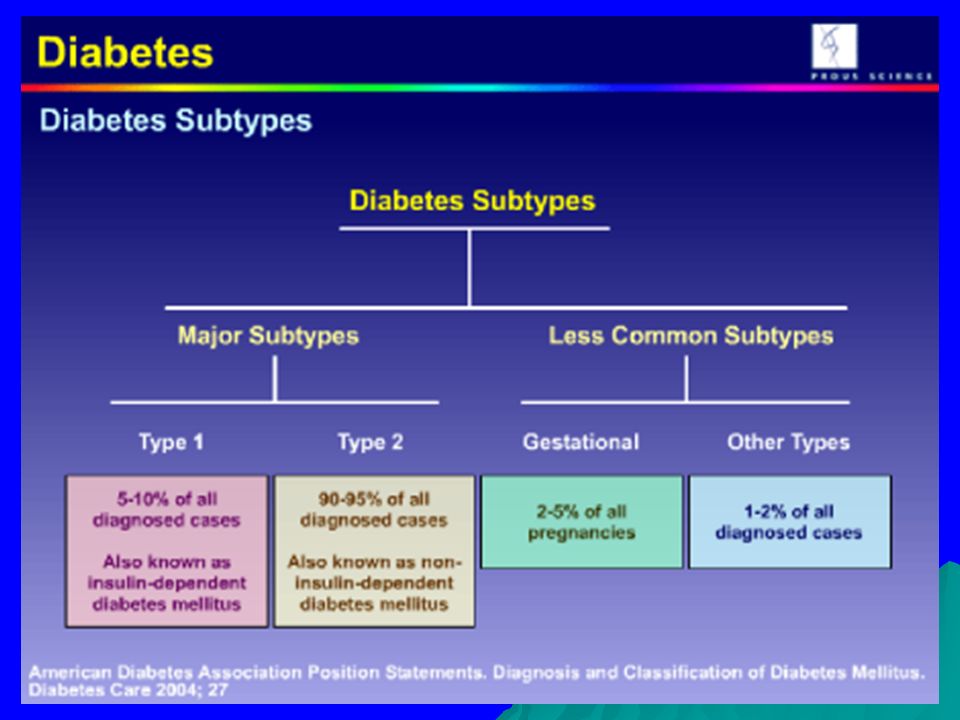
Diabetes Mellitus A disorder of carbohydrate, protein, and fat metabolism resulting from an imbalance between insulin availability and insulin need. (Porth, 2002) End Result : HYPERGLYCEMIA
 End Result : HYPERGLYCEMIA.")
7
Physiology Cont.:Glucose Control

8
Patho: DM Type 1

9
Patho Cont.: DM Type 2

10
Normal Physiology

11
Pathophysiology-Cont.:DM Type 2

12
DM 1&2: The big difference… DM TYPE 1 DM TYPE 2 No endogenous insulin Some endogenous insulin Tx requires insulin injections Tx diet and exercise 1st, then pills and /or insulin Usually < age 30 yrs. Usually over 30 yrs. (peaks at 50) Ketosis prone (DKA) no ketosis Former names: IDDM (Juvenile) Diabetes Type I NIDDM (maturity/adult- onset) Diabetes Type II Thin to normal body weight Usually Overweight Acute metabolic complications (DKA) Chronic vascular complications
 Ketosis prone (DKA) no ketosis Former names: IDDM (Juvenile) Diabetes Type I NIDDM (maturity/adult- onset) Diabetes Type II Thin to normal body weight Usually Overweight Acute metabolic complications (DKA) Chronic vascular complications.")
13
Case Study

14
THE 3 POLYs POLYURIA POLYPHAGIA POLYDYPSIA 14 Diabetes: Clinical Manifestations

15
Signs and Symptoms Diabetes Clinical Manifestations Cont: Signs and Symptoms Early signs 3 Polys Weight loss Fatigue/Always tired Visual Blurring Late signs Any of the 3 Polys Infections Numbness/ tingling of feet or leg pain Slow healing wounds Chronic Complications

