Download presentation
Presentation is loading. Please wait.

1
Pediatric Skin Disorders
There are disorders that occur to children at particular ages related to the growth and development process and the immaturity of the anatomical and physiological aspects of the child’s body. Nurse play an important role in public education and prevention.

2
Compare skin differences
Infant: skin not mature at birth Adolescence: sebaceous glands become enlarged & active. Infant- less effective barrier to physical elements & microorganisms thinner & more sensitive Adolescence- They produce sebum in response to hormones ...predisposing to acne.

3
Skin Assessment Assess history Assess exposure Assess character
Assess sensation Assess history of allergies, exposure to any irritants- chemicals, animals, medication, etc Assess exposure to other people with similar complaints Assess character for color, size, shape, distribution & lesion (macule, papule, bulla, etc) Assess description of sensation- how it feels, if painful, pruritis
 Assess description of sensation- how it feels, if painful, pruritis.")
4
Dermatitis Atopic/Eczema- worsens progressively, begins in early infancy genetic history of tendency for dry, sensitive skin, allergy and emotional stress. Family hx of asthma, hay fever, or atopic dermatitis. **Controversial role of immunoglobulin E ((IgE)- medicated food allergy has been shown to exacerbate condition in some children. Contact Dermatitis- self limiting with removal of irritant and treatment with topical steroidal creams/ointments
- medicated food allergy has been shown to exacerbate condition in some children. Contact Dermatitis- self limiting with removal of irritant and treatment with topical steroidal creams/ointments.")
5
Dermatitis Inflammation of the skin that occurs in response to contact with an allergen or irritant; also referred to as “contact dermatitis” Self limiting with removal of irritant and treatment with topical stseroidal creams/ointments

6
Dermatitis Common irritants:
Soap, fabric softeners, lotions, urine and stool ♦ Common allergens poison ivy, poison oak lanolin, latex, rubber nickel, fragrances

7
Dermatitis: signs and symptoms
Erythema Edema Pruritus Vesicles or bullae that rupture, ooze and crust

8
Dermatitis: Treatment
Medications Application of a corticosteroid topical agent: remind pt to continue use for 2-3 wks after signs of healing Application of protective barrier ointments Oatmeal baths, cool compresses Antihistamines given for sedative effect With children, clip fingernails….can lead to bacterial infections if they scratch

9
Eczema Chronic superficial skin disorder characterized by intense pruritis

10
Eczema: signs and symptoms
Erythematous patches with vesicles Pruritis Exudate and crusts Drying and scaling Lichenification (thickening of the skin)
")
11
Eczema, cont.

12
Goal of Treatment Hydrate the skin

13
Treatment of Eczema Emollients (creams which lubricate the skin)
Oral antihistamines (control itching) Antibiotics (treat superinfections) Corticosteroids (anti-inflammatories) Immunomodulators (inhibit T lymphocyte activation) AVOID SOAPS!
 Antibiotics (treat superinfections) Corticosteroids (anti-inflammatories) Immunomodulators (inhibit T lymphocyte activation) AVOID SOAPS!")
14
Acne Inflammatory disease of the skin, involving the sebaceous glands and hair follicles. Contributing factors include: heredity, hormonal influences, and emotional stress (what a teenager eats may have little effect on the complexion) Unrelated to cleanliness
 Unrelated to cleanliness.")
15
Acne Inflammatory disease of the skin involving the sebaceous glands and hair follicles. Contributing factors include: heredity, hormonal influences and emotional stress

16
Acne: Three main types Follicular plugs Pustular papules
Cystic nodules

17
Patient teaching Do not pick! This increases the bacterial count on the surface of the skin and opens lesions to infection which worsens scarring Remind patients that the treatment will not show improvement until about 4-6 weeks but they must consistently follow the regime set up by the physician

