Download presentation
Presentation is loading. Please wait.

1
Transsphenoidal Pituitary Tumors
Dr. Shahrokh Yousefzadeh Chabok 27 Nov 2014

2
Neurosurgery has changed !
ESBS 2007

3
Evolution of Skull base Neurosurgery
Early 20th Century Harvey Cushing( ) Walter Dandy ( ) Hertbert Olivecrona( ) Charles Frazier( )
 Walter Dandy ( ) Hertbert Olivecrona( ) Charles Frazier( )")
4
Evolution of Skull Base Surgery
Contemporary Skull Base Surgery Al-Mefty Dolenc Jannetta Rhoton Samii Sen Sekhar Spetzler Yasargil many more !

5
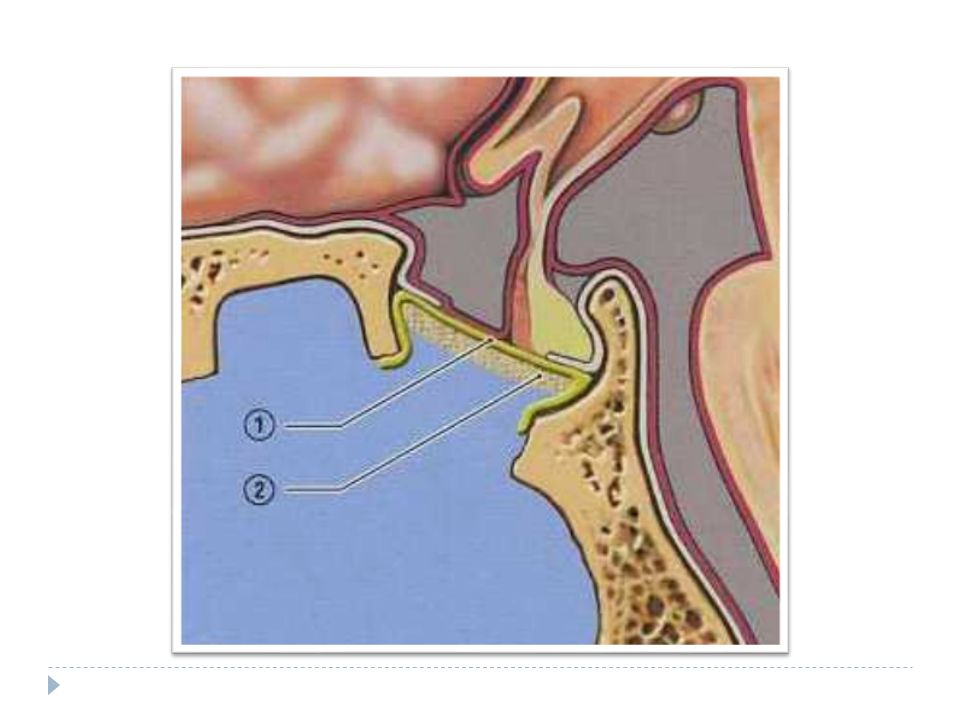
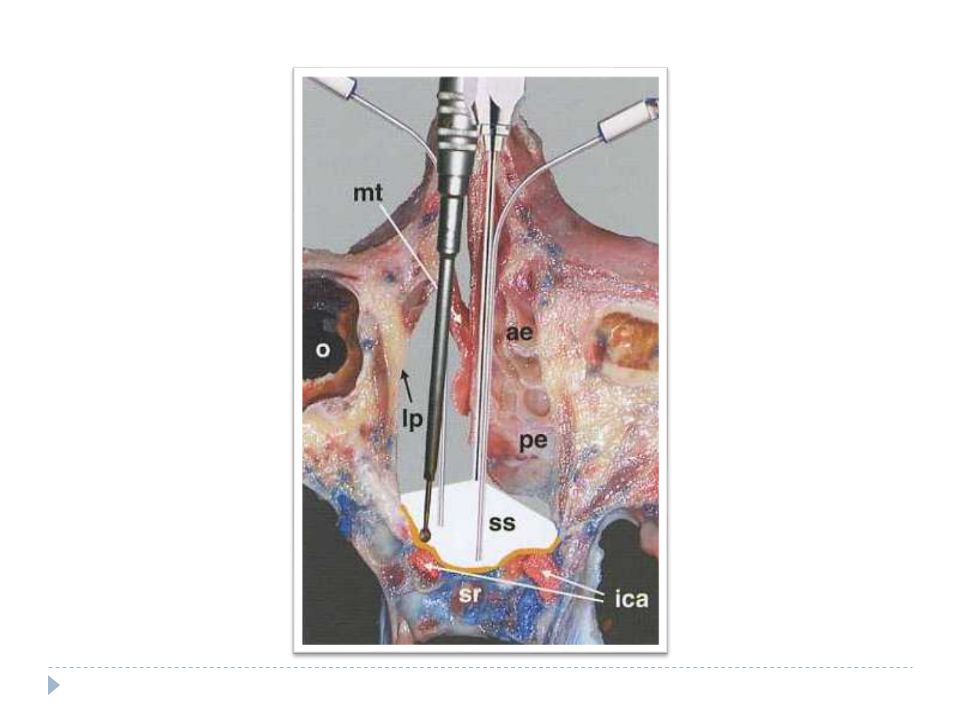
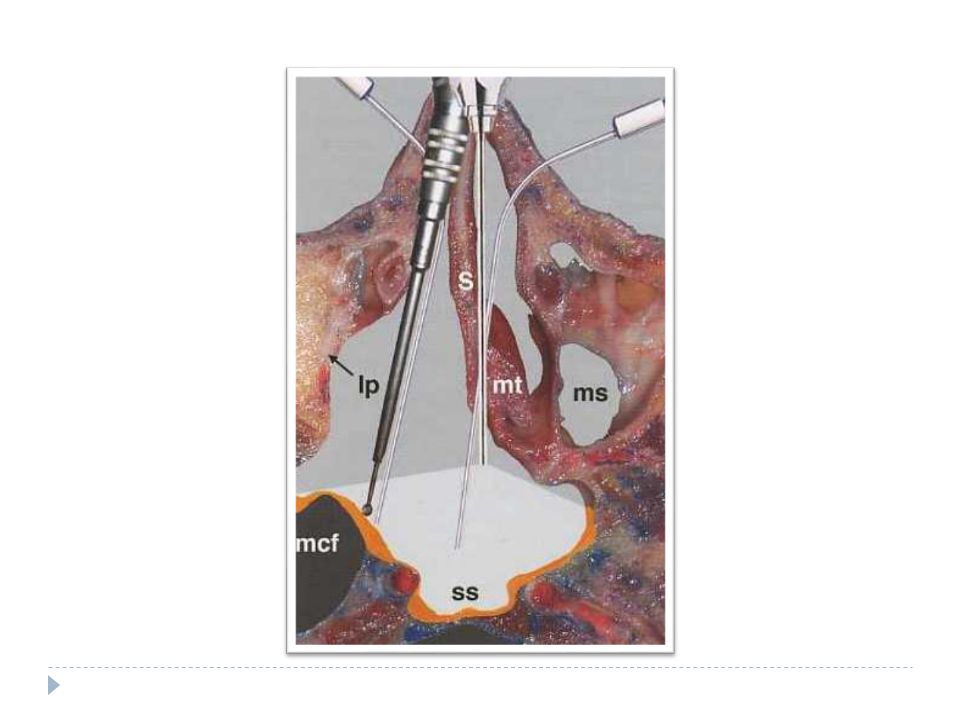
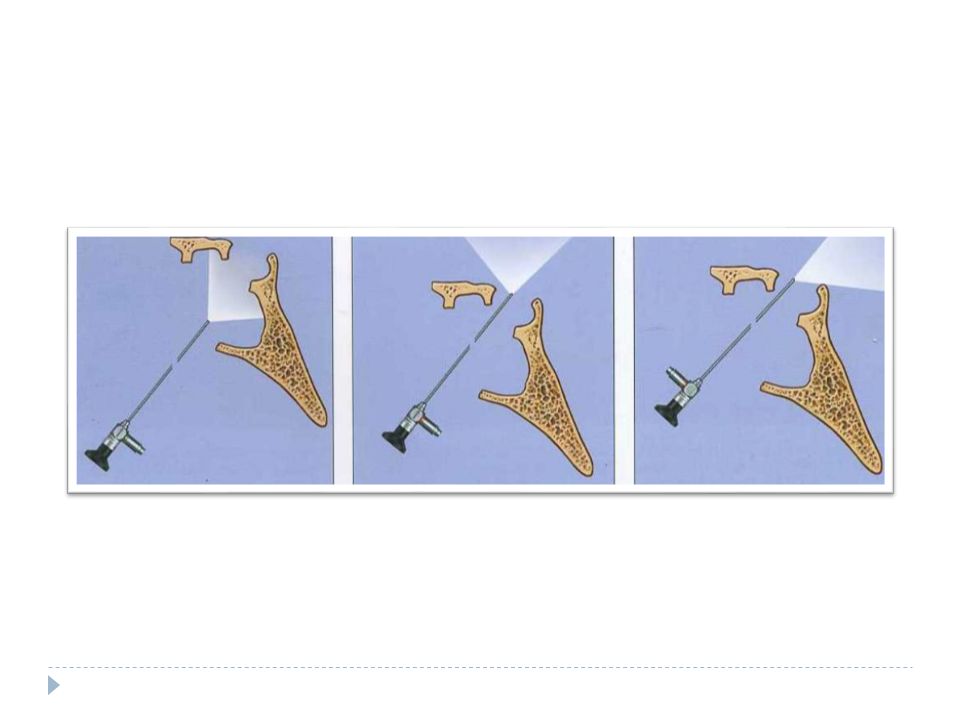
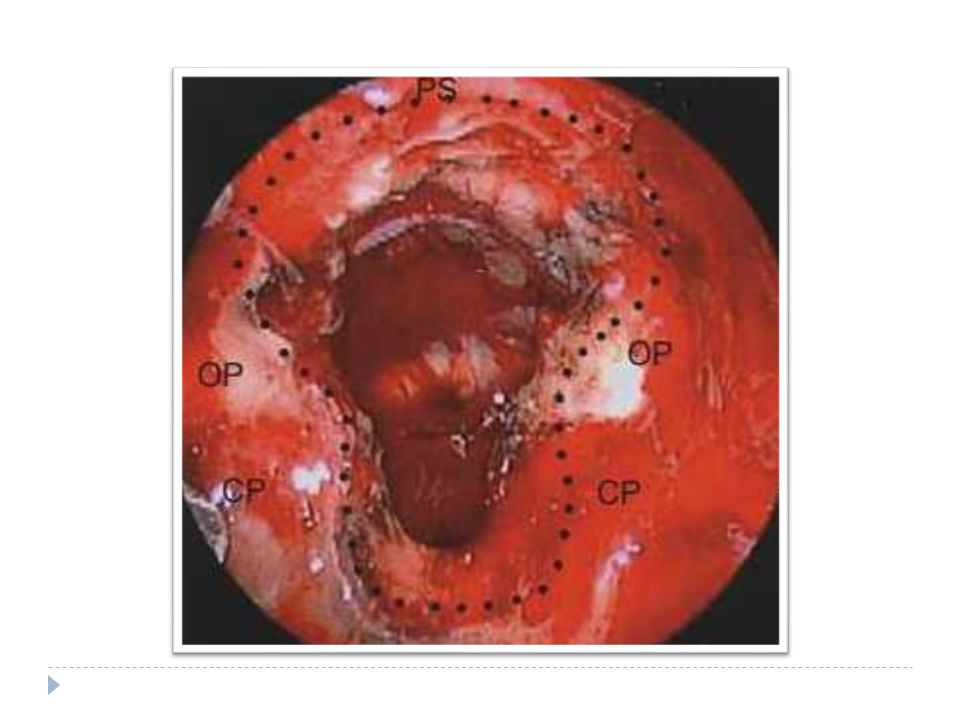
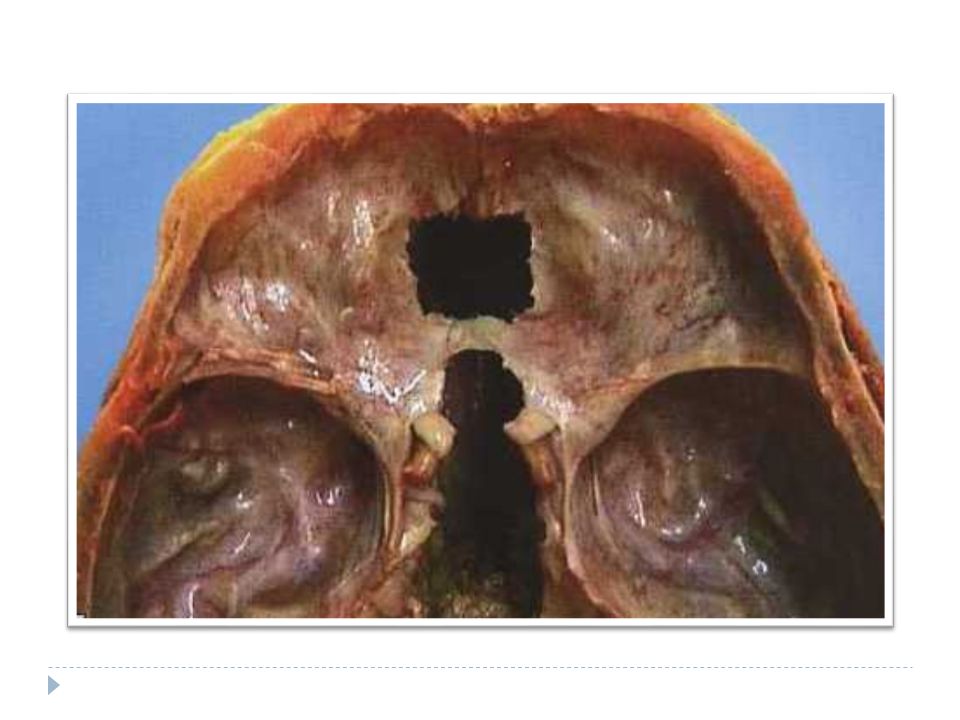
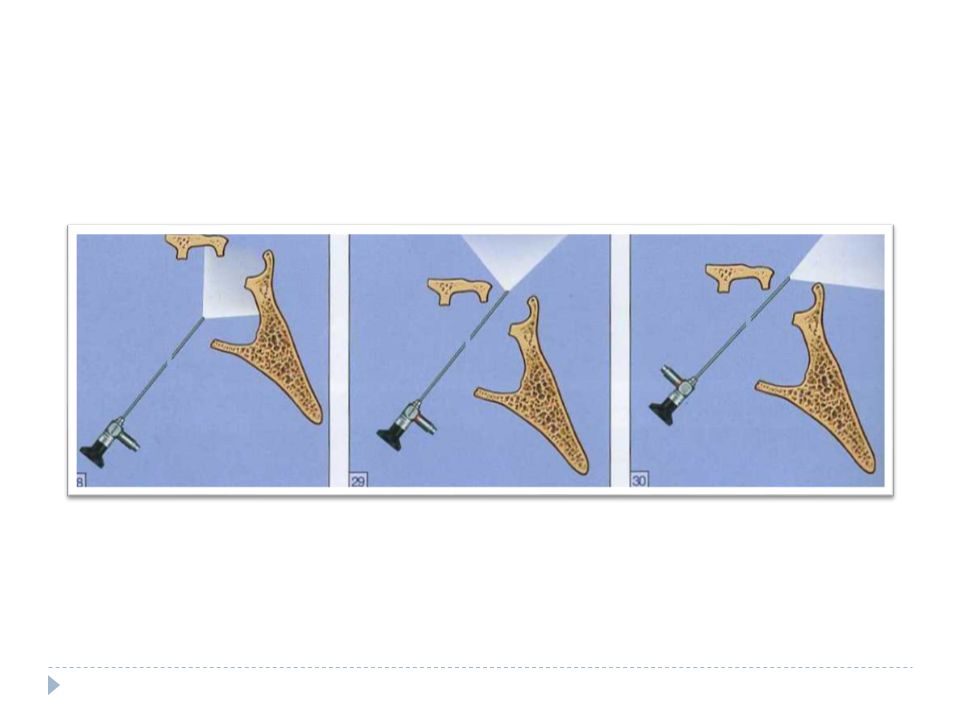
Quantification of exposure with endoscopic and microscopic approach to sellar- and supra sellar region

