Download presentation
Presentation is loading. Please wait.

1
Good Morning 12 November 2002

2
Pituitary Tumor with Acromegaly 麻醉科 林子富

3
Case Summary A 43-year-old male Schizophrenia under medical control for 20 + years Insidious onset of enlargement of the jaw, hands, nose and feet which became prominent in recent 3 years Endocrinology work-up and brain MRI revealed pituitary tumor Called on our OPD for surgical intervention DM, HTN: -- Family history: --

4
NE: intact VF: hemianopia (L>R) CBC, coagulation profile, blood chemistry: WNL Endocrinology: T3, T4, TSH, cortisol: WNLT3, T4, TSH, cortisol: WNL Elevated GHElevated GH MRI of sella: pituitary microadenoma Surgical tumor excision Endonasal, transsphenoidEndonasal, transsphenoid
 CBC, coagulation profile, blood chemistry: WNL Endocrinology: T3, T4, TSH, cortisol: WNLT3, T4, TSH, cortisol: WNL Elevated GHElevated GH MRI of sella: pituitary microadenoma Surgical tumor excision Endonasal, transsphenoidEndonasal, transsphenoid")
11
Pituitary Disease and Anesthesia M. Smith and N. P. Hirsch. Br J Anaesth 2000; 85: 3–14

12
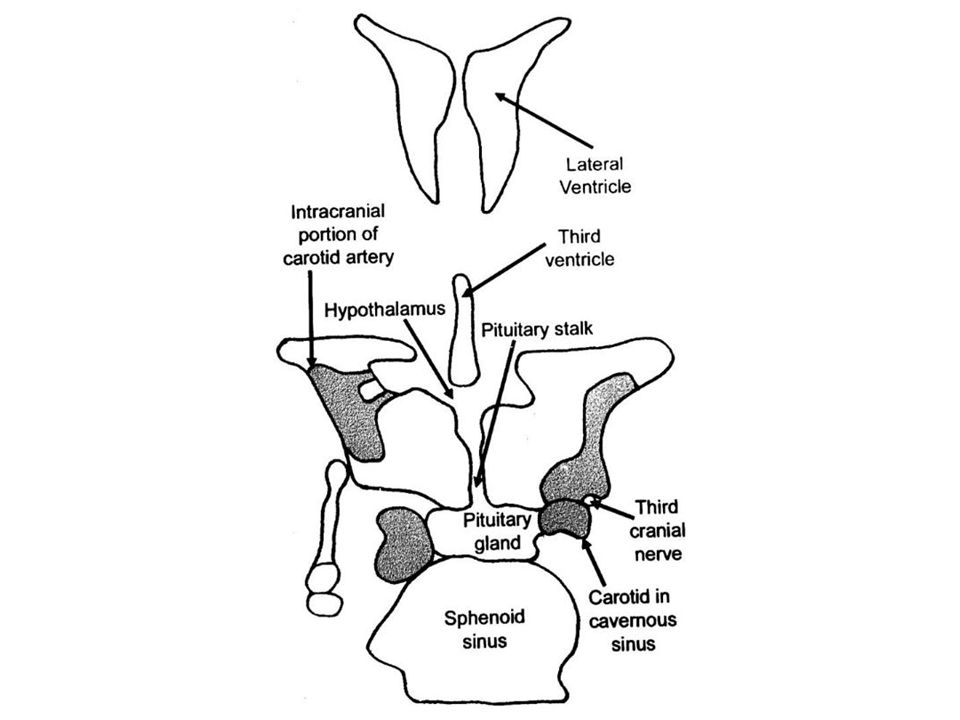
Anatomy The large anterior lobe or adenohypophysis and the smaller posterior lobe or neurohypophysis The gland averages 6 × 13 × 9 mm 3 Lie within the pituitary fossa or sella turcica Bounded by the roof of the sphenoid air sinus and cavernous sinuses which contain the carotid arteries and the third, fourth and sixth cranial nerves

14
Physiology At least five cell types within the anterior lobe: Somatotrophs: growth hormone; 50%Somatotrophs: growth hormone; 50% Prolactin-producing lactotrophs; 10–25%Prolactin-producing lactotrophs; 10–25% ACTH-producing corticotrophs; 15%.ACTH-producing corticotrophs; 15%. Thyrotrophs: TSH; 5–10%Thyrotrophs: TSH; 5–10% Gonadotrophs: FSH and LH; 10%Gonadotrophs: FSH and LH; 10% Null cells: non-functioning pituitary adenomasNull cells: non-functioning pituitary adenomas

