Download presentation
Presentation is loading. Please wait.

1
MEDICAL PARASITOLOGY Laboratory diagnosis Of parasitic diseases By
S.S Eghbali ApCp BPUMS 2008

2
Definitions Medical parasitology: the study of the parasites of man and their medical consequences. Parasite: living organism requiring intimate prolonged contact with another living organism to meet some of its basic nutritional needs. In a more restricted definition, it refers to organisms that are not viruses, bacteria, fungi, rickettsia, or chlamydia and obviously include organisms of varying complexity from a unicellular protozoa to a complex multicellular helminths.

3
Host: organism harboring a parasite.
Definitive host: animal harboring the adult or sexually mature stage of the parasite. Intermediate host: animal in which development occurs but in which adulthood is not reached. Life cycle: for survival and reproduction reasons many parasites evolve through a number of morphologic stages and several environments or different hosts. The sequence of morphologic and environmental stages is referred to as the life cycle. Parasitic infection: invasion by endoparasites (protozoa and helminths).
.")
4
Parasitic disease: invasion and pathology produced by endoparasites.
Parasitic infestation: external parasitism by ectoparasites (arthropods). Commensalisms: the association of two different species or organism in which one is benefited and the other is neither benefited nor harmed. (e.g. non pathogenic intestinal protozoa) Reservoir host: an animal that harbors a species of parasite that can be transmitted to and infect man.
. Commensalisms: the association of two different species or organism in which one is benefited and the other is neither benefited nor harmed. (e.g. non pathogenic intestinal protozoa) Reservoir host: an animal that harbors a species of parasite that can be transmitted to and infect man.")
5
Vector: an arthropod or other living carrier that transports a pathogenic organism from an infected to a non-infected host. Carrier: a host that harbors a parasite but exhibits no clinical signs or symptoms. Zoonosis: a disease involving a parasite for which the normal host is an animal, and wherein man can also be infected. Protozoa: a subkingdom consisting of unicellular eukaryotic (Greek-karyon=nut=nucleus) animals.
 animals.")
6
Vector: an arthropod or other living carrier that transports a pathogenic organism from an infected to a non-infected host. Carrier: a host that harbors a parasite but exhibits no clinical signs or symptoms. Zoonosis: a disease involving a parasite for which the normal host is an animal, and wherein man can also be infected. Protozoa: a subkingdom consisting of unicellular eukaryotic (Greek-karyon=nut=nucleus) animals.
 animals.")
7
INFORMATION EMPHASIS Agent ID and general importance Epidemiology (transmission, distribution, etc) Agent damage capability Diagnostics Control

8
Epidemiology Although parasitic infections occur globally, the majority occur in tropical regions, where there is poverty, poor sanitation and personal hygiene Often entire communities may be infected with multiple, different organisms which remain untreated because treatment is neither accessible nor affordable Effective prevention and control requires "mass intervention strategies” and intense community education. Examples include: General improved sanitation: pit latrines, fresh water wells, piped water Vector control: insecticide impregnated bed nets, spraying of houses with residual insecticides, drainage, landfill Mass screening and drug administration programmes which may need to be repeated at regular intervals

9
The burden of some major parasitic infections
Parasite Diseases No. people infected Deaths/yr Plasmodium malaria 273 million 1.12 million Soil transmitted helminths: Roundworm (Ascaris) Whipworm (Trichuris) Hookworm (Ancylostoma and Necator) Pnemonitis, intestinal obstruction Bloody diarrhoea, rectal prolapse Coughing, wheezing, abdominal pain and anaemia 2 billion 200,000 Schistosoma Renal tract and intestinal disease 200 million 15,000 Filariae Lymphatic filariasis and elephantiasis 120 million Not fatal but 40 million disfigured or incapacitated Trypanasoma cruzi Chagas disease (cardiovascular) 13 million 14,000 African trypanosomes African sleeping sickness 0.3 – 0.5 million 48,000 Leishamania Cutaneous, mucocutaneous and visceral leishmaniasis 12 million; 2 million new cases/yr 50,000
 Whipworm (Trichuris) Hookworm (Ancylostoma and Necator) Pnemonitis, intestinal obstruction. Bloody diarrhoea, rectal prolapse. Coughing, wheezing, abdominal pain and anaemia. 2 billion. 200,000. Schistosoma. Renal tract and intestinal disease. 200 million. 15,000. Filariae. Lymphatic filariasis and elephantiasis. 120 million. Not fatal but 40 million disfigured or incapacitated. Trypanasoma cruzi. Chagas disease (cardiovascular) 13 million. 14,000. African trypanosomes. African sleeping sickness. 0.3 – 0.5 million. 48,000. Leishamania. Cutaneous, mucocutaneous and visceral leishmaniasis. 12 million; 2 million new cases/yr. 50,000.")
10
Parasitology - protozoology (protozoa), helmintology(worms), enthomology(insects)
Laboratory diagnosis: - life cycle of parasits, material v laboratory diag. Protozoa – intestinal, genital, urinary, blood, tissue Worms - Helmints: Nematodes, Cestodes,Trematodes Ectoparasits: louse, ticks, flies – important as vectors

