Download presentation
Presentation is loading. Please wait.

1
Ali Zahedmehr, Interventional Cardiologist Shahid Rajaie Cardiovascular medical and research center

2
Common Asymptomatic Readily detectable Easily treatable Leads to lethal complications if left untreated.

3
Hypertension doubles the risk of cardiovascular diseases.

4
Average systolic blood pressure is higher for men than for women during early adulthood, although among older individuals the age- related rate of rise is steeper for women.

5
blood pressure heritabilities are in the range of 15–35%.

6
Mechanisms of Hypertension Intravascular volume Autonomic nervous system Renin-Angiotensin-Aldosterone Vascular

7
vascular volume Salt and water go with each other.

8
When NaCl intake exceeds the capacity of the kidney to excrete sodium, vascular volume initially expands and cardiac output increases.

9
However, many vascular beds (including kidney and brain) have the capacity to autoregulate blood flow, and if constant blood flow is to be maintained in the face of increased arterial pressure, resistance within that bed must increase.
 have the capacity to autoregulate blood flow, and if constant blood flow is to be maintained in the face of increased arterial pressure, resistance within that bed must increase.")
11
over time, peripheral resistance increases and cardiac output reverts toward normal.

12
Autonomic nervous system Norepinephrine»»»»»α Epinephrine »»»»»β

13
α 1 Receptors are located on postsynaptic cells in smooth muscle and elicit vasoconstriction.

14
α 2 Receptors are localized on presynaptic membranes of postganglionic nerve terminals that synthesize norepinephrine. When activated by catecholamines, α 2 receptors act as negative feedback controllers, inhibiting further norepinephrine release.

15
Activation of myocardial ß 1 receptors stimulates the rate and strength of cardiac contraction, and consequently increases cardiac output. ß 1 Receptor activation also stimulates renin release from the kidney.

16
Activation of ß 2 receptors relaxes vascular smooth muscle and results in vasodilation.

17
Pheochromocytoma is the most obvious example of hypertension related to increased catecholamine production.

18
One arterial baroreflex is mediated by stretch- sensitive sensory nerve endings located in the carotid sinuses and the aortic arch. The rate of firing of these baroreceptors increases with arterial pressure, and the net effect is a decrease of sympathetic outflow, resulting in decreases of arterial pressure and heart rate.

19
However, the activity of the baroreflex declines or adapts to sustained increases of arterial pressure such that the baroreceptors are reset to higher pressures.

20
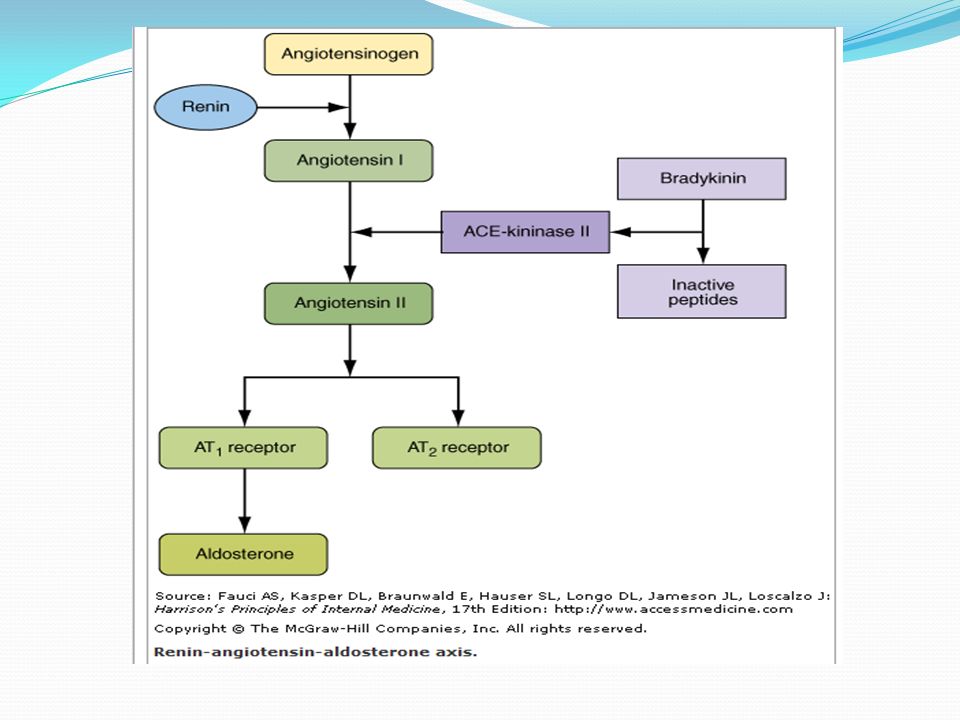
Renin-Angiotensin-Aldosterone Most renin in the circulation is synthesized in the segment of the renal afferent renal arteriole (juxtaglomerular cells) that abuts the glomerulus and a group of sensory cells located at the distal end of the loop of Henle, the macula densa.
 that abuts the glomerulus and a group of sensory cells located at the distal end of the loop of Henle, the macula densa.")
22
There are three primary stimuli for renin secretion: (1) decreased NaCl transport in the thick ascending limb of the loop of Henle (macula densa mechanism) (2) decreased pressure or stretch within the renal afferent arteriole (baroreceptor mechanism) (3) sympathetic nervous system stimulation of renin- secreting cells via ß 1 adrenoreceptors.
 decreased NaCl transport in the thick ascending limb of the loop of Henle (macula densa mechanism) (2) decreased pressure or stretch within the renal afferent arteriole (baroreceptor mechanism) (3) sympathetic nervous system stimulation of renin- secreting cells via ß 1 adrenoreceptors.")
23
Vascular mechanisms Hypertrophic or eutrophic (no change in the amount of material in the vessel wall) vascular remodeling results in decreased lumen size and hence contributes to increased peripheral resistance. Ion transport Vascular endothelial function