6
Quantification of exposure with endoscopic and microscopic approach to sellar- and supra sellar region

7
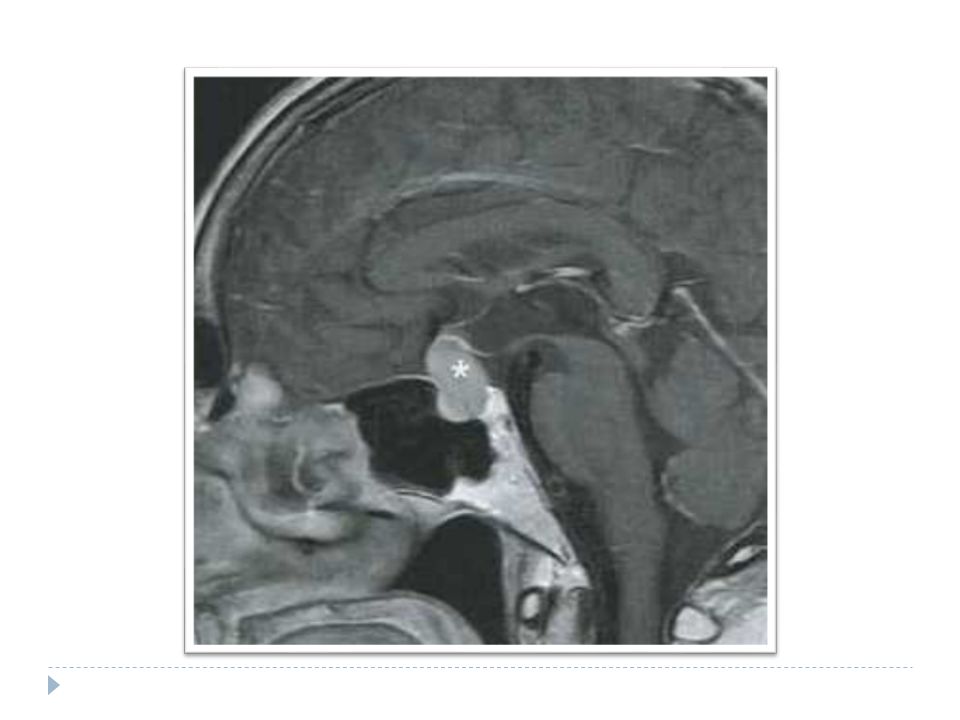
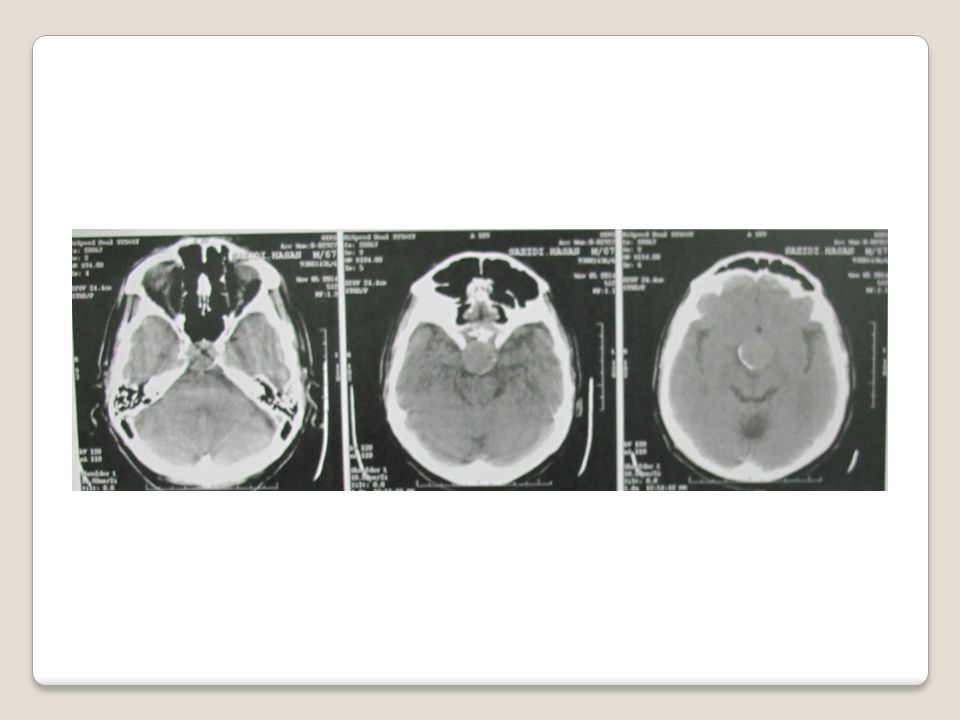
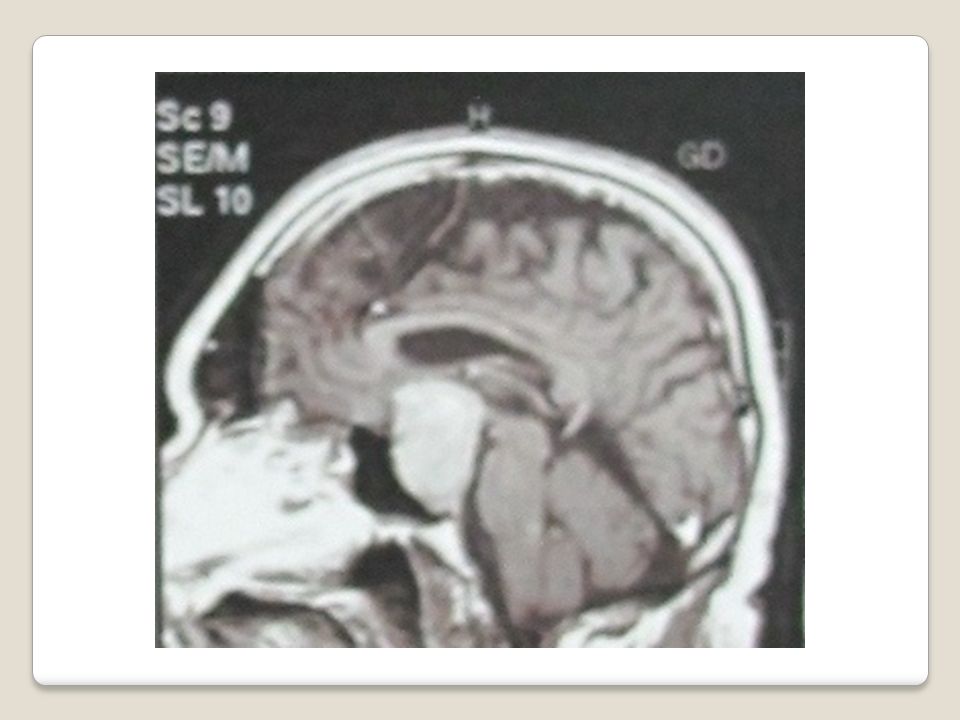
Pituitary Adenoma

8
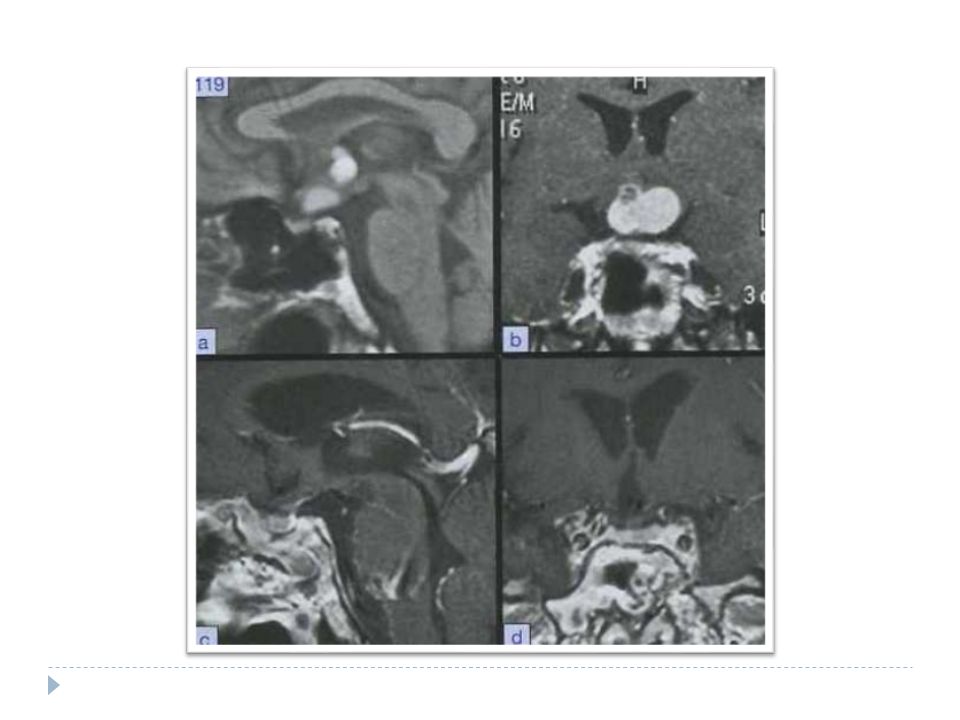
Evaluation MRI Visual field assessment Endocrine evaluation
Tests of normal gonadal, thyroid, and adrenal function Radioimmunoassays – for hormone levels

9
Classifying Imaging/surgical classification
Clinical/endocrine – functional vs. nonfunctional Pathological classification WHO classification – reconciles the three systems above

10
Pathologic Classification
Benign or malignant Chromophobic - Non-functioning Basophilic - Cushing’s Acidophilic - Acromegaly Mixed

11
Natural History Pituitary adenomas have long natural history
Vary in size and direction of spread Microadenomas < 10 mm – may cause focal bulging Macroadenomas > 10 mm – cause problems due to mass effect

12
Classification Microadenomas – Grades 0 and I
Macroadenomas – Grades II to IV Grade 0: Intrapituitary microadenoma with normal sellar appearance Grade I: Nml-sized sella with asymmetric floor Grade II: Enlarged sella with an intact floor Grade III: Localized erosion of sellar floor Grade IV: Diffuse destruction of floor

13
Classification Type A: Tumor bulges into the chiasmatic cistern
Type B: Tumor reaches the floor of the 3rd ventricle Type C: Tumor is more voluminous with extension into the 3rd ventricle up to the foramen of Monro Type D: Tumor extends into temporal or frontal fossa

14
WHO Classification Five-tiered system
Clinical presentation and secretory activity Size and invasiveness (e.g. Hardy) Histology (typical vs. atypical) Immunohistologic profile Ultrasturctural subtype
 Histology (typical vs. atypical) Immunohistologic profile. Ultrasturctural subtype.")
15
Goal of treatment Reversing endocrinopathy and restoring normal pituitary Function. Eliminating mass effect and restoring normal neurological Function. Eliminating or minimizing the possibility of tumor recurrence. Obtaining a definitive histologic diagnosis.

