Download presentation
Presentation is loading. Please wait.

1
Principles of Gynecological Endocrinology

2
Menarche - 1st menstruation
Menopause – last menstruation Amenorrhea - absence of menstruation Oligomenorrhea – rare menses (40 d – 6 months) Hypomenorrhea – reduction in duration and/or amount of menstrual bleeding Polimenorrhea – frequent menses (less than 25 d) Hypermenorrhea - long and/or extensive menstrual bleeding Dysfunctional uterine bleeding – irregularity without organic pathology
 Hypomenorrhea – reduction in duration and/or amount of menstrual bleeding. Polimenorrhea – frequent menses (less than 25 d) Hypermenorrhea - long and/or extensive menstrual bleeding. Dysfunctional uterine bleeding – irregularity without organic pathology.")
3
Reproductive cycle GnRH FSH LH E2 P 1 5 14 21 28 ovulation
No implantation

4
Amenorrhea Primary – woman has menstruated never before
Secondary – 6 months interval after last menstruation

5
Amenorrhea - Causes Pregnancy Hypothalamic-Pituitary Dysfunction
Ovarian dysfunction Pathology of the genital outflow tract

6
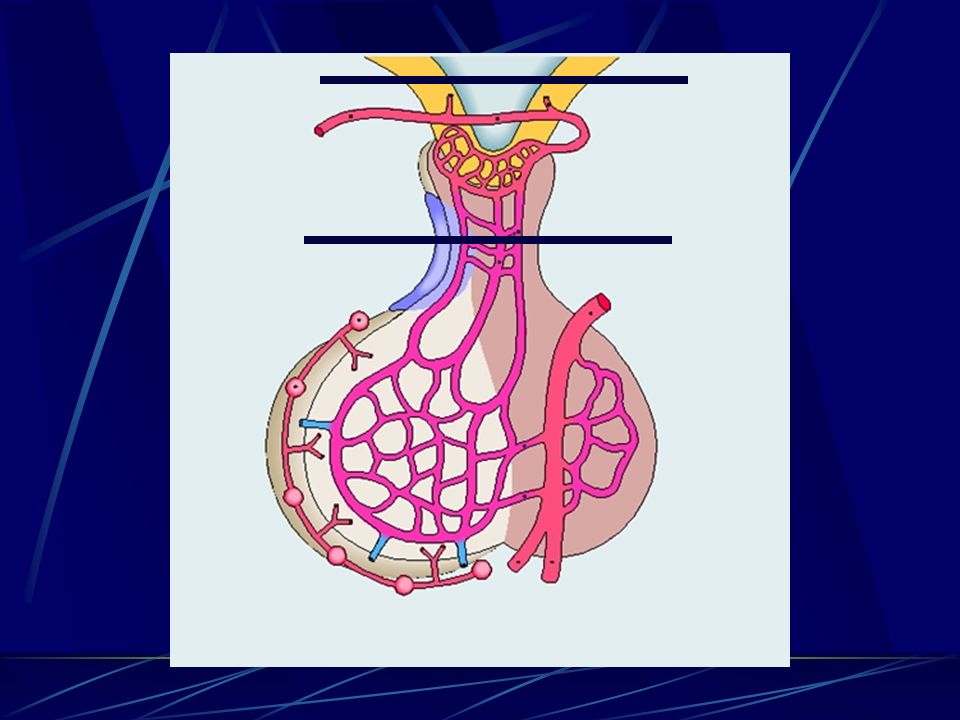
Hypothalamic-Pituitary Dysfunction
Disturbances of the pulsatile manner of the GnRH release or FSH and LH release Causes Congenital – Isolated hypogonadotropic hypogonadism Functional Weight loss Excessive exercise Obesity Drugs Psychogenic causes Anorexia nervosa Chronic anxiety Head injury Neoplastic diseases of the hypothalamo–pituitary region Diagnosis – medical history; low E2, PRL, low FSH and LH levels; CT; NMR; GnRH test