24
Pathologic Consequences of :Hypertension Heart Heart disease is the most common cause of death in hypertensive patients.

25
Hypertensive heart disease is the result of structural disease: -Left ventricular hypertrophy -Diastolic dysfunction - CHF -Abnormalities of blood flow due to atherosclerotic coronary artery disease and microvascular disease -Cardiac arrhythmias

26
Aggressive control of hypertension can regress or reverse left ventricular hypertrophy and reduce the risk of cardiovascular disease.

27
Brain Hypertension is an important risk factor for brain infarction and hemorrhage.

28
Autoregulation over a wide range of arterial pressures (mean arterial pressure of 50–150 mmHg)
")
29
hypertensive encephalopathy severe headache nausea and vomiting (often of a projectile nature) focal neurologic signs Alterations in mental status.
 focal neurologic signs Alterations in mental status.")
30
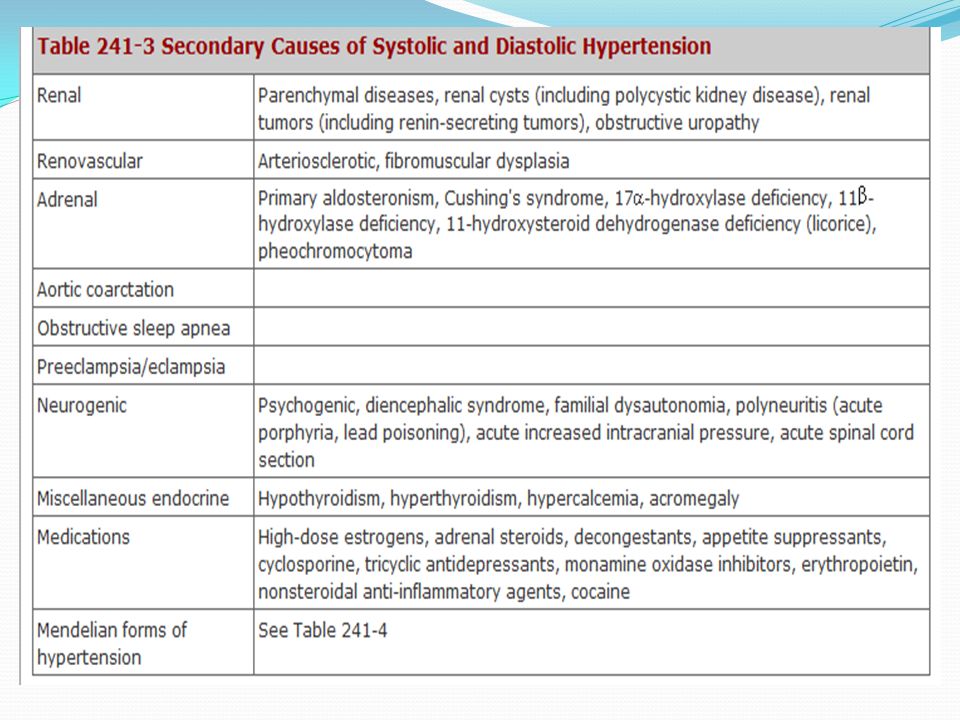
Kidney Primary renal disease is the most common etiology of secondary hypertension. Conversely, hypertension is a risk factor for renal injury and ESRD.