16
Diabetes: Dx Tests Diabetes: Dx Tests Fasting Blood Glucose (FBG): <100 mg/dL –Iggy: 70-110 mg/dL *Random/Casual Blood Glucose*:<200 mg/dL Oral Glucose Tolerance Test (OGTT): < 140 mg/dL Glycosylated Hemoglobin (HgbA1C): 4-6% Check MD orders or agency protocol for frequency of BS Monitoring In General: AC&HS if pt able to eat; Q4-6 hours if NPO or tube feedings
: <100 mg/dL –Iggy: mg/dL *Random/Casual Blood Glucose*:<200 mg/dL Oral Glucose Tolerance Test (OGTT): < 140 mg/dL Glycosylated Hemoglobin (HgbA1C): 4-6% Check MD orders or agency protocol for frequency of BS Monitoring In General: AC&HS if pt able to eat; Q4-6 hours if NPO or tube feedings")
17
Diabetes: Diagnostic Tests Cont. Glycosylated hemoglobin test – Hemoglobin A1C (HbA1c) – –measures the amount of glycosylated hemoglobin (hemoglobin that is chemically linked to glucose) in blood. –Normal -4-6% –Target range DM patient <7%
 – –measures the amount of glycosylated hemoglobin (hemoglobin that is chemically linked to glucose) in blood. –Normal -4-6% –Target range DM patient <7%.")
18
HbA1C Control

19
Criteria for the Diagnosis of Diabetes Mellitus Normal –FPG <110 mg per dL –2hr OGTT <140 mg per dL Diabetes- positive findings from any two of the following tests on different days: –Symptoms of diabetes mellitus* plus casual (random) plasma glucose concentration >=200 mg / dL or –FPG >=126 mg per dL or –2hr OGTT >=200 mg per dL after a 75-g glucose load
 plasma glucose concentration >=200 mg / dL or –FPG >=126 mg per dL or –2hr OGTT >=200 mg per dL after a 75-g glucose load")
20
Diagnostic Tests – Cont. Is it Diabetes Yet? Impaired Fasting Glucose Impaired Glucose Tolerance <6 100-125 140-200 <100 <140 >126 >200 >6

21
Acute Complications Diabetic Ketoacidosis (DKA) BS > 300 mg/dL Classic symptoms Ketosis Hyperglycemic- Hyperosmolar Nonketotic Syndrome (HHNS) BS > 800 mg/dL Similar symptoms No Ketosis Check urine for ketones
 BS > 300 mg/dL Classic symptoms Ketosis Hyperglycemic- Hyperosmolar Nonketotic Syndrome (HHNS) BS > 800 mg/dL Similar symptoms No Ketosis Check urine for ketones")
22
(ADA)
")
23
Chronic Complications of DM

24
Effects on Blood Vessels Blood Vessel Lumen

25
Chronic Complications - Macrovascular Cardiovascular –heart disease Cerebrovascular –Stroke Peripheral vascular disease DM pts have heart disease and stroke risks 2 to 4 X higher than non-DM pts

26
Chronic Complications- Microvascular : Diabetic Retinopathy The leading cause of new cases of blindness in adults ages 20 - 74

27
Chronic Complications- Microvascular Nephropathy The leading cause of end-stage renal disease (ESRD), occurs in about 20 - 40% of patients with diabetes
, occurs in about % of patients with diabetes")
28
Chronic Complications-Microvascular Diabetic Neuropathy - Diabetic Neuropathy - the poor blood supply will cause the nervous system to malfunction

29
Chronic Complications- Microvascular Amputation of Toes

30
Chronic Complications- Microvascular Sexual problems for men erectile dysfunction retrograde ejaculation Sexual problems for women decreased vaginal lubrication decreased sexual response Urologic problems for men and women urinary tract infections neurogenic bladder

31
Chronic Complications- Microvascular Gastroparesis Nerve damage to the digestive system most commonly causes constipation. Damage can also cause the stomach to empty too slowly

