Download presentation
Presentation is loading. Please wait.

1
Mohammed Alshurem R2 Neurology resident 2013 July 24 th Emergency lecture series Neurology Half academic Day

2
Content 1-Historical context 2-Definition 3-Diagnostic Criteria 4-Ancillary test 5-Organ donation

3
Historical context before the 1800s: general medical opinion focused on the heart as the residence for a person’s central and controlling “life force.” Late 1800s: Machado and his colleagues did number of experiments demonstrated situations in which patients with high intracranial pressure ceased to have respirations but continued to have beating hearts shortly thereafter Horsley, Duckworth and Cushing noted that patients with disease states such as intracerebral hemorrhage and brain tumors that increase intracranial pressure tended to pass away first from respiratory failure rather than circulatory arrest.

4
mid-1970s: The advent of resuscitative measures such as electroshock and artificial ventilation, forced the medical community to reconsider the location of “vital principles” after the first electroencephalogram was recorded by Bergerin 1929: Sugar and Gerard were able to show in cats that an occlusion of a carotid artery resulted in the complete abolition of electric potentials in the brain Löfstedt and von Reis described 6 patients with apnea and absent brainstem reflexes who showed no intracranial blood flow during cerebral angiography but who did not have subsequent cardiac arrest until 2 to 26 days afterward

5
1959: Mollaret and Goulon “coma dépassé,” meaning “a state beyond coma,” 23 ventilated patients in which loss of consciousness, brain stem reflexes, and spontaneous respirations were associated with absent encephalographic activity. Wertheimer and Jouvet : description of ((death of the nervous system)), and criteria to stopping the ventilator in such cases.
), and criteria to stopping the ventilator in such cases..")
6
Definition Death is an irreversible, biological event that consists of permanent cessation of the critical functions of the organism as a whole. Brain death implies the permanent absence of cerebral and brainstem functions.

7
Diagnostic Criteria Guidelines Before American Academy of Neurology(1995-2010): Harvard Criteria (1968) Minnesota Criteria (1971) United Kingdom Criteria (1976) President’s Commission Criteria (1981) Unreceptivity and unresponsivity No spontaneous movement Establish etiologyUnreceptive and unresponsive coma No movements or breathing No spontaneous respirations when tested for a period of 4 min at a time Exclude mimicking conditions Absent papillary, corneal, oculocephalic, oculovestibular, oropharyngeal reflexes No reflexesAbsence of brain stem reflexes Absent motor response Apnea with Pco 2 greater than 60 mm Hg Flat electroencephalogra m A status in which all the findings above remain unchanged for at least 12 h Absent brainstem reflexes Absence of posturing or seizures
: Harvard Criteria (1968) Minnesota Criteria (1971) United Kingdom Criteria (1976) President’s Commission Criteria (1981) Unreceptivity and unresponsivity No spontaneous movement Establish etiologyUnreceptive and unresponsive coma No movements or breathing No spontaneous respirations when tested for a period of 4 min at a time Exclude mimicking conditions Absent papillary, corneal, oculocephalic, oculovestibular, oropharyngeal reflexes No reflexesAbsence of brain stem reflexes Absent motor response Apnea with Pco 2 greater than 60 mm Hg Flat electroencephalogra m A status in which all the findings above remain unchanged for at least 12 h Absent brainstem reflexes Absence of posturing or seizures")
8
Harvard Criteria (1968) Minnesota Criteria (1971) United Kingdom Criteria (1976) President’s Commission Criteria (1981) Exclusion of hypothermia (below 90°F or 32.2°C) and central nervous system depressants Electroencephalogram is not mandatory Apnea with a Pco 2 target of ≥50 mm Hg Irreversibility demonstrated by establishing cause and excluding reversible conditions (sedation, hypothermia, shock, and neuromuscular blockade) All the above tests shall be repeated at least 24 hours with no change. Spinal reflexes have no bearing on the diagnosis of brain death Prolonged observation in anoxic- ischemic injury Period of observation determined by clinical judgment Brain death can be pronounced only if the pathologic process for the above are deemed irreparable with presently artificial means. Temperature should be ≥35°C Use of cerebral flow tests when brainstem reflexes are not testable, sufficient cause cannot be established, or to shorten period of observation Electroencephalogram is not mandatory