11
Life cycle of parasits -terminology
Complex life cycle – key to diagnosis Host – hosts Definitive host – parasit finishes the growing cycle and is becoming adult in it Not typical host - parasit cannot develop in it Transient host – larves are developing in it and not sexual multiplication is performed Helmints : egg - larvae - adult worm Protozoa :trophozoite - motile cysts – non motile sexual multiplication - zygota asexual- schizonts, sporogons

12
Diagnosis Problematic, not ususals outside endematic areas
Nonspecific clinical manifestation eosinophilia in helmintoses – not constant sign Importance of history – personal, travellers, social, economic, food, therapy Conditions for successful dg: - think on parasitosis - také a good sample – right sample, with good method at right time, send it in appropriate conditions to the lab that is able to identify the parasite, good interpretation: - Knowledge of life cycle is principal

13
Laboratory diagnosis Usually based on morphology (microscopic)
Demonstration of the parasit in different stages of life cycle in clinical material Macroscopic examination of the sample (stool or tissue) Microscopic examination – native smear, staining, concentration method Serology – detection of antibodies, detection of antigénes Genetic probes - detection, identification Cultivation Animal model
 Microscopic examination – native smear, staining, concentration method. Serology – detection of antibodies, detection of antigénes. Genetic probes - detection, identification. Cultivation. Animal model.")
14
Stool for parasitological examination
Macroscopy – blood, mucous, adult worms Microscopy - native smear - iodine – motility, eggs of helmints, cysts of protozoa, Rbc,Wbc Concentration methods – separation of cysts of protozoa and eggs of helmints from other material in the stool Staining - identification – smear of native stool + hematoxylin eosin, trichrome

15
Other material acc.to clinical manifestation
Perianal - Enterobius vermicularis Sigmoidoscopy - Entamoeba histolytica Duodenal aspiration - Giardia lamblia Biopsy of abscess of liver - Entameba histolytica Sputum - Ascaris lumbricoides, Strongyloides, Urine - Schistosoma Hematobium Urogenital sample - Trichomonas Blood - (malaria, trypanosomiasis, leishmaniosis, filariosis) smear, thick drop - staining Giemsa, H&E, Serum (Hydatid cyst)
 smear, thick drop - staining Giemsa, H&E, Serum (Hydatid cyst)")
16
Protozoa Amoeba - Entamoeba histolytica, Entamoeba coli, Naegleria fowleri, Acanthamoeba, Endolimax nana Flagelata - Giardia lamblia, Trichomonas vaginalis, Leishmania, Trypanosoma Ciliata - Balantidium coli Coccidia a Sporosoa - Cryptosporidium, Blastocystis, Microsporidia, Plasmodia, Babesia,, Toxoplasma

17
Nematodes -worms Enterobius vermicularis, Ascaris lumbricoides, Toxocara canis,cati, Trichuris trichiura, Ancylostoma duodenale, Strongyloides stercoralis, Trichinella spiralis, Wuchereria bancrofti, Dracunculus medinensis Nonsegmented body, adult worms living in the GIT-e, - diagnosisa: identification of eggs in the stool (morphology of eggs) Filariae – tin worms parasiting in eye, skin, tissue, transmitted by insects. Larval form- microfilariae penetrate to blood and are transmitted by suckling insect
 Filariae – tin worms parasiting in eye, skin, tissue, transmitted by insects. Larval form- microfilariae penetrate to blood and are transmitted by suckling insect.")
18
Cestodes - Head - scolex, segmented body
Hermafrodit, male and female organs are present in every segment - dif.dg. They have not GIT, absorbtion of food. Complex life cycle with transient host (sometimes - human – larval stage of cysticerkósis, echinococcosis) Taenia solium, Taenia saginata, Diphylobotrium latum, Echinococcus granulosus, Hymenolepsis nana
 Taenia solium, Taenia saginata, Diphylobotrium latum, Echinococcus granulosus, Hymenolepsis nana.")
19
Trematodes - Usually hermafrodits (ex Schistosoma) Need transient host
Fasciolopsis, Clonorchis, Paragonimus, Schistosoma

20
Enterobius vermicularis
Definitive host - human transient - none dg. – perianal sample – microscopy of eggs fecal oral transmission - autoinfection