8
Premature Ovarian failure
Lack of ovarian follicles Resistance to pituitary stimulation (FSH, LH) Additional symptoms similar to those associated with menopause Hot flushes, mood changes, sleep disturbances, headaches, vaginal dryness and/or pruritus, dyspareunia, diaphoresis, altered libido
 Additional symptoms similar to those associated with menopause. Hot flushes, mood changes, sleep disturbances, headaches, vaginal dryness and/or pruritus, dyspareunia, diaphoresis, altered libido.")
9
Ovarian failure Causes
Chromosomal abnormalities 45,X gonadal dysgenesis (Turner,s syndrome) 46,XY (Sweyer,s syndrome) Androgen insensitivity syndrome Gonadropin-resistant ovary syndrome (Savage’s syndrome) Premature menopause Autoimmune ovarian failure (Blizzard’s syndrome) Iatrogenic – chemo- and radiotherapy, surgery Diagnosis - medical history; low E2, elevated FSH and LH levels; E-P test, exogenous Gn
 46,XY (Sweyer,s syndrome) Androgen insensitivity syndrome. Gonadropin-resistant ovary syndrome (Savage’s syndrome) Premature menopause. Autoimmune ovarian failure (Blizzard’s syndrome) Iatrogenic – chemo- and radiotherapy, surgery. Diagnosis - medical history; low E2, elevated FSH and LH levels; E-P test, exogenous Gn.")
10
Pathology of the genital outflow tract
Congenital defects of the uterus and/or vagina preventing menstrual bleeding Müllerian anomalies Lack of the uterus and/or vagina (Mayer-Rokitansky-Kuster-Hauser syndrome) Imperforate hymen Treatment - surgery Asherman’s syndrome – scarring of the uterine cavity After dilation and curettage (D&C) Treatment – hysteroscopy; E2
 Imperforate hymen. Treatment - surgery. Asherman’s syndrome – scarring of the uterine cavity. After dilation and curettage (D&C) Treatment – hysteroscopy; E2.")
11
Obstruction of the genital outflow tract – Congenital defects

12
Amenorrhea - diagnosis
Prolactin serum level Hyperprolactinemia Elevated Normal P Positive Anovulation Negative E+P Obstruction of Genital outflow Negative Positive FSH level Elevated Decreased Hypothalamic-Pituitary Dysfunction Ovarian failure

13
Treatment of the amenorrhea
Congenital – Isolated hypogonadotropic hypogonadism – E and P replacement, exogenous GnRH in pulsatile manner Functional – changing behavior Drugs - Psychogenic causes Anorexia nervosa Chronic anxiety Head injury Neoplastic diseases - surgery Prolactin secreting adenoma – bromocriptine Ovarian failure – hormonal replacement Obstruction of the genital outflow tract - surgery

14
Dysfunctional uterine bleeding
Irregularity without organic pathology Usually associated with anovulation (periodical ovulation) Causes Hyperprolactinemia PCOD Hyperandrogenism Obesity Early stage of premature ovarian failure Unknown Irregular, extensive uterine bleeding
 Causes. Hyperprolactinemia. PCOD. Hyperandrogenism. Obesity. Early stage of premature ovarian failure. Unknown. Irregular, extensive uterine bleeding.")
15
Anovulatory cycle E2 P 1 5 14 21 28 ovulation

16
Dysfunctional uterine bleeding
Chronic estrogen stimulation, unopposed with progesterone Endometrium outgrows its blood supply Ischemia, necrosis The endometrium is partially shed Irregular, unpredictable, bleeding The the extent of the bleeding depends on the levels of the estradiol Infrequent and light Frequent and heavy Elongated mitogenic stimulation without progesterone action

17
Dysfunctional uterine bleeding
Luteal phase defect The ovulation exist Corpus luteum is poorly developed and insufficient Shortening of the reproductive cycle Menses occur earlier than expected If conception and implantation occur the function of the corpus luteum is not adequate to support the gestation

18
Dysfunctional uterine bleeding - diagnosis
Medical history Irregular uterine bleeding Lack of premenstrual symptoms characteristic for ovulatory cycles: Breast tenderness and fullness, abdominal bloating, mood changes, edema, weight gain, menstrual cramps Exclusion of the organic causes Uterus – leyomioma, infection, polyps, neoplasmic diseases Cervix – polyps, erosions, carcinoma Vagina – carcinoma, injuries, foreign bodies

