Download presentation
Presentation is loading. Please wait.

1
FUNGAL SKIN INFECTIONS

2
Fungal skin Infections
The most common cutaneous infection Referred to as ring worm infections Usually superficial and can involve hair, nail, skin. Tinea capitis,tinea corporis, tinea pedis Three genera of fungi: Trichophyton, Microsporum and Epidermophyton Predisposing factors: Trauma to the skin: blisters Diabetes or immunocompromised patients Skin occlusion, high humid conditions Tinea pedis: Athlete’s foot: the most prevalent fungal infection More common in adults than in children, more in men than in women, Tinea corporis: common among children, hot and humid conditions, individuals under stress and overweight Tinea capitis: scalp is involved, common among children

3
Environmental factors play an important role
Epidemiology Trauma Environmental factors play an important role Chronic health problems and medications that weaken immune response Tinea pedis is the most common infection Etiology: three genera of pathogenic fungi: trichophyton, microsporum and epidermophyton Transmission: contact with infected people, fomites. Environmental factors Pathophysiology: Inoculation Incubation period: dermatophyte grows in SC, minimal signs of infection Infection is established: fungal growth rate vs epidermal growth rate Serum inhibitory factor inhibits further growth Dermatophyte starts secreting enzymes and keratinases and reach the viable epidermis Cell mediated immunity starts: inflammation and pruritis Signs and symptoms of infection Mild itching and scaling to severe exudative inflammatory process. Fissuring, crusting and discoloration of the skin

5
Tinea Pedis Four accepted variants are present Chronic intertriginous type: most common, fissuring , scaling, maceration in the interdigital space. Malodor, pruritis. Chronic papulosquamous: both feet, mild inflammation and diffuse scaling of the soles Vesicular type: small vesicles. Skin scaling may be seen Acute ulcerative type: macerated weeping ulceration on the sole. Hyperkeratosis and pungent odor Infection may trigger a bacterial overgrowth BE CAREFUL WHEN: Toe nail is involved, vesicular eruptions with ooszing, eczematous eruptions with blisters, diabetic patients

6
Tinea unguium: nails are infected
The gradually loose their shiny luster and become opaque If untreated, the nails become thick, yellowish and friable The nail may separate from the nail bed and may be lost

7
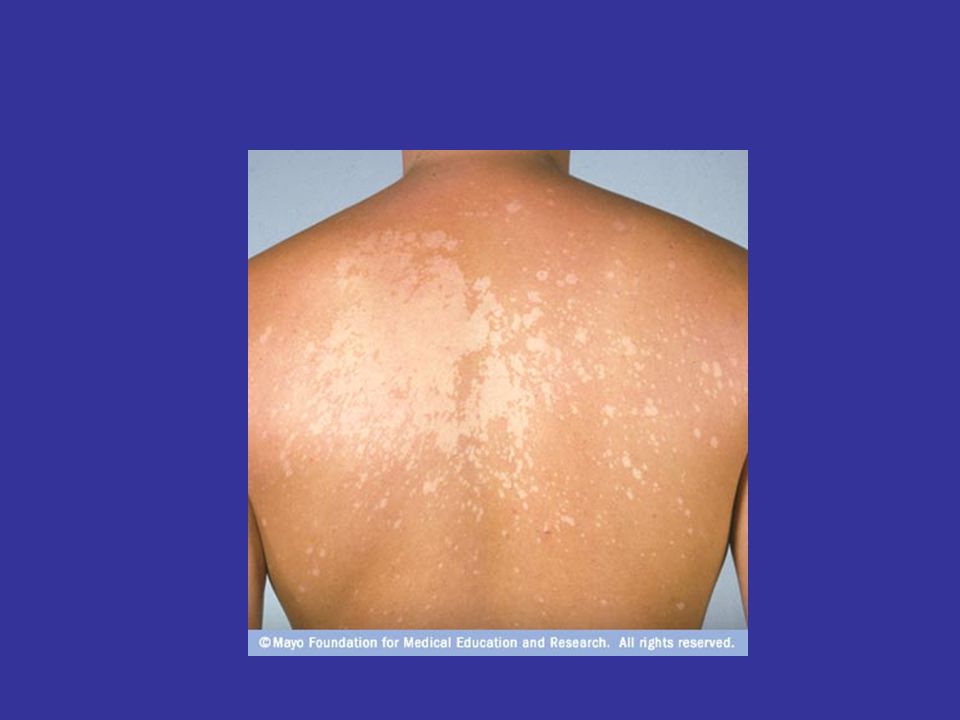
Tinea corporis: has diverse clinical presentation.
Lesions start as small circular erythematous scaly areas Spread peripherally and the borders may contain vesicles. Pruritis