21
Enterobius vermicularis

22
Ascaris lumbricoides Definitive host: human
Larva migrans: intestin, colon - muc.membrane - blood- lung - cough - mouth - colon dg. Egg in stool Infection via contaminated food Symptoms acc.to localisation of the larva

23
Ascaris lumbricoides

24
Toxocara canis, cati Definitive host dog, cat Transient host: rat
Human incidental: human (larves) dg. serology transmission: hand food
 dg. serology. transmission: hand food.")
25
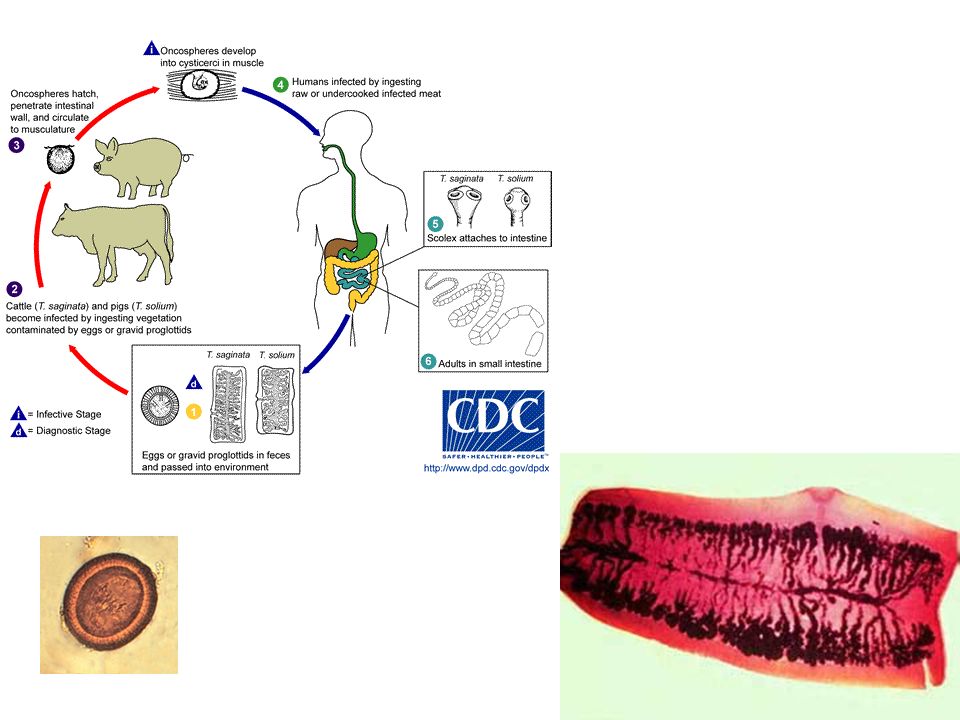
Taenia saginata Definitive: human transient: cattle
dg. Segments in stool Transmission cysticercus in beef

26
Taenia solium Definitive: pig transient: rat
incidental: human in small intestin dg. Serology,body Rare Contaminated food

28
Echinococcus granulosus
definitive: dog transient:sheep incidental: human Diagnosis: serology,Direct methods transmission: cyste in meat infection: mechanic pressure from expanded cyst, prolonged growing, rupture of the cyst and dissemination