31
Peripheral Arteries intermittent claudication An ankle-brachial index 50% stenosis in at least one major lower limb vessel.

32
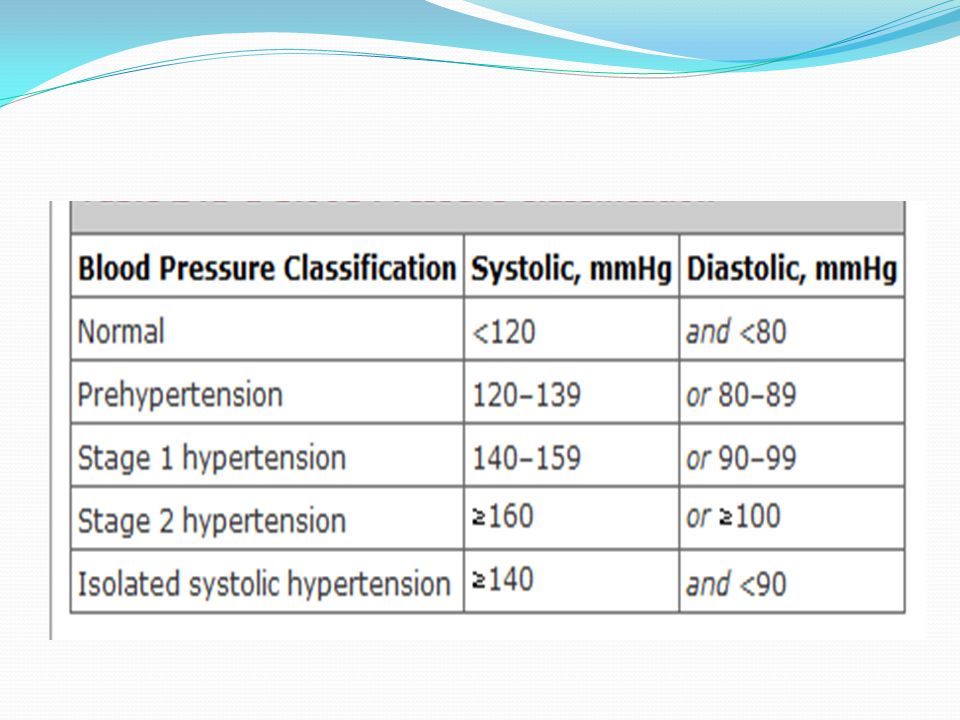
Defining Hypertension The average of two or more seated blood pressure readings during each of two or more outpatient visits.

34
White coat hypertension

35
Clinical disoders of HTN 80–95% of hypertensive patients are diagnosed as having "essential" hypertension.

38
Essential Hypertension Plasma Renin Activity (PRA) 10–15% : High PRA vasoconstrictor form 25% : low PRA volume-dependent hypertension
 10–15% : High PRA vasoconstrictor form 25% : low PRA volume-dependent hypertension")
39
Metabolic Syndrome The constellation of insulin resistance, hypertension, and dyslipidemia has been designated as the metabolic syndrome.

40
Physical Examination At the initial examination, blood pressure should be measured in both arms, and preferably in the supine, sitting, and standing positions to evaluate for postural hypotension.

41
Even if the femoral pulse is normal to palpation, arterial pressure should be measured at least once in the lower extremity in patients in whom hypertension is discovered before age 30.

42
Funduscopic examination Auscultation for bruits over the carotid and femoral arteries Palpation of femoral and pedal pulses.

