Download presentation
Presentation is loading. Please wait.

2
1 Diabetes Mellitus Dr. Belle Erickson With thanks to Karen McKenna, MSN, RN

3
2 PANCREAS - An Endocrine Gland n Islets of Langerhans –Beta Cells »INSULIN – Alpha Cells »GLUCAGON

4
3 INSULIN n Lowers blood sugar by: –Transporting glucose into cell Receptor sites –Converting glucose to glycogen for storage in muscle and liver tissue(glycogenesis) –Converting excess glucose into fat cells, forming lipids from fatty acids (lipogenesis) and promoting storage in adipose tissue
 –Converting excess glucose into fat cells, forming lipids from fatty acids (lipogenesis) and promoting storage in adipose tissue")
5
4 GLUCAGON n Known as Hyperglycemic agent n Promotes activities that raise blood sugar- - - Converting of stored glycogen to glucose (Glycogenolysis) Formation of glucose from protein and fat sources (Gluconeogenesis)
 Formation of glucose from protein and fat sources (Gluconeogenesis)")
6
5 Hormones affecting CHO metabolism n ACTH (Adrenocorticotropic hormone) and Glucocorticoids –enhances gluconeogenesis n Epinephrine –enhances glycogenolysis
 and Glucocorticoids –enhances gluconeogenesis n Epinephrine –enhances glycogenolysis")
7
6 Vocabulary n Glucose n Glucagon n Glycogen n Glycogenesis n Gluconeogenesis n Glycogenolysis n Lipogenesis n Glycolysis

8
7 Carbohydrate Metabolism n Active transport of glucose into cells & metabolism of glucose with release of energy n Storage of glucose n Conversion of glycogen back to glucose n Conversion of proteins to glucose

9
8 CHO (not enough) n Decreased blood sugar & depleted glycogen stores n Unable to use available glucose
 n Decreased blood sugar & depleted glycogen stores n Unable to use available glucose")
10
9 Body needs energy source n Catabolism of fats and proteins Where? n Ketones

11
10 Diabetes Mellitus n Chronic disorder characterized by hyperglycemia –Imbalance between Insulin supply & demand n Abnormal metabolism of fat, carbohydrate, & protein

12
11 Types of DM n *Type 1 (IDDM) 10 - 15 % of all Diabetics n *Type 2 85 - 90-% of all cases n Secondary n Gestational n (High Risk) Impaired Glucose Tolerance
 % of all Diabetics n *Type % of all cases n Secondary n Gestational n (High Risk) Impaired Glucose Tolerance")
13
Type l (Type I) IDDM = Insulin Dependent Diabetes Mellitus Juvenile Diabetes Body produces NO INSULIN Must take at least one injection of insulin per day to control blood sugar Usually occurs before 30 years old Body weight thin or ideal Onset abrupt Know This Stuff
 IDDM = Insulin Dependent Diabetes Mellitus Juvenile Diabetes Body produces NO INSULIN Must take at least one injection of insulin per day to control blood sugar Usually occurs before 30 years old Body weight thin or ideal Onset abrupt Know This Stuff")
14
TYPE 2 Type II Adult/Maturity Onset NIDDM = Non Insulin Dependent Diabetes Mellitus n Body does not produce enough insulin and/or n Body cannot use the insulin it has made Know This Stuff

15
TYPE 2 Type II Adult/Maturity Onset NIDDM = Non Insulin Dependent Diabetes Mellitus n May control blood sugar with diet and exercise alone (but may take oral meds. or insulin) n Clients usually > 35/40 years old n Clients usually overweight/obese n 1/2 go undiagnosed for years & by then complications can be underway Know This Stuff
 n Clients usually > 35/40 years old n Clients usually overweight/obese n 1/2 go undiagnosed for years & by then complications can be underway Know This Stuff.")
17
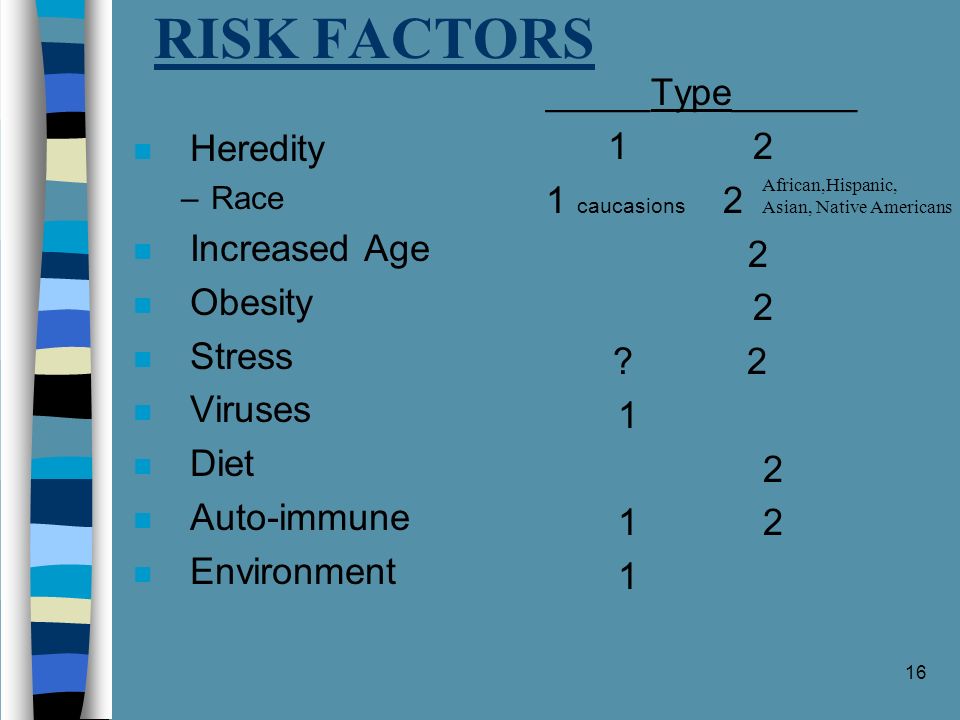
16 RISK FACTORS n Heredity –Race n Increased Age n Obesity n Stress n Viruses n Diet n Auto-immune n Environment _____Type______ 1 2 1 caucasions 2 2 ? 2 1 2 1 2 1 African,Hispanic, Asian, Native Americans

18
17 DM - Pathophysiology n Lack of Insulin n Glucose Where? ECF n Fat & Protein breakdown n Ketosis & Negative Nitrogen balance n Hyperglycemia - - - WHY?