29
Echinococcus granulosus

30
Entamoeba histolytica
definitive: human Diagnosis:trophozoites in stool, serology dysenteria – diarhea with blood

31
Entamoeba histolytica

33
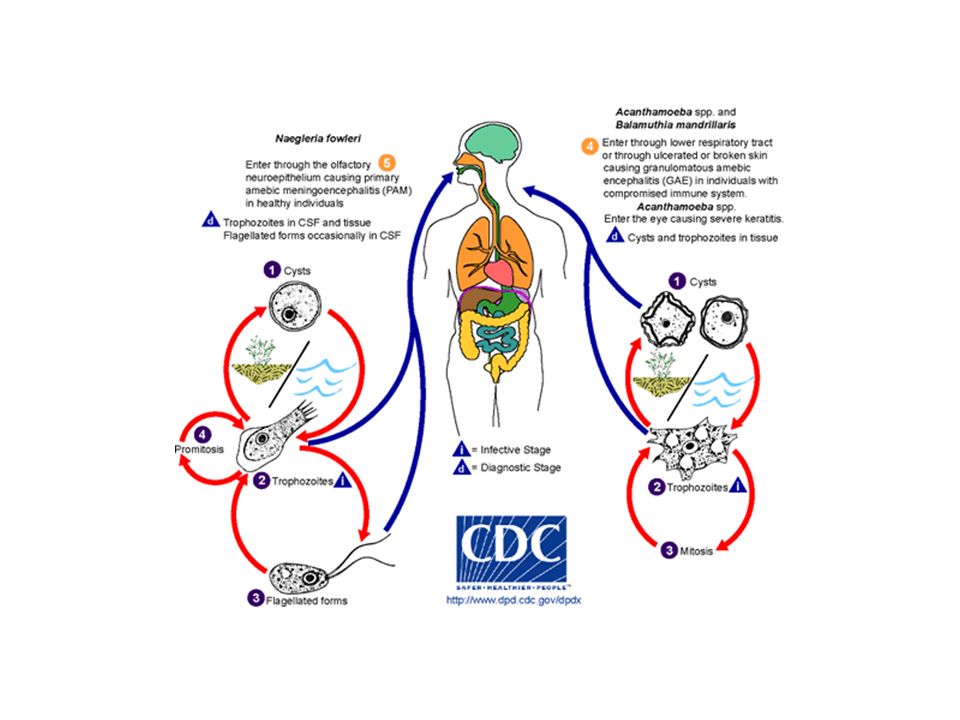
Naegleria fowleri, Acantamoeba,Balamuthia
Free Living in water Human (via nose) Diagnosis:microscopy in CSF- identification of invasive strains Diseases:Negleriafowleri:P.A.M Balamuthia:G.A.E,Acantamoeba:Keratitis
 Diagnosis:microscopy in CSF- identification of invasive strains. Diseases:Negleriafowleri:P.A.M Balamuthia:G.A.E,Acantamoeba:Keratitis.")
36
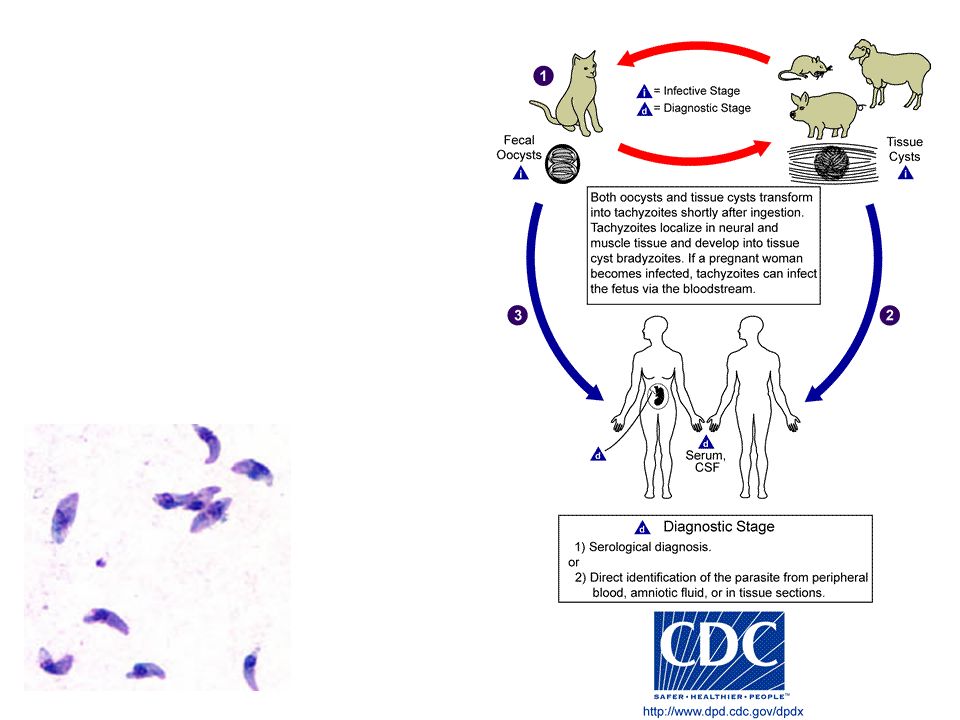
Toxoplasma gondii Definitive: cat transient: rat incidental: human
Diagnosis: serology , IgA, IgG, IgM transmission: food borne, hand, annimal disease: - intrauterine primoinfection generalized lymphadenopathy, encystation in organs – abortion, eye……..