32
MANAGEMENT OF DM Regular Blood Glucose Monitoring Diet Exercise Drug Therapy 32

33
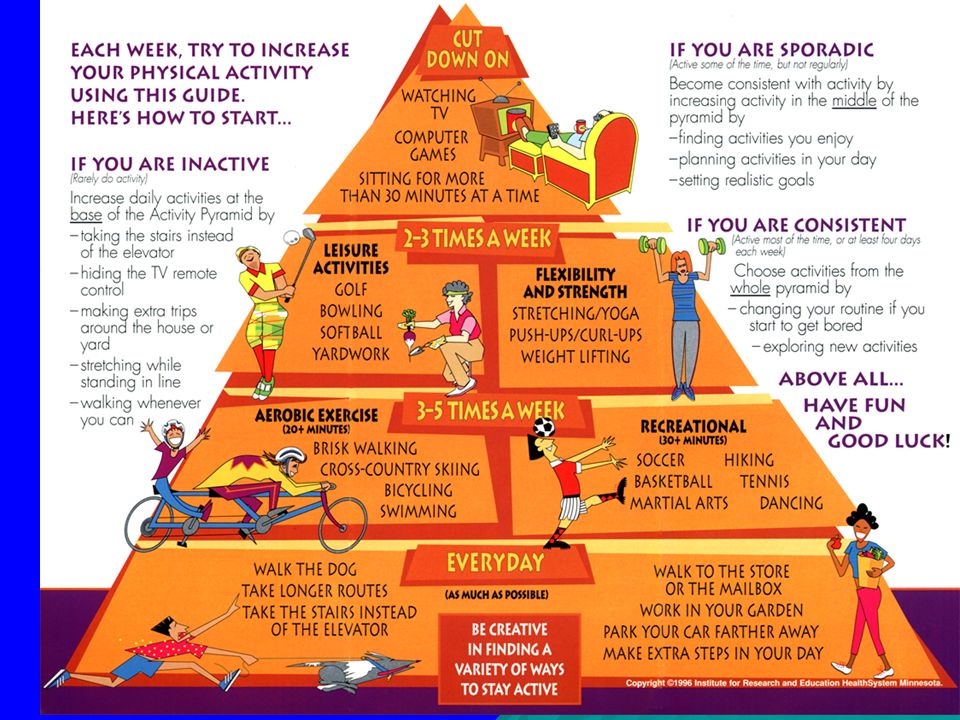
Management: Diet & Exercise

34
Diet : Diet : Diabetes Food Pyramid

35
Diet Cont: What to do???

36
Diet Cont. Carb-Counting

37
Diet Cont: Diet Cont: Glycemic Index

38
Diet Cont.: Getting the balance right Get your portions right!!

39
Management: Exercise Helps regulate blood glucose Increases insulin effectiveness and sensitivity in the body. Must monitor insulin and food intake to match exercise regimen.

41
Drug Therapy Insulin& Oral Antidiabetic Agents

42
Drug Therapy: Insulin Types Fast-acting insulin – –Rapid Acting Insulin AnalogsRapid Acting Insulin Analogs Aspart, Lispro, Glulisine – –Regular Human InsulinRegular Human Insulin Intermediate-acting insulin – –NPH Human InsulinNPH Human Insulin – –Pre-Mixed InsulinPre-Mixed Insulin Humulin 70/30, Humalog 75/25 Long-acting insulin – –Insulin Glargine, Insulin Detemir BASAL Used to lower blood sugar throughout the day and night BOLUS Used to lower blood sugar after eating a meal

43
Drug Therapy Cont.: Insulin Onset - how soon it starts to work in the blood Peak - when the insulin has the greatest effect on blood sugar levels Duration – how long it keeps working

44
Drug Therapy Cont: Goal of Insulin Therapy Basal and Bolus Insulin Coverage

45
Drug Therapy Cont: Sample Insulin Regimen (NPH & Regular insulin)
")
46
Drug Therapy-Insulin Cont: Rapid Acting “Logs” Humalog (insulin lispro) Novolog (insulin aspart) Bolus insulin Onset 15 min; peaks 1-2 hrs; lasts 4-6 hours Ideal for meal coverage “Give the shot while the plate is hot!”
 Novolog (insulin aspart) Bolus insulin Onset 15 min; peaks 1-2 hrs; lasts 4-6 hours Ideal for meal coverage Give the shot while the plate is hot!")
47
Drug Therapy-Insulin Cont: Short Acting: Regular Insulin Regs Bolus insulin Onset ½-1 hr; peaks 2-4 hrs; lasts 6-8 hrs Give 30 minutes to 1 hour before a meal