16
Normal histology white and firmness paucicellular and acinar pattern with pleomorphism
Histopathology yellow - gray or purple soft fluid to creamy texture Hypocellularity, monomorphism, uniform cytoplasm staining.

17
Surgical Indication Apoplasy Progressive mass effect (PRL , PRL )
Hyper functioning of P.T Unresponsive prolactinoma Histologic confirmation

18
Surgical contraindication
Profound hypopituitarism Active sinus infection Ectatic and tortuous carotid

19
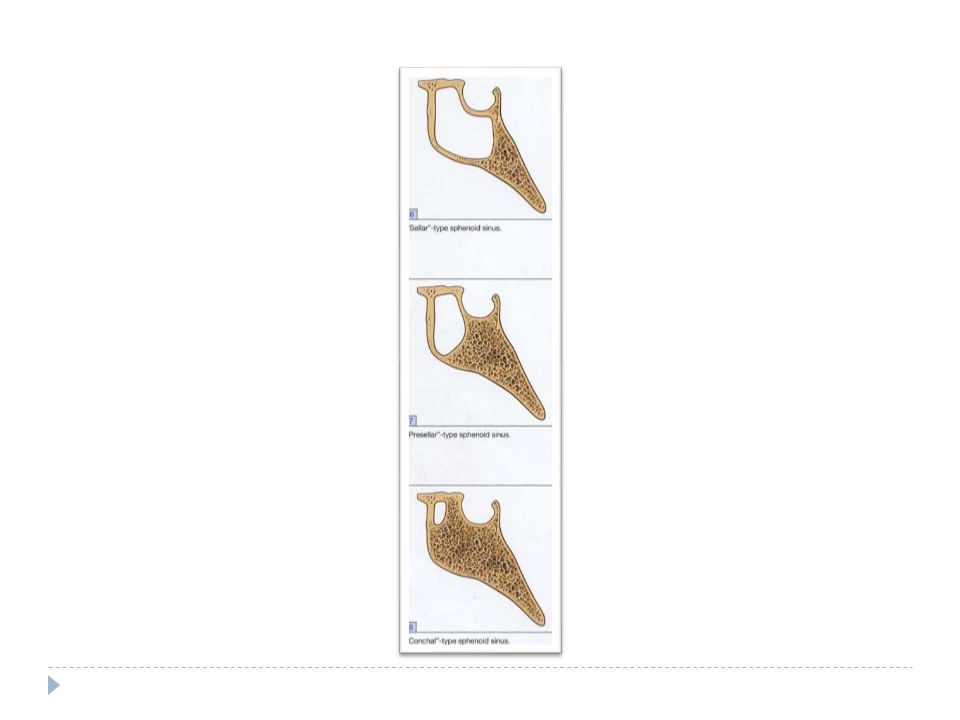
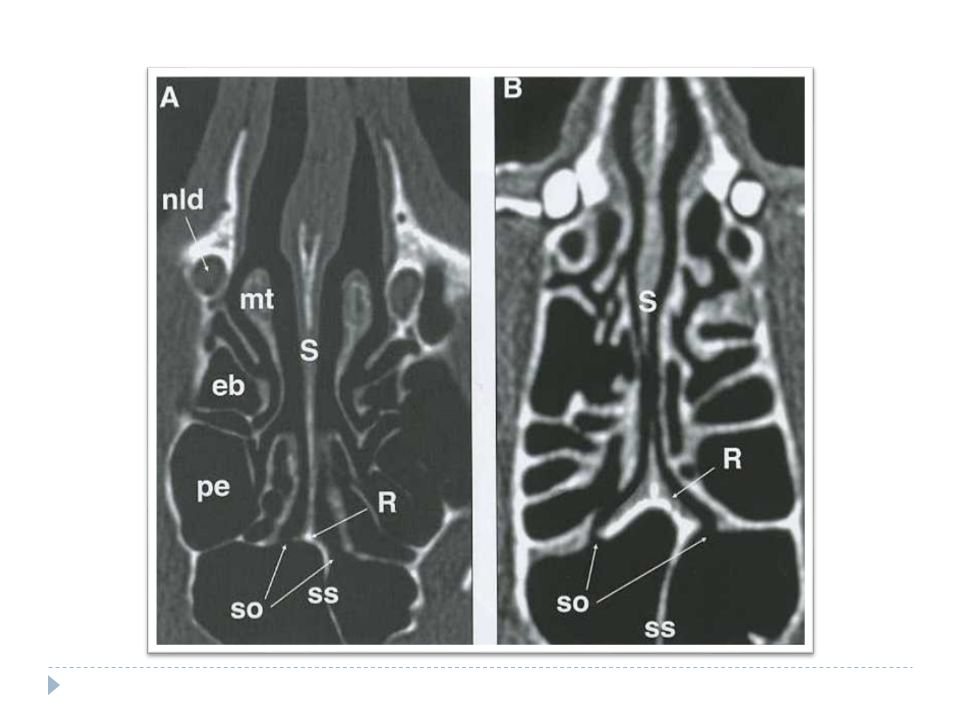
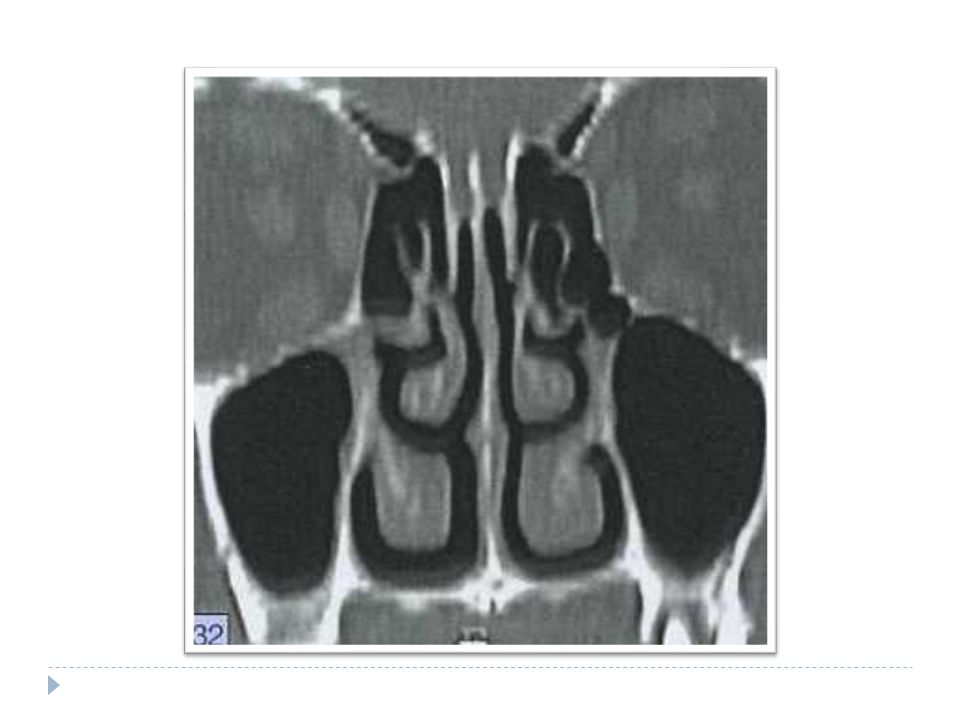
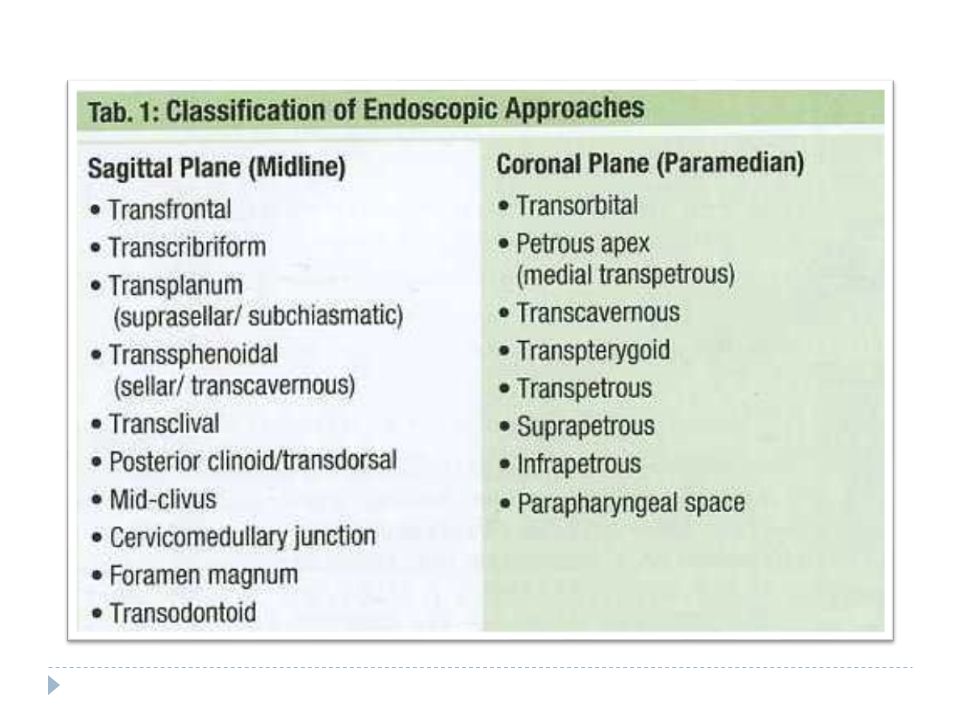
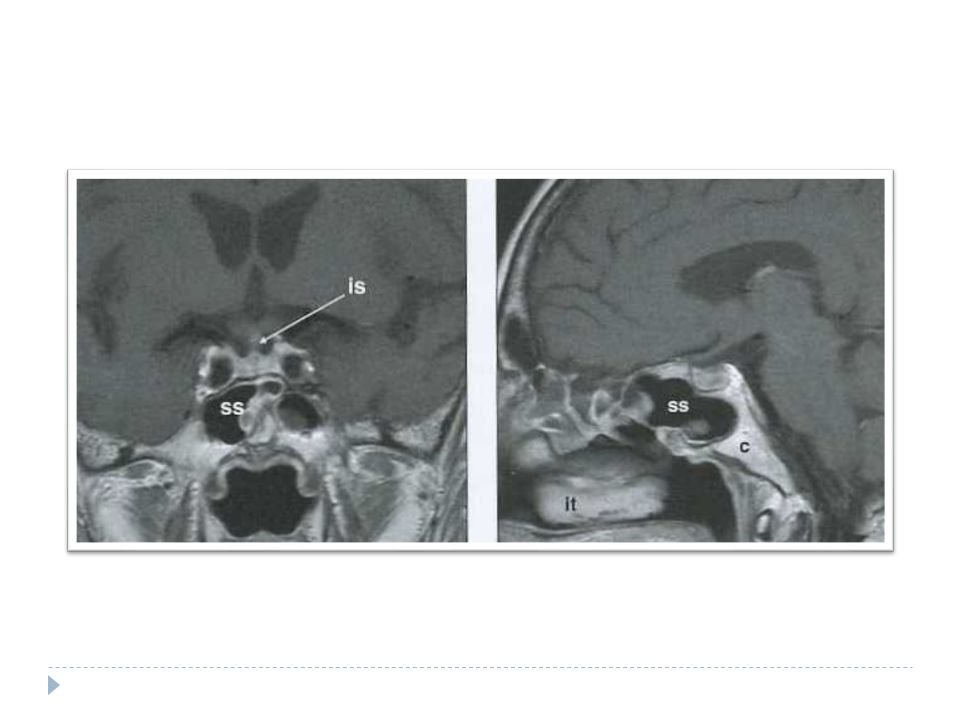
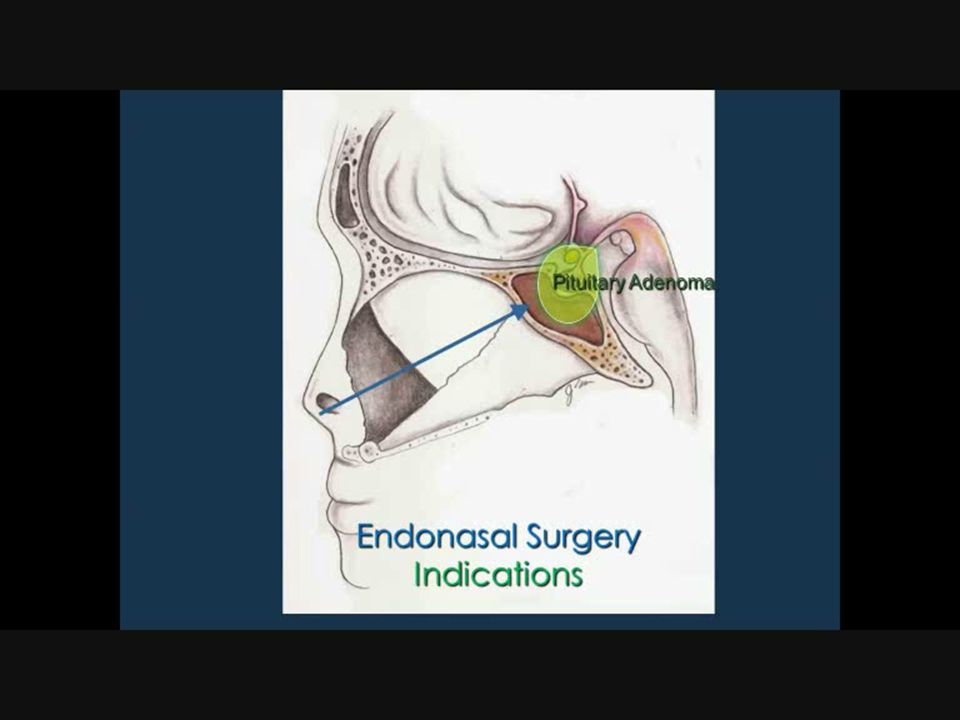
Choice of Surgical approach
Size of sella Size of pneumatization of SS Position and tortuous of carotid Direction of intracranial tumor extension uncertainly about pathology Prior therapy