38
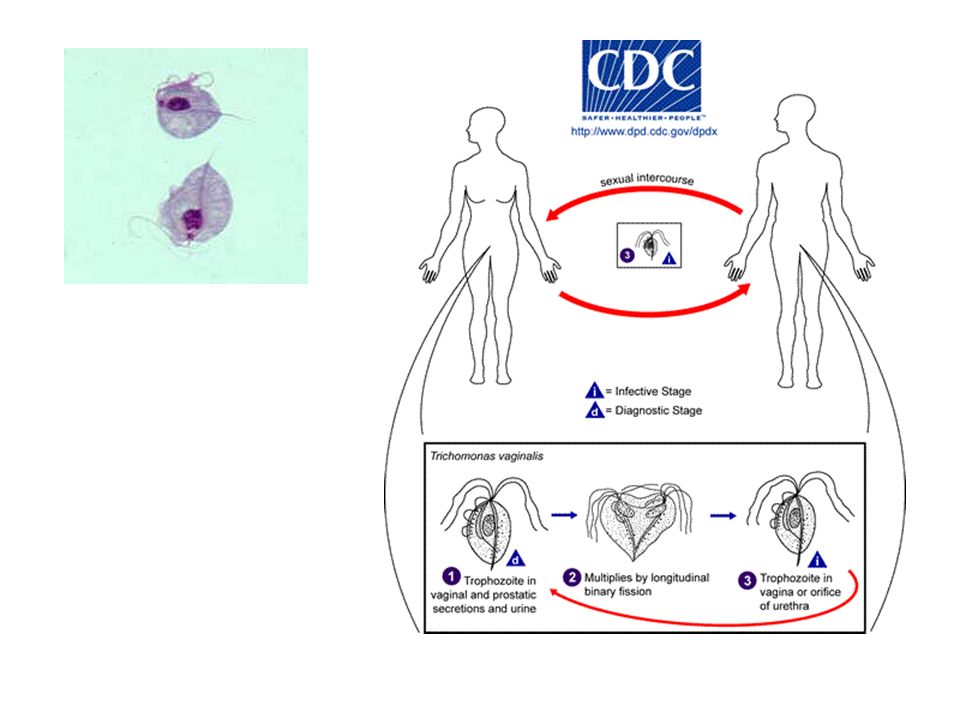
Trichomonas vaginalis
Definitive: human transient: none dg. Cultivation - microscopy trophozoite - from vagina, urine Sexual transmission Therapy of both (all) partners
 partners.")
40
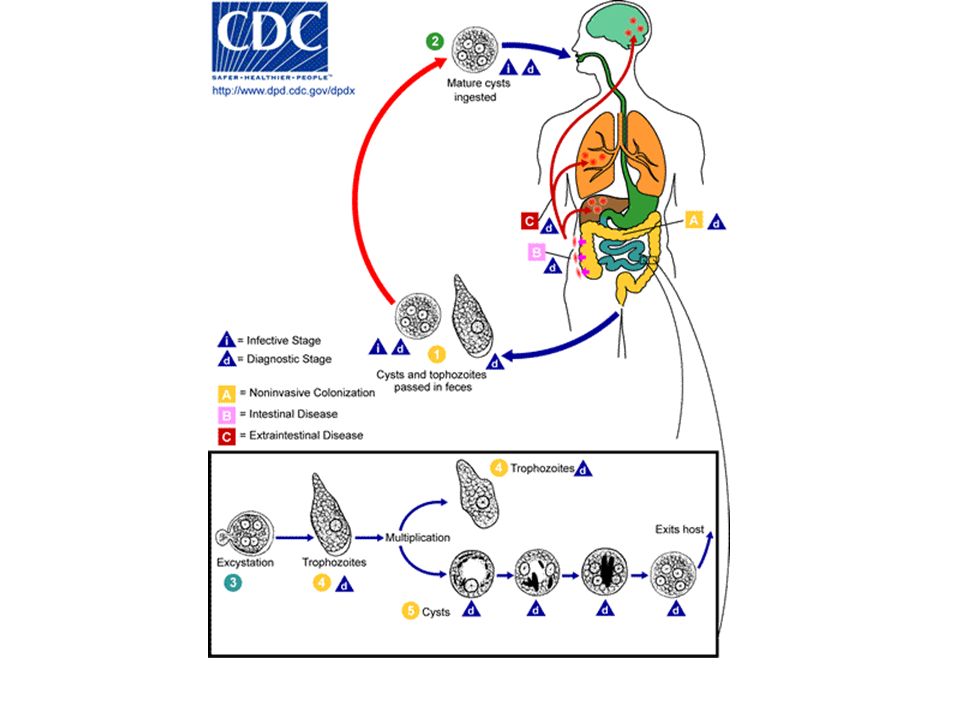
Giardia lamblia definitive: human – small intestin,dog, cat
transient: non Diag:microscopy – cysts and trophozoits in stool, transient in duodenal secretion Transmission contaminated food malabsorption