9
CMA- 1987 The Clinical diagnosis Of brain death can be made when all the following criteria have been satisfied. 1.An Etiology has been established that is capable of causing brain death and potentially reversible conditions have been excluded 2.The Patient is in deep coma and shows no response within the cranial nerve distribution to stimulation of any part of the body. No Movements such as cerebral seizures, dyski-netic movements, "decorticate" Or decerebrate posturing arising from the brain are present 3.Brain-stem Reflexes are absent 4.The Patient is apneic when taken off the respirator for an appropriate time 5.The Conditions listed above persist when the patient is reassessed after a suitable interval

10
AAN Guidelines 2010 3 clinical finding to declare brain death - Come (with known irreversible cause) - Absence of brain stem reflex - Apnea
 - Absence of brain stem reflex - Apnea")
11
Prerequisites (all must be checked) Coma, irreversible and cause known Neuroimaging explains coma Central nervous system (CNS) depressant drug effect absent (if indicated toxicology screen; if barbiturates given, serum level <10 g/mL) No evidence of residual paralytics (electrical stimulation if paralytics used) Absence of severe acid-base, electrolyte, endocrine abnormality Normothermia or mild hypothermia (core temperature ≥36°C) Systolic blood pressure ≥100 mm Hg No spontaneous respirations
 Coma, irreversible and cause known Neuroimaging explains coma Central nervous system (CNS) depressant drug effect absent (if indicated toxicology screen; if barbiturates given, serum level <10 g/mL) No evidence of residual paralytics (electrical stimulation if paralytics used) Absence of severe acid-base, electrolyte, endocrine abnormality Normothermia or mild hypothermia (core temperature ≥36°C) Systolic blood pressure ≥100 mm Hg No spontaneous respirations")
12
Examination (all must be checked) Pupils nonreactive to bright light Corneal reflex absent Oculocephalic reflex absent (tested only if C-spine integrity ensured) Oculovestibular reflex absent No facial movement to noxious stimuli at supraorbital nerve, temporomandibular joint Gag reflex absent Cough reflex absent to tracheal suctioning Absence of motor response to noxious stimuli in all 4 limbs (spinally mediated reflexes are permissible)
 Pupils nonreactive to bright light Corneal reflex absent Oculocephalic reflex absent (tested only if C-spine integrity ensured) Oculovestibular reflex absent No facial movement to noxious stimuli at supraorbital nerve, temporomandibular joint Gag reflex absent Cough reflex absent to tracheal suctioning Absence of motor response to noxious stimuli in all 4 limbs (spinally mediated reflexes are permissible)")
14
Pupillary reflex