19
18 Pathophysiology (cont’d) n Intracellular fluid deficit n Glycosuria n ECF deficit n Signs of DM
 n Intracellular fluid deficit n Glycosuria n ECF deficit n Signs of DM")
20
19 Four Cardinal Symptoms n Polyuria n Polydypsia n Polyphagia n Weight Loss

21
20 WARNING SIGNS -TYPE 1 usually occur suddenly n 3 “poly’s” & weight loss n irritability n weakness and fatigue n nausea and vomiting

22
21 WARNING SIGNS -TYPE 2 usually occur less suddenly & may be very mild n any of the Type 1 signs n recurring or hard-to-heal skin, gum or bladder infections n drowsiness n blurred vision n tingling or numbness in hands or feet n itching

24
23 Assessment - Lab Studies FBS Postprandial glucose Glycosylated Hgb (Hb A 1c ) normal value is 3-8% (Oral Glucose Tolerance Test =OGTT) (Fractionals)
 normal value is 3-8% (Oral Glucose Tolerance Test =OGTT) (Fractionals)")
25
24 Control n Normal FBS n B.S. 180mg 2hrs. after a meal n Glycosylated Hgb 10% or less n Normal weight and general good health

26
25 Diabetes Management n Diet management n Physical Activity n Medications

27
Recommended Nutrient Intake PROTEIN10 -20% of total energy intake FAT< 30% (Depends on lipid & glucose levels) CARBOHYDRATE40-60% of total intake (Based on glucose & lipid levels and client’s habits) NCS ***FIBER***20-35 grams Fiber slows/moderates blood absorption of carb/glucose
 CARBOHYDRATE40-60% of total intake (Based on glucose & lipid levels and client’s habits) NCS ***FIBER***20-35 grams Fiber slows/moderates blood absorption of carb/glucose")
28
6 MAJOR EXCHANGE LISTS MILK Non-Fat, Low Fat VEGETABLE All Non-Starchy Vegetables FRUIT All Fruits & Fruit Juices BREAD Bread, Cereal, Pasta, Starchy Vegetables & Prepared Foods MEAT Lean Meat, Medium & High Fat & Other Protein Rich Food FATS Polyunsaturated, Saturated and Non Saturated

29
28 Medications Type 1 –Insulin NOT ORALLYAdministered SQ or IV NOT ORALLY NOT IN TUBE FEEDINGS NOT IN TUBE FEEDINGS Type 2 –Oral Hypoglycemic Agents –Insulin

30
29 Insulin n Types of insulin n Duration of action Short - Intermediate - Long n Action Onset - Peak - Duration

31
30 Insulin - (cont’d) n Concentration –Expressed in Units U100 n Insulin Order NPH Humulin (U100) 32U SQ daily before dinner
 n Concentration –Expressed in Units U100 n Insulin Order NPH Humulin (U100) 32U SQ daily before dinner")
32
31 Types of Humulin Insulin and Comparative Actions

33
32 Sliding Scale Insulin Measure BG at -7am -11am - 4pm - 9pm Give Humulin Regular Insulin BG Value Dosage 150-200 0 units 201-250 2 units 251-300 4 units 301-350 6 units 351-400 8 units over 400 call MD under 50give 6oz OJ repeat BS

34
33 Insulin n Dosage –Individual requirements –Individual response

35
34 Insulin Administration n Check Order n Gather equipment n Insulin - Precipitate

36
35 Administration - cont’d n Combining Insulins –30U of NPH & 6U of Regular n Drawing up n Injecting –NO aspiration - 90 0 angle not 45 0

37
Special Things About Regular Insulin n Only one to give IV n Only one to give in Emergencies n Only one to give for coverage n Given via Insulin Pump (or Humalog)
")
39
38 Teaching n Pathophysiology n Diet n Exercise n Diabetes Mellitus ID n Sexuality n Community Resources n Stress Management n Health Care

40
39 Teaching n Home management –Insulin administration storage travel exercise sick days

41
40 Insulin pumps n Mimic release of pancreas –electro - mechanical with computer chip n Basal rate (++) n Sub-Q n Complications
 n Sub-Q n Complications")
42
41 Oral Hypoglycemic Agents n Sulfonylureas n Insulin ? n Functioning Beta Cells n OOC on diet and exercise n Action –release insulin from beta cells –enhance sensitivity of receptor sites n *Metformin - (Glucophage) guanidine derivative not a sulfonylureas
 guanidine derivative not a sulfonylureas.")
43
42 Physical Activity n Exercise –Lowers BS levels – uptake of free fatty acids –lower cholesterol & triglycerides –promote cardiac stabillity –reduce stress & sense of well-being

Similar presentations








 muscle proteins liver glycogen fat lipids glucose.>")
 muscle proteins liver glycogen fat lipids glucose.>")








 bring them back to life on this planet! Scientists.>")
 state>")


>")