41
Giardia lamblia

42
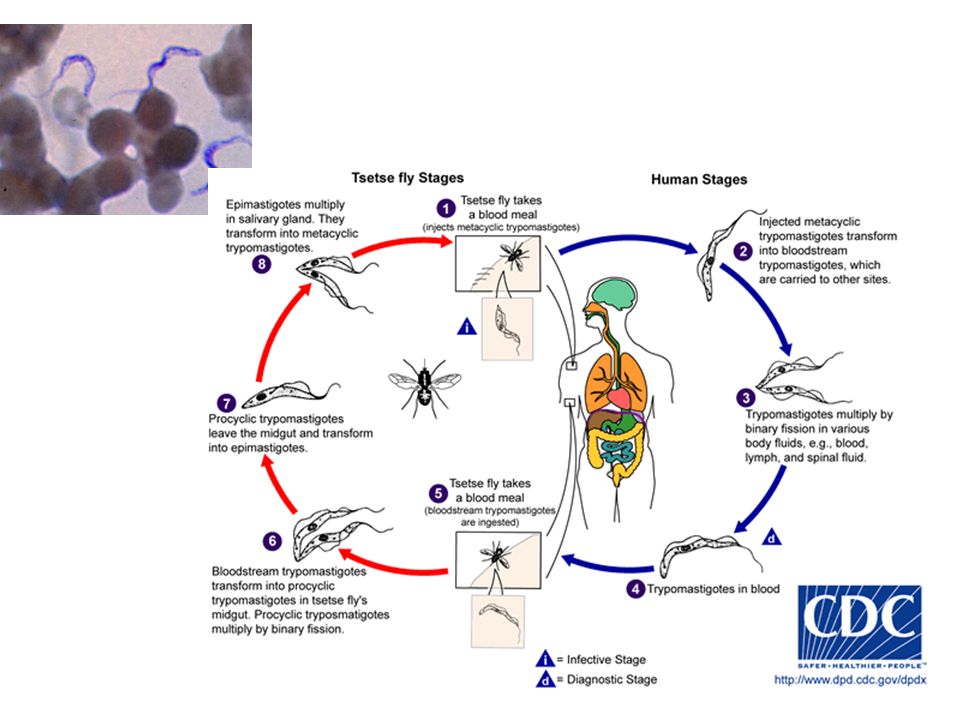
Trypanosoma gambiensis (spavá choroba)
Definitive host: insect - fly tse tse transient: human, monkey dg.microscopy – thick drop Transmission bite Disease – sleeping disease, myalgia, arthralgia, lymphadenopathy, hyperactivity in acute phase, lethargy, meningoencephalitis, coma