15
Growth Hormone Growth hormone acts on a wide variety of tissues, both directly and through release of insulin-like growth factor I (IGF-I).Growth hormone acts on a wide variety of tissues, both directly and through release of insulin-like growth factor I (IGF-I). In addition to stimulating bone and cartilage growth, growth hormone and IGF-I increase protein synthesis and lipolysis whilst decreasing insulin sensitivity and causing Na + retention.In addition to stimulating bone and cartilage growth, growth hormone and IGF-I increase protein synthesis and lipolysis whilst decreasing insulin sensitivity and causing Na + retention.

16
Pituitary Pathology Mostly arise from the anterior part of the gland The majority are benign adenomas 10–15% of intracranial neoplasms 75% of them secrete inappropriate amounts of pituitary hormones Malfunction of normal growth-regulating genes, abnormalities of tumour suppressor genes Prevalence: 200 per million of the population Post-mortem studies: 10–27%. The majority are therefore asymptomatic.

17
Presentation Hormonal hypersecretion syndromes hyperprolactinaemia, acromegaly and Cushing’s disease Mass effect visual disturbance or raised intracranial pressure Non-specific infertility, headache, epilepsy or pituitary hypofunction Incidental detected during imaging for other conditions

18
GH-secreting tumours Acromegaly in the adult and gigantism before epiphyseal closure Annual incidence of acromegaly is 6-8 cases per million Insidious in onset, characterized by enlargement of the jaw, hands and feet and increased soft tissue growth Associated complications of the disease diabetes mellitus and hypertension

21
Increase in size of skull and supraorbital ridges; enlarged lower jaw; increase in spacing between teeth/malocclusion Face Spade-shaped; carpal tunnel syndrome Hands and feet Macroglossia; thickened pharyngeal and laryngeal soft tissues; obstructive sleep apnoea Mouth/tongue Thick skin; doughlike feel to palmSoft tissue Vertebral enlargement; osteoporosis; kyphosisSkeleton Hypertension; cardiomegaly; impaired left ventricular functionCardiovascular Impaired glucose tolerance; diabetesEndocrine Arthropathy; proximal myopathyOther Clinical featuresAffected area Clinical features of acromegaly

22
GH-secreting tumours Preoperative diagnosis A random serum GH concentration of >10 mU litre –1 (5 ng ml –1 )A random serum GH concentration of >10 mU litre –1 (5 ng ml –1 ) Failure of suppression of GH concentrations to < 2 mU litre –1 (1 ng ml –1 ) following a 75 g oral glucose loadFailure of suppression of GH concentrations to < 2 mU litre –1 (1 ng ml –1 ) following a 75 g oral glucose load Elevated IGF-IElevated IGF-I Treatment The primary treatment is surgery, with or without subsequent radiotherapyThe primary treatment is surgery, with or without subsequent radiotherapy Dopamine agonistsDopamine agonists Long-acting analogues of somatostatin (such as octreotide)Long-acting analogues of somatostatin (such as octreotide)
A random serum GH concentration of >10 mU litre –1 (5 ng ml –1 ) Failure of suppression of GH concentrations to < 2 mU litre –1 (1 ng ml –1 ) following a 75 g oral glucose loadFailure of suppression of GH concentrations to < 2 mU litre –1 (1 ng ml –1 ) following a 75 g oral glucose load Elevated IGF-IElevated IGF-I Treatment The primary treatment is surgery, with or without subsequent radiotherapyThe primary treatment is surgery, with or without subsequent radiotherapy Dopamine agonistsDopamine agonists Long-acting analogues of somatostatin (such as octreotide)Long-acting analogues of somatostatin (such as octreotide)")
23
Preoperative Assessment Visual function Signs and symptoms of raised intracranial pressure Endocrine studies; and the effects of hormonal hypersecretion Co-morbidities, particularly in acromegaly or Cushing’s syndrome

24
Acromegaly 1. Anatomical changes prognathism and macroglossiaprognathism and macroglossia thickening of the pharyngeal and laryngeal soft tissues and vocal cordsthickening of the pharyngeal and laryngeal soft tissues and vocal cords reduction in the size of the laryngeal aperturereduction in the size of the laryngeal aperture hypertrophy of the periepiglottic foldshypertrophy of the periepiglottic folds recurrent laryngeal nerve palsyrecurrent laryngeal nerve palsy enlarged thyroid: 25%enlarged thyroid: 25%