15
Corneal reflex

16
Vestibulocular reflex Oculocephalic test (dolls eyes)
")
17
Vestibulo-ocular reflex caloric test

18
Apnea testing (all must be checked) Patient is hemodynamically stable (even with the use of vasopressors) Ventilator adjusted to provide normocarbia (Paco 2 34–45 mm Hg) Patient preoxygenated with 100% Fio 2 for ≥10 minutes to Pao 2 ≥200 mm Hg Patient well-oxygenated with a positive end-expiratory pressure (PEEP) of 5 cm of water Provide oxygen via a suction catheter to the level of the carina at 6 L/min or attach T-piece with continuous positive airway pressure (CPAP) at 10 cm H2O Disconnect ventilator Spontaneous respirations absent Arterial blood gas drawn at 8–10 minutes, patient reconnected to ventilator Pco 2 ≥60 mm Hg, or 20 mm Hg rise from normal baseline value OR: Apnea test aborted
 Patient is hemodynamically stable (even with the use of vasopressors) Ventilator adjusted to provide normocarbia (Paco 2 34–45 mm Hg) Patient preoxygenated with 100% Fio 2 for ≥10 minutes to Pao 2 ≥200 mm Hg Patient well-oxygenated with a positive end-expiratory pressure (PEEP) of 5 cm of water Provide oxygen via a suction catheter to the level of the carina at 6 L/min or attach T-piece with continuous positive airway pressure (CPAP) at 10 cm H2O Disconnect ventilator Spontaneous respirations absent Arterial blood gas drawn at 8–10 minutes, patient reconnected to ventilator Pco 2 ≥60 mm Hg, or 20 mm Hg rise from normal baseline value OR: Apnea test aborted")
19
Ancillary test (only 1 needs to be performed; to be ordered only if clinical examination cannot be fully performed because of patient factors, or if apnea testing inconclusive or aborted) Cerebral angiogram Transcranial Doppler (TCD) Electroencephalogram (EEG) single-photon emission computed tomography (SPECT)
 Cerebral angiogram Transcranial Doppler (TCD) Electroencephalogram (EEG) single-photon emission computed tomography (SPECT)")
20
When severe facial trauma preventing complete brain stem reflex testing, preexisting pupillary abnormalities, and sleep apnea or severe pulmonary disease resulting in chronic retention of carbon dioxide Not confirmatory or supplemental

21
cerebral angiography Invasive Cerebral circulatory arrest is defined by a lack of opacification of the internal carotid arteries above the level of the petrous portion or of the vertebral arteries above the level of the atlanto-occipital junction

22
Transcranial Doppler Operator and patient dependent Depend on ability to obtain reliable signal 10% to 20% of patients will not have an adequate bone window for ultrasound transmission. when obtained, TCDs have a specificity of 98% to 100% and a sensitivity ranging from 88% to 99%.

23
EEG simple to perform and provides insight into the cortical activity of the brain difficult to interpret secondary to artifact in either a positive or negative direction. sedation and hypothermia may produce a false-positive result

24
(SPECT) ‘‘hollow skull’’ or ‘‘empty light bulb’’ sign
 ‘‘hollow skull’’ or ‘‘empty light bulb’’ sign")
25
Mimics need to R/O fulminant Guillain-Barre syndrome baclofen overdose barbiturate overdose delayed vecoronium clearance hypothermia