44
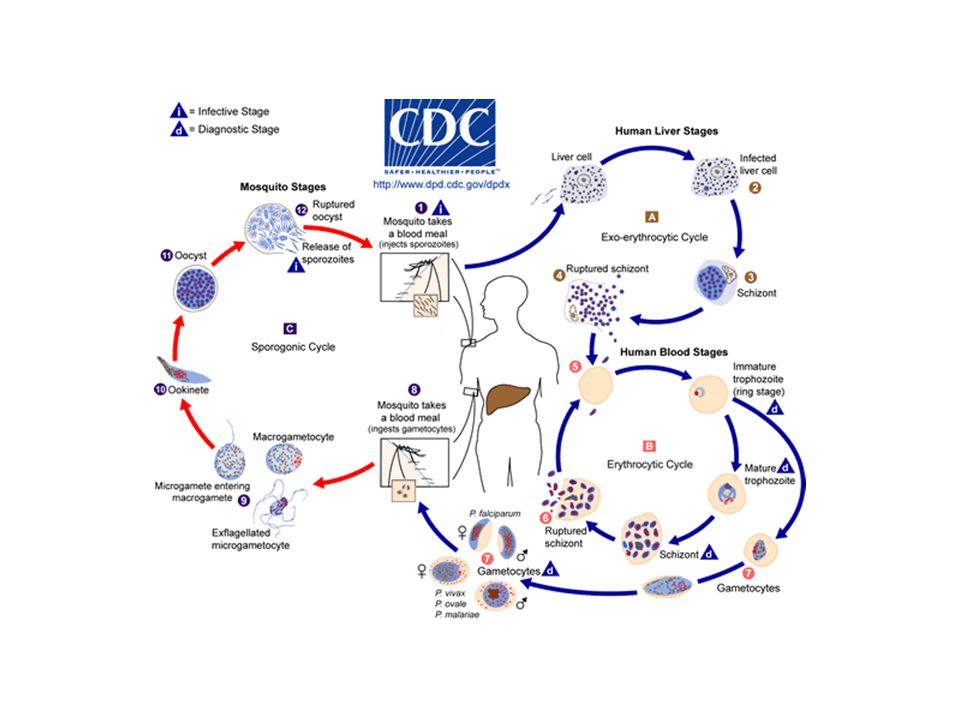
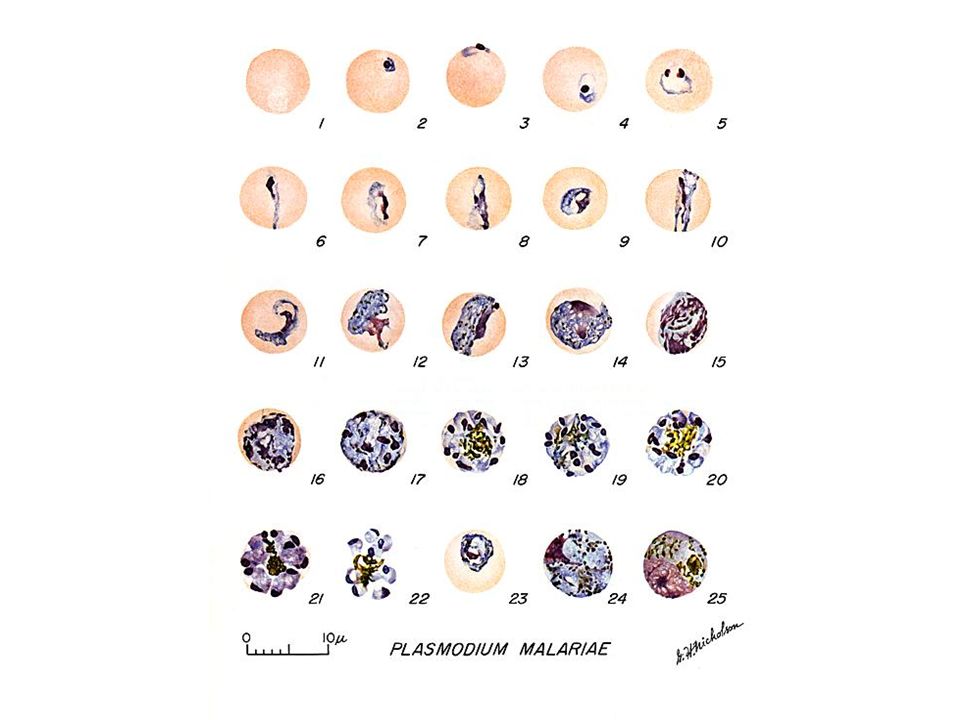
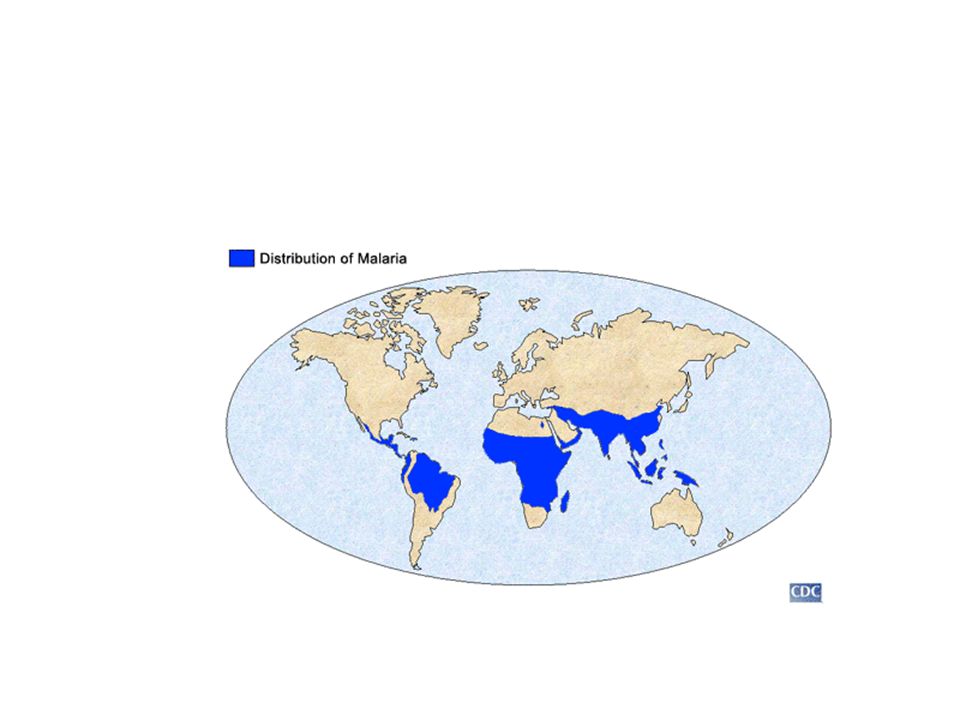
Plasmodium-malariae, falciparum
Definitive host:Anopheles Transient host: human, monkey Diag:microscopy thick drop Transmission insect bite disease: malaria acc.to the rate of schizogonia- clinically as fever attacks - tercianna, quartana,