25
Acromegaly 2. Sleep apnoea a rare complicating factor, but is associated with a high risk of perioperative airway compromisea rare complicating factor, but is associated with a high risk of perioperative airway compromise upper airway obstruction is the major cause, but central depression may also contributeupper airway obstruction is the major cause, but central depression may also contribute a history of loud snoring and daytime hypersomnolence should alert the anaesthetist to the possibility of sleep apnoeaa history of loud snoring and daytime hypersomnolence should alert the anaesthetist to the possibility of sleep apnoea

26
Acromegaly 3. Hypertension occurs in 30% of patients, but usually responds to therapyoccurs in 30% of patients, but usually responds to therapy myocardial hypertrophy and interstitial fibrosis are common and may be associated with reduced left ventricular functionmyocardial hypertrophy and interstitial fibrosis are common and may be associated with reduced left ventricular function 4.Glucose intolerance diabetes: 25%diabetes: 25%

27
Surgical Approach The pituitary fossa can be approached using the transsphenoidal, transethmoidal or transcranial route The transsphenoidal route is preferred for all but the largest of tumours Transsphenoidal access to the pituitary fossa is obtained using a sublabial or endonasal approach

28
Anesthetic Management 1. Hormone replacement Preoperative hormone replacement therapy should be continued into the operative period In general, hydrocortisone 100 mg should be administered at induction of anaesthesia in all patients undergoing pituitary surgery

29
Anesthetic Management 2. Airway management Four grades of airway involvement: grade 1-- no significant involvementgrade 1-- no significant involvement grade 2-- nasal and pharyngeal mucosa hypertrophy but normal cords and glottisgrade 2-- nasal and pharyngeal mucosa hypertrophy but normal cords and glottis grade 3-- glottic involvement including glottic stenosis or vocal cord paresisgrade 3-- glottic involvement including glottic stenosis or vocal cord paresis grade 4-- combination of grades 2 and 3, i.e. glottic and soft tissue abnormalitiesgrade 4-- combination of grades 2 and 3, i.e. glottic and soft tissue abnormalities

30
2. Airway management airway management and tracheal intubation proceed uneventfully in the majority of patients if large face masks and long-bladed laryngoscopes are used fibreoptic intubation should be considered in patients in whom difficult airway management is predicted intubating laryngeal mask airway has also been used successfully Equipment for tracheostomy should be available if airway changes are advanced (recommended for grades 3 and 4)
.")
31
2. Airway management the mouth and posterior pharynx should be packed before surgery begins prevent bleeding into the glottic region during surgery, but also entry of blood and secretions into the stomach which may precipitate postoperative vomiting

32
Anesthetic Management 3. Maintenance of anaesthesia short-acting agents are used to allow rapid recovery at the end of surgery During transsphenoidal surgery, ventilation to normocapnia should be employed. (Excessive hyperventilation will result in loss of brain bulk and make any suprasellar extension of the tumour less accessible from below) longer-acting opioids are administered before the end of surgery so that patients do not awaken in pain (IV morphine or IM codeine 20–30 min before the end of surgery)
 longer-acting opioids are administered before the end of surgery so that patients do not awaken in pain (IV morphine or IM codeine 20–30 min before the end of surgery).")
33
Anesthetic Management 4. Operative complications surgeon loses the anatomical landmarks of the fossa during transsphenoidal surgery. Deviation laterally may result in carotid damage. risk of development of a false aneurysm in the postoperative period If misses the fossa altogether, damage to the pons may occur

34
Anesthetic Management 4. Emergence from anaesthesia Smooth and rapid emergence from anaesthesia is essential to allow early neurological assessment and maintenance of stable respiratory and cardiovascular variables. use of short-acting agents for maintenance of anaesthesia

35
Postoperative Care Airway management Postoperative analgesia Hormone replacement Postoperative hormone complications

36
學習心得 … 此類病人 air way 之 management, 雖然 case 很少 … 此類病人 air way 之 management, 雖然 case 很少 … Keep in mind: endocrine abnormalities 所造成 的 co-morbidities.Keep in mind: endocrine abnormalities 所造成 的 co-morbidities. Awakening management after neurosurgery…Awakening management after neurosurgery…

37
Have A Nice Day

Similar presentations








 Hypothalamic control hGH releasing hormone hGH.>")












>")