20
Complication cavernous sinus injury iatrogenic hypopituitarism
Hypothalamic injury Visual damage Vascular complication Brain stem injury CSF leaks Nasal complication

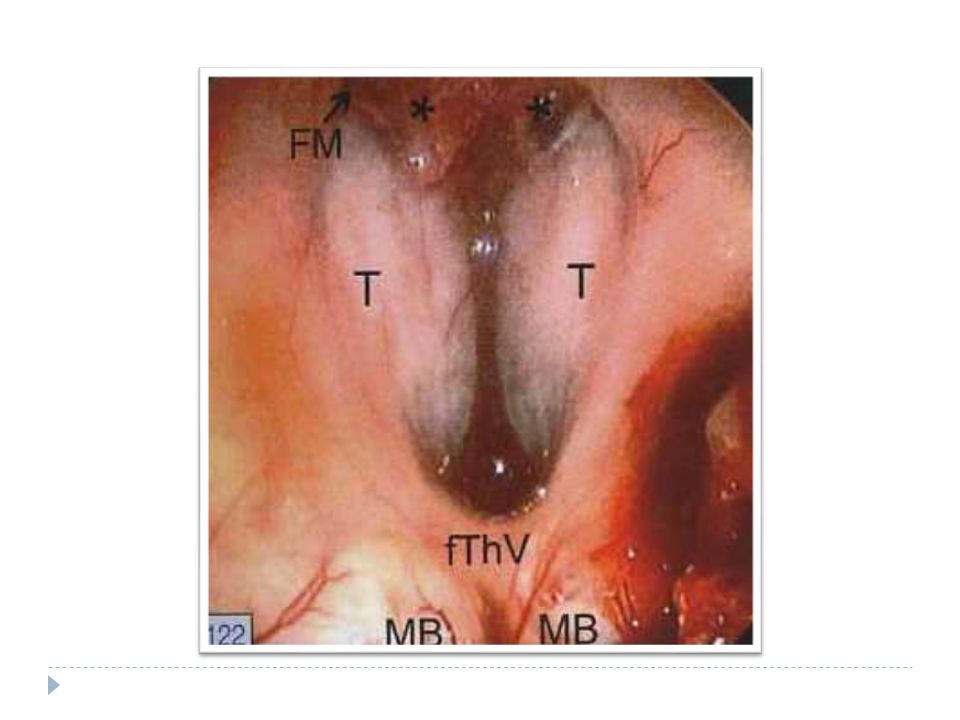
24
Pituitary Adenoma Endonasal Sublabial

25
Mile stone of modern and contemporary neurosurgery in the treatment of pituitary tumors

26
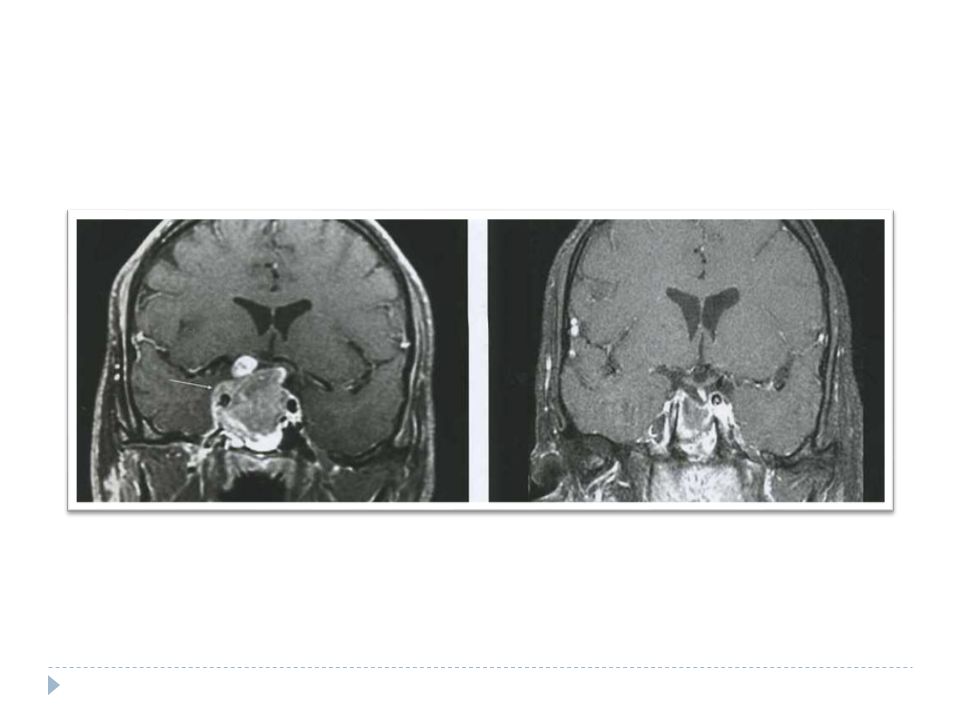
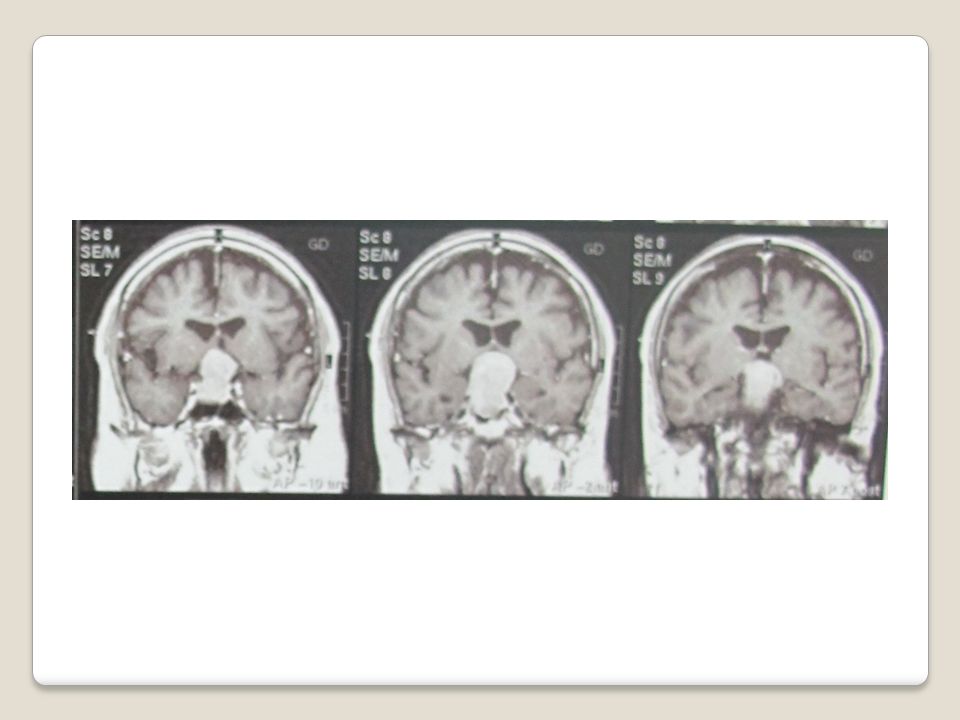
Pituitary Adenoma