26
Red Flag normal computed tomography (CT) scan unsupported blood pressure absence of diabetes insipidus marked heart rate variations fever or shock marked metabolic acidosis hypothermia lower than 32°C as this is often accidental and reversible marked miosis (opiate or organophosphate toxicity) myoclonus (lithium or selective serotonin reuptake inhibitor [SSRI] toxicity) rigidity (SSRI or haloperidol toxicity) positive urine or serum toxicology
![Red Flag normal computed tomography (CT) scan unsupported blood pressure absence of diabetes insipidus marked heart rate variations fever or shock marked metabolic acidosis hypothermia lower than 32°C as this is often accidental and reversible marked miosis (opiate or organophosphate toxicity) myoclonus (lithium or selective serotonin reuptake inhibitor [SSRI] toxicity) rigidity (SSRI or haloperidol toxicity) positive urine or serum toxicology](http://images.slideplayer.com/23/6568787/slides/slide_26.jpg "Red Flag normal computed tomography (CT) scan unsupported blood pressure absence of diabetes insipidus marked heart rate variations fever or shock marked metabolic acidosis hypothermia lower than 32°C as this is often accidental and reversible marked miosis (opiate or organophosphate toxicity) myoclonus (lithium or selective serotonin reuptake inhibitor [SSRI] toxicity) rigidity (SSRI or haloperidol toxicity) positive urine or serum toxicology")
27
Organ donation organs that can be transplanted are the kidneys, heart, lungs, liver, pancreas, and intestines A single donor can provide organs for 8 people Organ donation in numbers (AS OF 31 DECEMBER 2012) DONORS 120 RECIPIENTS 346 PATIENTS ON THE WAITING LIST 1250
 DONORS 120 RECIPIENTS 346 PATIENTS ON THE WAITING LIST 1250")
28
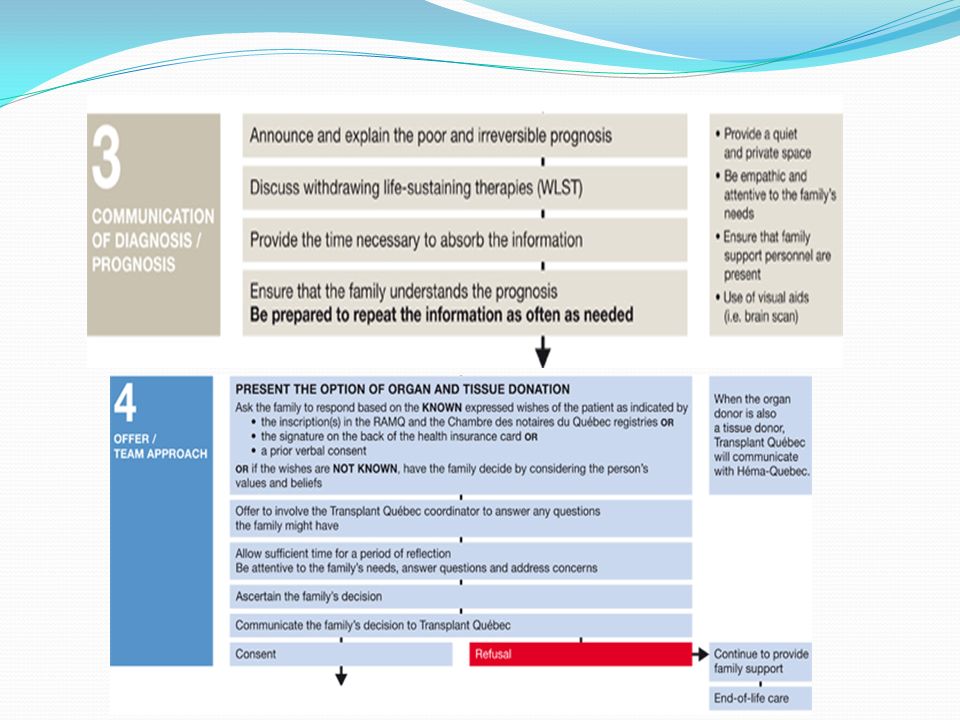
Who is a potential organ donor? A potential organ donor is a mechanically ventilated patient of any age with severe primary neurological damage., some patients may present with severe neurological damage that is secondary to an end-stage organ failure such as pulmonary or cardiac failure. In most cases, these people are diagnosed with: stroke cerebral anoxia (following cardiopulmonary arrest, hanging, drowning, poisoning, etc.) encephalopathy major, severe head trauma
 encephalopathy major, severe head trauma.")
29
http://www.transplantquebec.ca/sites/defa ult/files/eva-gui-001a_v2.pdf http://www.transplantquebec.ca/sites/defa ult/files/eva-gui-001a_v2.pdf

32
Tissue donation Bone, skin, heart valves, tendons, and corneas are the main types of tissues used for grafts A single donor can provide tissues to 15 other people. Héma-Québec

33
References Diagnosis of brain death, G Bryan Young. Uptodate.G Bryan Young Assessment of Brain Death in the Neurocritical Care Unit, David Y. Hwang, Neurosurgery Clinics of North AmericaVolume 24, Issue 3, July 2013, Pages 469– 482 David Y. Hwang Neurosurgery Clinics of North AmericaVolume 24, Issue 3 Evidence-based guideline update:Determining brain death in adults:Report of the Quality Standards Subcommittee of the American Academy of Neurology. Eelco F.M. Wijdicks, Panayiotis N. Varelas, Gary S. Gronseth, et al Neurology 2010;74;1911-1918 http://www.transplantquebec.ca http://www.hema-quebec.qc.ca

34
THANK YOU ANY QUESTION What is the treatment of brain death ?

Similar presentations