48
Drug Therapy-Insulin Cont: Short Acting: Regular Insulin ♪ It’s time give you your regular insulin ♪ ♪ It’s time to give it 30 minutes before your plate is in ♪ ♪ Come back to check you in 2 (hours) ♪ ♪ Watch out for shakes and sweats too ♪ ♪ If your lucky you’ll have no clue!!!! ♪

49
Drug Therapy-Insulin Cont: Drug Therapy-Insulin Cont: Rapid Acting (Humalog/Novolog) VS. Short Acting (Regular Insulin) Rapid onset 1-2 hour peak Limited duration Delayed onset Peaks in 2-4 hr Lasts 6-8 hours
 Rapid onset 1-2 hour peak Limited duration Delayed onset Peaks in 2-4 hr Lasts 6-8 hours.")
50
Drug Therapy-Insulin Cont: Intermediate acting: NPH Insulin Basal insulin: covers blood sugar between meals Satisfies overnight insulin requirement Onset 1-2 hrs, peaks 6-10 hrs, lasts 12+ hrs Need snack if NPH given at 5 pm (only) Ideal to be given at 9 pm (HS) to address Dawn Phenomenon
 Ideal to be given at 9 pm (HS) to address Dawn Phenomenon")
51
Drug Therapy-Insulin Cont: L ong-Acting: Peakless Insulins!!! L antus (insulin glargine) L evimir (insulin detimir) Basal Insulin Onset 1.5 hrs; no peak (max effect in 5 hrs); lasts 24 hours No risk for hypoglycemia Do not mix with other insulins – becomes inactivated when mixed with other insulins
 L evimir (insulin detimir) Basal Insulin Onset 1.5 hrs; no peak (max effect in 5 hrs); lasts 24 hours No risk for hypoglycemia Do not mix with other insulins – becomes inactivated when mixed with other insulins.")
52
Lantus

53
Drug Therapy- Insulin Cont: Hypoglycemia BS < 60-70 mg/dL An acute complication of insulin administration Tx: (15/15 or 20/20 Rule) –Give 15/20 g simple carb and recheck BG in 15/20 minutes
 –Give 15/20 g simple carb and recheck BG in 15/20 minutes")
54
Synthetic injectables Byetta: Synthetic incretin mimetic hormone – –Indicated for patients with type 2 diabetes who don’t use insulin Symlin: Synthetic analogue of human amylin – –Approved for use with insulin in adults with type 1 and type 2 diabetes

55
Drug Therapy Cont: Other Methods of Administration For Uncontrolled DM 1 0r 2 Rapid-acting insulin

56
Continuous IV insulin infusion Used to maintain glycemic control in hospitalized patients with high blood glucose levels; in DKA and HHNS Regular insulin may be used IV May also be given preoperatively or postoperatively More frequent BS monitoring ( q1- 2 hours per agency protocol)
")
57
Drug Therapy Cont: Drug Therapy Cont: Oral Antidiabetic agents (see handout)
")
58
New Oral Med Januvia (Sitagliptin) – –An oral drug that reduces blood sugar levels in patients with type 2 diabetes.diabetes – – Sitagliptin is the first approved member of a class of drugs that inhibit the enzyme, dipeptidyl peptidase-4 (DPP-4).
 – –An oral drug that reduces blood sugar levels in patients with type 2 diabetes.diabetes – – Sitagliptin is the first approved member of a class of drugs that inhibit the enzyme, dipeptidyl peptidase-4 (DPP-4).")
59
Oral Agents: How do they work?

60
Acute Complication of Insulin and (some) Oral Meds Hypoglycemia Acute Complication of Insulin and (some) Oral Meds Hypoglycemia
 Oral Meds Hypoglycemia Acute Complication of Insulin and (some) Oral Meds Hypoglycemia")
61
Hyperglycemia

62
Critical Thinking Exercises Course Packet pp. 81-84

63
Diabetic Teaching Needs Disease process S/S of hyperglycemia and hypoglycemia Blood sugar monitoring DietExercise Drug therapy Sick Day Rules Complications (acute and chronic) Prevention: Foot care, eye exam etc.
 Prevention: Foot care, eye exam etc.")
64
DIABETES can be controlled!!!

Similar presentations












 Diabetes Mellitus.>")