18
Medical treatment for acne
Topical (Benzoyl peroxide, Tretinoin (RetinA), topical preferred to systemic; however, both may be needed Oral: Tetracycline, minocycline, erythromycin; estrogen for female pts., Accutane SE of Accutane: liver toxicity, teratogen; nosebleeds and depression.
, topical preferred to systemic; however, both may be needed. Oral: Tetracycline, minocycline, erythromycin; estrogen for female pts., Accutane. SE of Accutane: liver toxicity, teratogen; nosebleeds and depression.")
19
Acne: Nursing care Avoid picking and squeezing
Use gentle skin cleansers Avoid use of astringents containing ETOH Avoid hats or abrasive rubbing of the skin Wash hands after handling greasy foods Limit use of petrolatum-based hair products; hair away from face Use oil-free makeup, protections from windy, cold weather Continue therapy even when improved

20
Impetigo Hemolytic Strep infection of the skin
Impetigo became infected Hemolytic Strep infection of the skin Incubation period is 2-5 days after contact Strep infection of the skin- Test question

21
Begins as a reddish macular rash, commonly seen on face/extremities
Progresses to papular and vesicular rash that oozes and forms a moist, honey colored crust. Pruritis of skin Common in 2-5 year age group Spreads from one lesion to another; requires abx to treat

22
Therapeutic Management
Apply moist soaks of Burrow’s solution Antibiotic therapy: Keflex for 10 days Patient education Burrow’s solution is aluminum acetate used as a drying agent for weeping skin lesions- to soften lesions, remove crusts, cover to prevent spread by itching CUT FINGERNAILS Topical antibiotic therapy TID Bactroban, Baciguent, Neosporin Oral (systemic)- Cephalexin (Keflex) Erythromycin, Dicloxacillin ** Make sure the pt takes the entire regime of antibiotics– complication of impetigo and strep infections is glomerulonephritis Teach thorough hand washing to patient and family (antibacterial soap), trim nails, wear gloves when treating the wounds, Teach family that child should not share towels, combs, eating utensils. Wash clothes and linens in machine using soap and hot water Teach about transmission- wound to skin, protect immuno-compromised individuals.
- Cephalexin (Keflex) Erythromycin, Dicloxacillin ** Make sure the pt takes the entire regime of antibiotics– complication of impetigo and strep infections is glomerulonephritis. Teach thorough hand washing to patient and family (antibacterial soap), trim nails, wear gloves when treating the wounds, Teach family that child should not share towels, combs, eating utensils. Wash clothes and linens in machine using soap and hot water. Teach about transmission- wound to skin, protect immuno-compromised individuals.")
23
Therapeutic Interventions for impetigo
Goal: prevent scarring and promote + self image. Individualize treatment to gender, age, and severity of infection Takes 4-6 wks to improve What is the major nursing implication here? To prevent spread of the lesions

24
Candiditis- Thrush Overgrowth of Candida albicans
Acquired through delivery Candiditis is an overgrowth of the Candida albicans fungus- also known as Thrush or a yeast infection Usually occurs during delivery when the NB passes through an infected vagina- candida is a common fungus found on the skin and is easily transmitted