48
CONTROL OF PARASITIC DISEASES
A CHALLENGE FOR OUR FUTURE PUV

49
COMPLEXITY OF PARASITIC DISEASES AND PROBLEMS
The complexity of zoonotic infectious diseases offers, however, several problems which must be solved: Although the general knowledge on the disease epidemiology and transmission is usually available, the knowledge on local epidemiology and transmission characteristics is still lacking in many cases Multisdisciplinary approaches and transprofessional team networks are needed for both research and training. Efforts will be needed to convince different ministries and health responsibles to co-work and related political-strategic difficulties must be solved Funding agencies shall be convinced about the need for increasing efforts at animal level Studies on geographical distribution and epidemiology of zoonoses by using modern tools are crucial to establish the appropriate local control measures Field work shall again be encouraged The need for “old-fashioned” disciplines as Medical Malacology and Entomology shall be emphasized DPUV

50
THE NEED TO AGAIN EMPHASIZE THE IMPORTANCE OF FIELD STUDIES
Experimental work has sense if it is for the understanding of what happens outside During years and years we have been developping numerous new, modern, sophisticated molecular tools for the diagnosis of many infectious diseases; once the new test obtained, a field trial has been usually performed to verify its usefulness; and afterwards, only a few or nobody is applying it in endemic areas Too sophisticated to be applied in many developing countries Too expensive and consequently unaffordable DPUV Too much similar tests for the same disease, so that health responsibles become lost

51
THE NEED TO AGAIN EMPHASIZE THE IMPORTANCE OF FIELD STUDIES
Divorce between traditional methods (as those for simple epidemiological surveys) and new technologies In many centres of developing countries, health responsibles think that traditional diagnostic methods are old fashioned and make efforts to incorporate modern methods which are usually more expensive, need sophisticated infrastructure and not appropriate for large epidemiological studies in endemic areas The consequence is that those modern techniques are only used in a few centres and applied to only a few patients, and that almost nobody is carrying out surveys in the endemic areas any more DPUV
 and new technologies. In many centres of developing countries, health responsibles think that traditional diagnostic methods are old fashioned and make efforts to incorporate modern methods which are usually more expensive, need sophisticated infrastructure and not appropriate for large epidemiological studies in endemic areas. The consequence is that those modern techniques are only used in a few centres and applied to only a few patients, and that almost nobody is carrying out surveys in the endemic areas any more. DPUV.")
52
THE NEED TO AGAIN EMPHASIZE THE IMPORTANCE OF FIELD STUDIES
Consequences: Today, one of the greatest problems we have is that in many areas of the developing world we do not know which are the epidemiological situations So, for given diseases we dispose of more or less effective control methods and we cannot apply them D PUV

53
THE NEED TO AGAIN EMPHASIZE THE IMPORTANCE OF FIELD STUDIES
Interestingly, when we go today again to the field and perform surveys, the results usually suggest that many diseases are emerging / re-emerging Whether this is related to the higher performance of today diagnostic methods when compared to old ones or not, one conclusion is evident: all those diseases are still there and continue to be as prevalent as always ! Thus, evidence is suggesting small impact or sometimes even no impact at all of all our efforts against neglected infectious diseases in recent years; given diseases are really re-emerging and/or expanding ! PUVD

54
TRAINING, TECHNOLOGY TRANSFER, CAPACITY BUILDING
Control of all kind of infectious diseases needs sustainability Sustainibility needs specifically trained scientists in endemic countries and areas Consequently, we need to include training and technology transfer high in the agendas of research projects on zoonotic diseases Problems appeared in recent years: There begins to be a lack of people in traditional but always necessary disciplines for the fight against vector-borne diseases, as Medical Entomology and Medical Malacology, or even coprological methodology, needed for patient diagnosis in many diseases, mainly in endemic areas of developing countries Molecular tools may be very helpful in attracting young researchers to disciplines as Medical Entomology and Medical Malacology, as well as to diagnostic methodologies as coprology DPUV

55
CONTROL OF PARASITIC DISEASES
A CHALLENGE FOR OUR FUTURE PUV

56
Thank you for your attention
Any Question?

Similar presentations


, helmintology(worms), enthomology(insects) Laboratory.>")
 Drs. Babcock and Hopkins Spring 2009>")












 : Protozoa: 1- Protozoa are unicellular (eukaryotic) or acellular organisms. 2- Protozoan is measured in microns;>")

>")

, helmintology(worms), enthomology(insects) Laboratory.>")