42
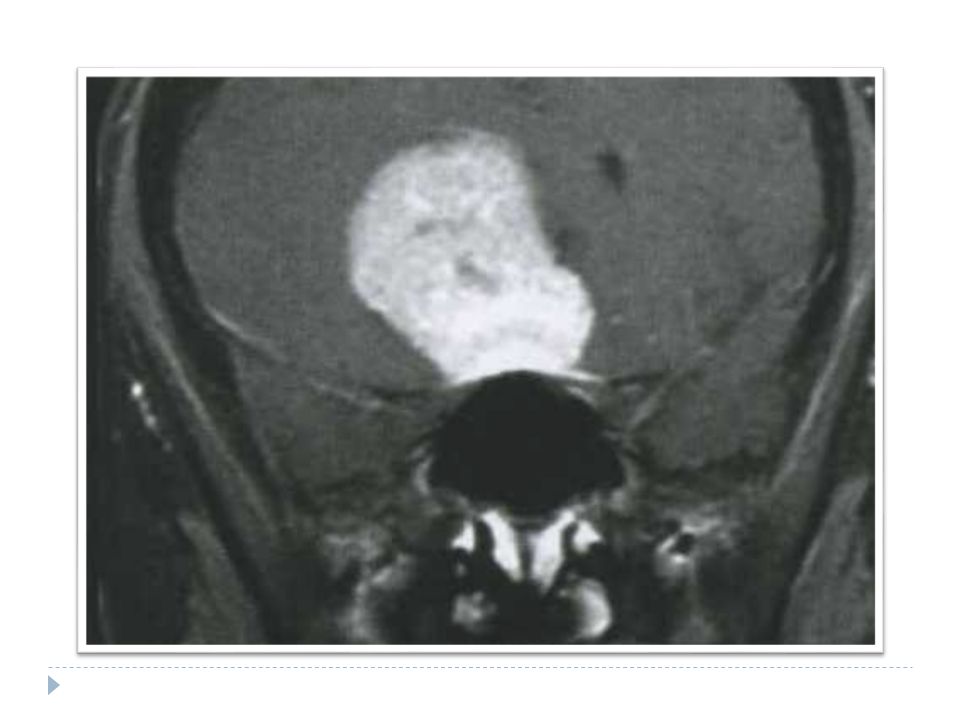
Pituitary Adenoma

43
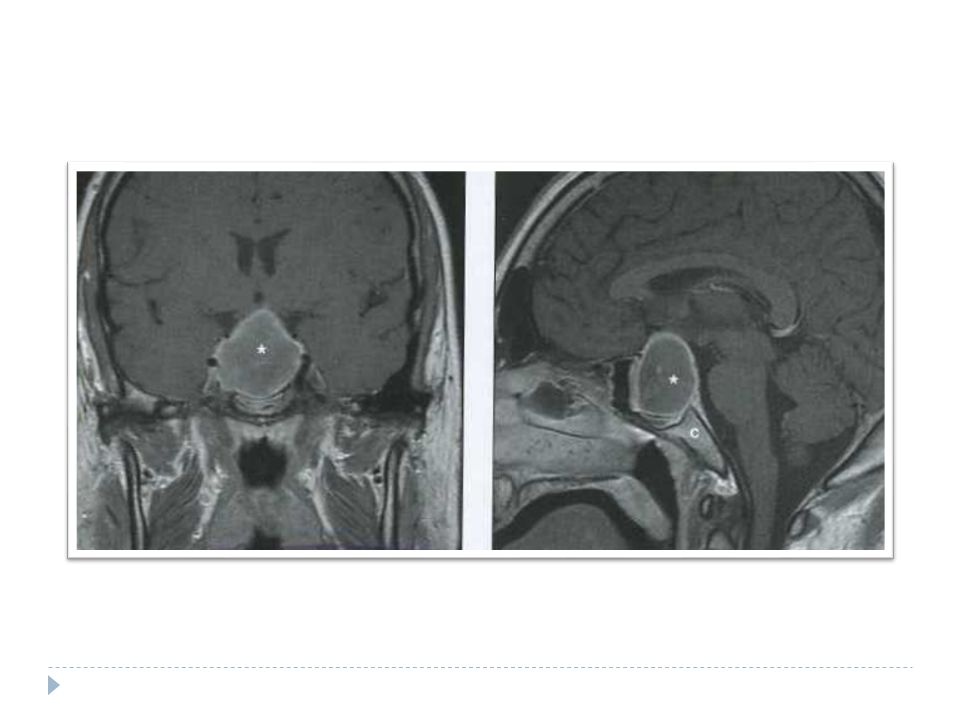
Pituitary Adenoma

46
Pituitary Adenoma

67
Appropriate for GKS

Similar presentations






























>")