25
Thrush Characterized by white patches in the mouth, gums, or tongue
Treated with oral Nystatin suspension: swish and swallow May present as white film over tongue, or curd-like plaques on the tongue, gums, and buccal mucosa Tell them apart from milk curds because they are difficult to remove (also may have foul breath- very unusual in an infant) NB or child may have difficulty in eating (mouth hurts) or throat may be sore. Diaper area– Candiditis dermatitis- will present as a bright read rash in the diaper area and may progress to the abdomen--- usually follows oral antibiotic therapy WHY?- antibiotics kill the normal flora and allow the yeast to take over Diagnosis is upon assessment- may require a culture- but is so common that simple observation of the S&S is enough.
 NB or child may have difficulty in eating (mouth hurts) or throat may be sore. Diaper area– Candiditis dermatitis- will present as a bright read rash in the diaper area and may progress to the abdomen--- usually follows oral antibiotic therapy WHY - antibiotics kill the normal flora and allow the yeast to take over. Diagnosis is upon assessment- may require a culture- but is so common that simple observation of the S&S is enough.")
26
Dermatophytosis (Ringworm)
Tinea Capitis fungal infection known as “ringworm” Transmission: Person-to-person Animal-to-person Tinea Capitis- fungal infection of the stratum corneum, nails and hair (at the base of the hair, the hair may break off , usually grows back) Why do cats have such a bad rep for spreading ring worm? Cats can get ringworm, they also dig in the moist soil and climb trees that may have the fungus. Sand boxes in playgrounds are one of the most common sources of infection
 Why do cats have such a bad rep for spreading ring worm Cats can get ringworm, they also dig in the moist soil and climb trees that may have the fungus. Sand boxes in playgrounds are one of the most common sources of infection.")
27
S&S: Scaly, circumscribed patches to patchy, gray scaling areas of alopecia. Pruritic Generally asymptomatic, but severe, deep inflammatory reaction may appear as boggy, encrusted lesions (kerions) Scaly, circumscribed patches to patchy, gray scaling areas of alopecia. Pruritic Generally asymptomatic, but severe, deep inflammatory reaction may appear as boggy, encrusted lesions (kerions)
 Scaly, circumscribed patches to patchy, gray scaling areas of alopecia. Pruritic. Generally asymptomatic, but severe, deep inflammatory reaction may appear as boggy, encrusted lesions (kerions)")
29
Clinical manifestations
Fungal infection of the stratum corneum, nails and hair (the base of hair shaft causing hair to break off…rarely permanent) Scaly, patches Pruritis Generally asymptomatic, but severe reactions may appear as encrusted lesions
 Scaly, patches. Pruritis. Generally asymptomatic, but severe reactions may appear as encrusted lesions.")
30
Tinea: signs and symptoms

31
Therapeutic Interventions
Transmitted by clothing, bedding, combs and animals (cats especially) May take 1-3 months to heal completely, even with treatment Child doesn’t return to school until lesions dry
 May take 1-3 months to heal completely, even with treatment. Child doesn’t return to school until lesions dry.")
32
Diagnosis Potassium hydroxide examination Black Light
Potassium hydroxide examination- examine with microscope using potassium hydroxide to stain the fungus Black light causes fungus to glow-phosphoresce

33
Medication Therapy Antifungals: Oral griseofulvin (Lamisil)
Give with fatty foods to aid in absorption Treatment is 4-6 wks Can return to daycare when lesions are dry Oral- systemic treatment with oral griseofulvin (very bitter) Lamisil Antifungal-topical on lesions until healed (may take 3 months) Shampooing, short trimmed nails, hand washing, increase the effectiveness of treatment. Why is it best if the patient does not scratch??
 Lamisil. Antifungal-topical on lesions until healed (may take 3 months) Shampooing, short trimmed nails, hand washing, increase the effectiveness of treatment. Why is it best if the patient does not scratch")
34
Pediculosis Capitis (lice)
a parasitic skin disorder caused by lice the lice lay eggs which look like white flecks, attached firmly to base of the hair shaft, causing intense pruritus Lice require several meals of human blood daily, and will die if away from humans more than 2 days Most common in children 3-10 years of age Why? Transmission via direct contact with someone infested