44
Hypertension: Treatment Lifestyle Interventions:

45
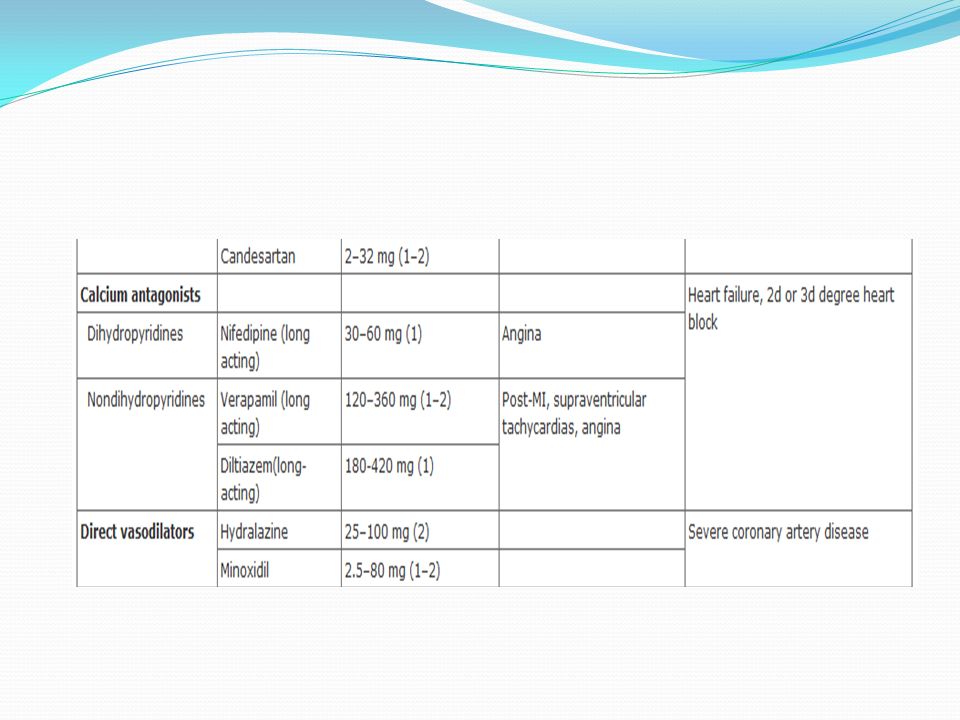
Pharmacologic Therapy Drug therapy is recommended for individuals with blood pressures 140/90 mmHg.

48
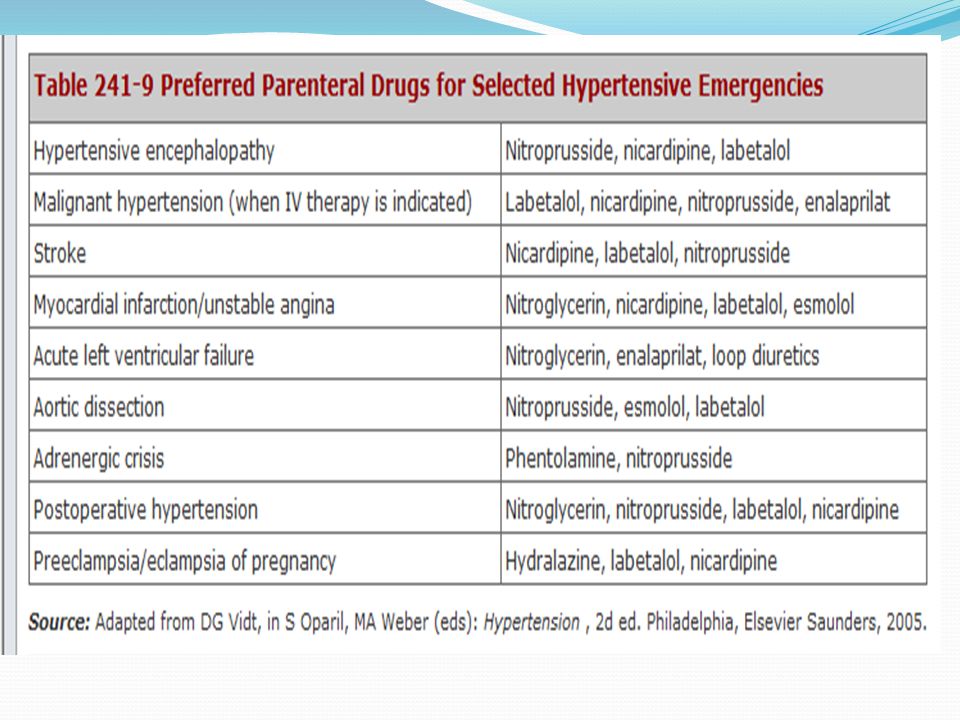
Hypertensive Emergencies The degree of target organ damage, rather than the level of blood pressure alone, determines the rapidity with which blood pressure should be lowered.

50
Malignant hypertension The absolute level of blood pressure is not as important as its rate of rise.

51
Progressive retinopathy Deteriorating renal function with proteinuria Microangiopathic hemolytic anemia Encephalopathy

52
Initial goal of therapy is to reduce mean arterial blood pressure by no more than 25% within minutes to 2 h or to a blood pressure in the range of 160/100–110 mmHg.

Similar presentations




>")















. –Coagulation cascade Regulation of blood pressure. Regulation of blood volume. Reading; Sherwood, Chapters 10 &11, Chapter.>")