9
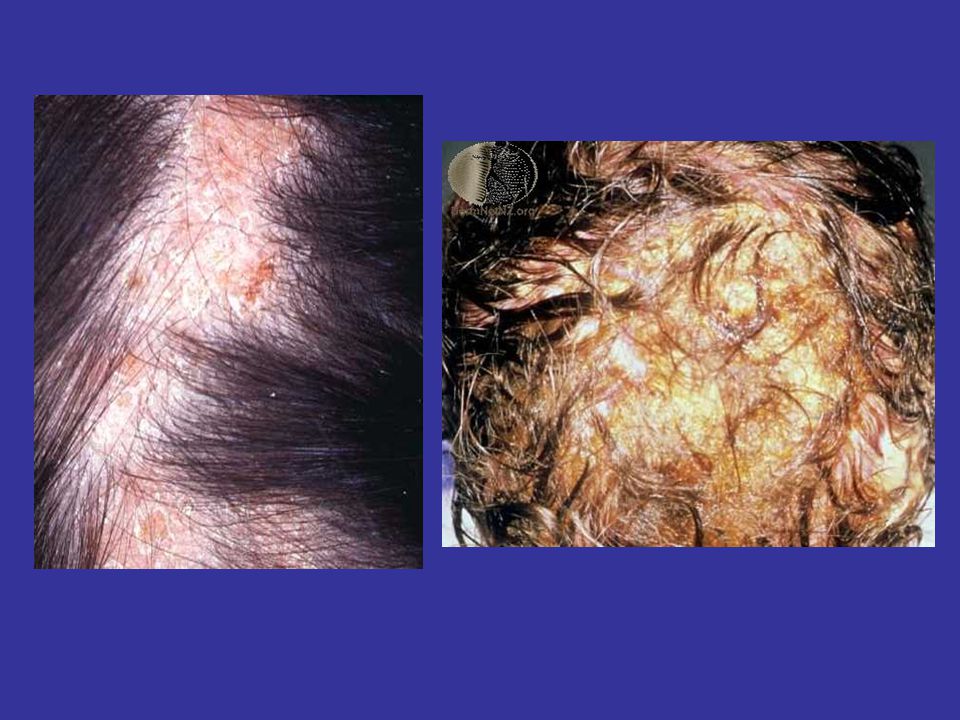
Tinea capitis: most prevalent between 3 - 7 years of age.
It is slightly more common in boys than girls. More common in crowded living conditions. The fungus can contaminate hairbrushes, clothing, towels and the backs of seats. The spores are long lived and can infect another individual months later. Tinea capitis may present in several ways. 1. Dry scaling – non inflammatory. Small papules surrounding the shafts, like dandruff but usually non inflammatory, spreads centrifugally, hair lesions are dull gray in color, hair breaks off the scalp 2. Inflammatory, pustules to kerions/ Kerion: weeping lesions, exudates, form thick crusts on the scalp. Pruritis, fever, pain, lymph nodes 3. Black dots - the hairs are broken off at the scalp surface, which is scaly Smooth areas of hair loss 4.Favus – patchy areas of hair loss, yellow crusts and matted hair Untreated kerion and favus may result in permanent scarring (bald areas).
.")
11
Treatment of fungal skin infections
Goals: provide symptomatic relief, eradicate the infection, prevent future infections Pharmacologic agents: antifungals, antiinflammatory agents, astringent salts for tinea pedis before therapy Patient compliance: 2-4 weeks for the infection to be eradicated Non pharmacologic measures: keep the skin dry and clean, avoid sharing personal articles Antifungals: Clioquinol 3%: pedis, corporis with hydrocortisone Clotrimazole, miconazole nitrate: pedis and corporis Terbinafine hydrochloride: 1% Tolnaftate Salts of aluminum: no direct antifungal effect, reduce iflammation, astringents, decrease edema, inflammation and irritation. Aluminum acetate and chloride

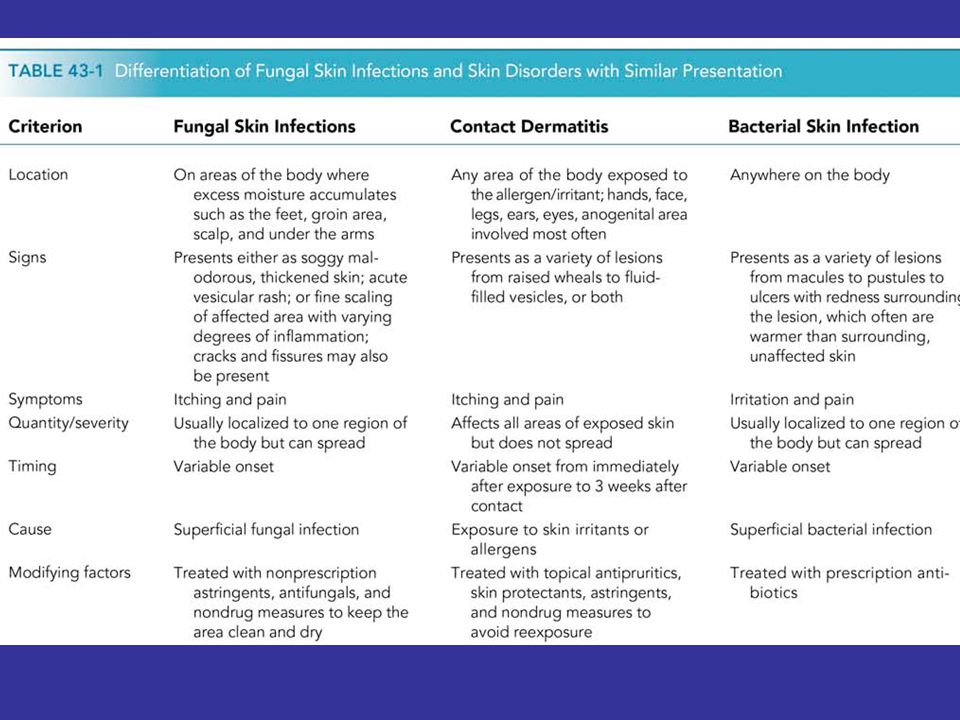
Similar presentations












>")







>")