35
Diagnosis Direct identification of egg (nits)
Direct identification of live insects Close examination of scalp reveals (nits) firmly attached to hair shafts Easily transmitted by clothing, towels, combs, close contact, unrelated to hygiene
 firmly attached to hair shafts. Easily transmitted by clothing, towels, combs, close contact, unrelated to hygiene.")
36
Pediculosis Here you can see the nits (eggs) as well as the lice
 as well as the lice")
37
Medication Therapy Treatment: shampoos RID, NIX, Kwell(or Lindane) shampoo: is applied to wet hair to form a lather and rubbed in for at least amount of time recommended, followed by combing with a fine-tooth comb to remove any remaining nits. Leave in place for 10 minutes and rise; towel dry; comb hair with a fine-ttoth comb to remove any remaining nits.
 shampoo: is applied to wet hair to form a lather and rubbed in for at least amount of time recommended, followed by combing with a fine-tooth comb to remove any remaining nits. Leave in place for 10 minutes and rise; towel dry; comb hair with a fine-ttoth comb to remove any remaining nits.")
38
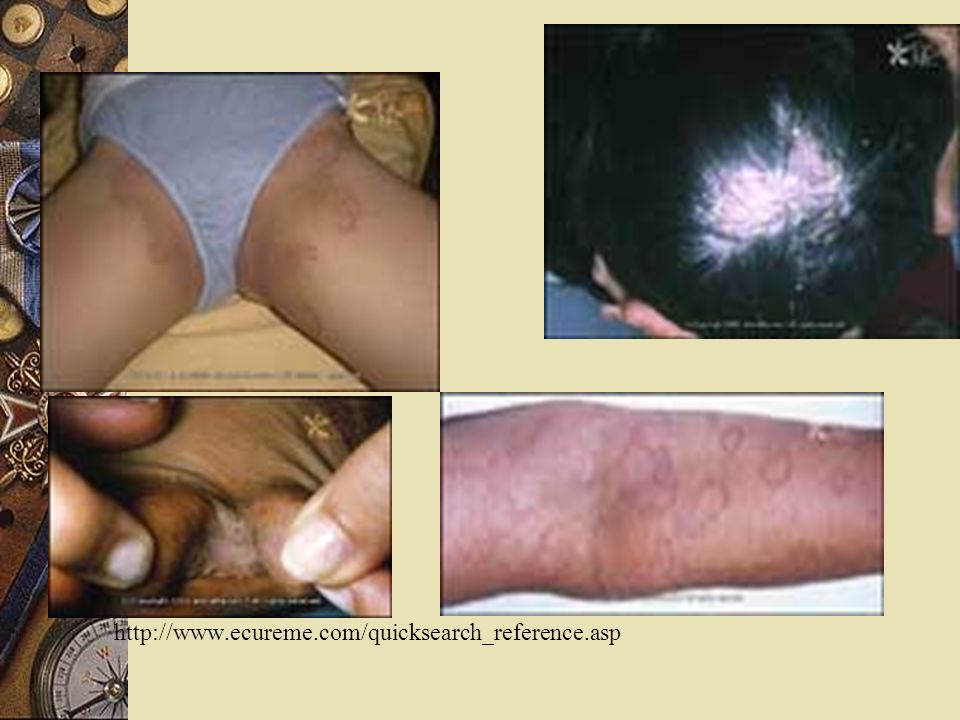
Scabies Sarcoptes scabei mite. Females are 0.3 to 0.4 mm long and 0.25 to 0.35 mm wide. Males are slightly more than half that size. A parasitic skin disorder (stratum corneum- not living tissue) caused by a female mite. The mite burrows into the skin depositing eggs and fecal material; between fingers, toes, palms, axillae pruritic & grayish-brown, thread-like lesion
 caused by a female mite. The mite burrows into the skin depositing eggs and fecal material; between fingers, toes, palms, axillae. pruritic & grayish-brown, thread-like lesion.")
39
Scabies between thumb and index finger
Scabies between thumb and index finger On foot

40
Therapeutic Interventions
transmitted by clothing, towels, close contact Diagnosis confirmed by demonstration from skin scrapings. treatment: application of scabicide cream which is left on for a specific number of hours (4 to 14)to kill mite rash and itch will continue until stratum corneum is replaced (2-3 weeks)
to kill mite. rash and itch will continue until stratum corneum is replaced (2-3 weeks)")
41
Care: Fresh laundered linen and underclothing should be used.
Contacts should be reduced until treatment is completed.

Similar presentations