19
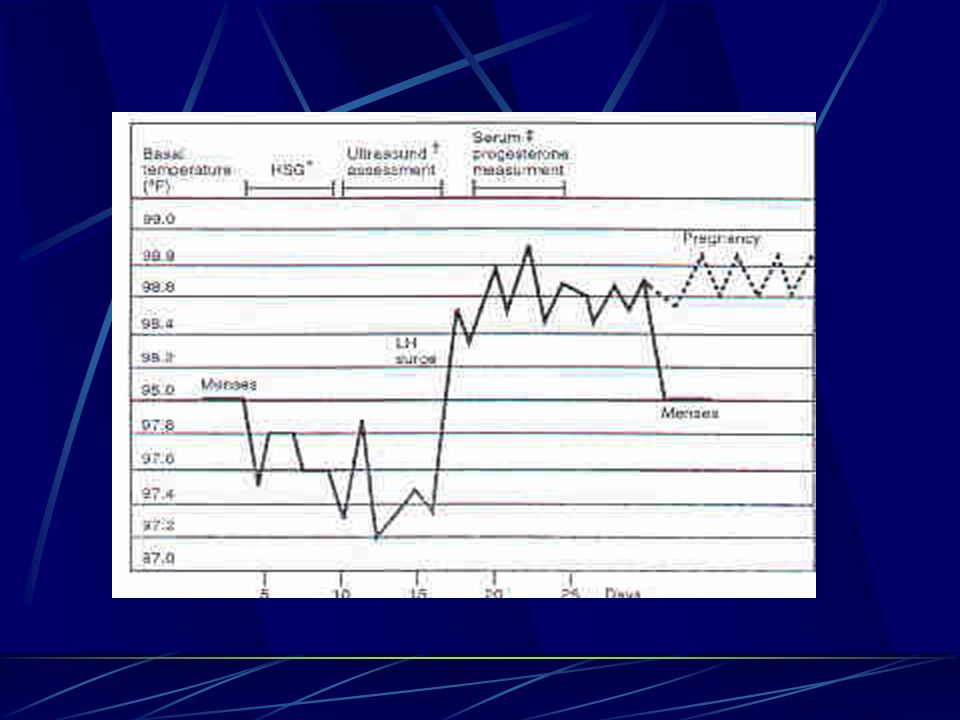
Dysfunctional uterine bleeding – diagnosis (cont.)
Confirmation of anovulation BBT Ultrasound examination Periovulatory pain Luteal phase progesterone serum levels Endometrial biopsy Proliferative endometrium Endometrial hyperplasia

21
Dysfunctional uterine bleeding - treatment
Termination of the bleeding (treatment of the acute hemorrhage) - hospitalization Administration of progestational agent for 10 days – secretory changes in the endometrium High doses of estrogen and progestational agent D&C Establishment of regular cycles (prevention of recurrences) OC progestational agent – 16th-25th day of cycle Diagnosis and treatment of Hyperprolactinemia, PCOS, Hyperandrogenism, Obesity
 - hospitalization. Administration of progestational agent for 10 days – secretory changes in the endometrium. High doses of estrogen and progestational agent. D&C. Establishment of regular cycles (prevention of recurrences) OC. progestational agent – 16th-25th day of cycle. Diagnosis and treatment of. Hyperprolactinemia, PCOS, Hyperandrogenism, Obesity.")
22
Hyperprolactinemia HYPOTHALAMUS OVARIAN STEROIDS OVARY ANDROGENS
ADRENALS

23
Hyperprolactinemia - Causes
Adenoma and microadenoma Prolactinoma Others Thyroid gland insufficiency – TRH increase Drugs Tranquilizers Antipsychotic (chlorpromazine) GI stimulant (Metoclopramide) Estrogens Methyldopa Chronic stress Inadequate regression after labor
 GI stimulant (Metoclopramide) Estrogens. Methyldopa. Chronic stress. Inadequate regression after labor.")
24
The effects of elevated level of prolactin
Suppressing pulsatile secretion of GnRH Decrease in Gn levels Disturbances in cyclic release of LH in response to the positive feedback of estradiol Decreased ovary sensitivity to Gn – receptors expression Stimulation of the adrenal androgens release

25
Hyprprolactinemia - symptoms
Galactorrhea Delayed menarche Luteal phase defect Anovulation Oligomenorrhea Primary or secondary amenorrhea

26
Hyprprolactinemia – diagnosis and treatment
Prolactin serum levels Basal In dynamic test (MCP, TRH) CT, NMR Treatment Bromocriptine Surgical treatment
 CT, NMR. Treatment. Bromocriptine. Surgical treatment.")
27
PCOS – polycystic ovarian syndrome
Definition Chronic anovulation or infrequent ovulation Androgen excess Metabolic abnormalities Hyperinsulinemia (50%) Insulin peripheral tissue resistance
 Insulin peripheral tissue resistance.")
28
PCOS Etiology Genetic predisposition Environmental factors
FOH – functional ovarian hyperandrogenism FAH - functional adrenal hyperandrogenism

29
PCOS LH Theca interna stimulation (+) adrostendion estrone
adipose tissue conversion androstendione estrone

30
PCOS Clinical Symptoms Oligomenorrhea or amenorrhea Acne
Hirsutism – excess body hair Appearance of coarse, dark and dense terminal hair Obesity (30-50%) Infertility
 Infertility.")
32
Hyperandrogenism - symptoms
Hirsutism – excess body hair Appearance of coarse, dark and dense terminal hair Acne Virilization – not present in PCOS Clitoral enlargement Deepening of the voice Involution of the breast Musculine appearance

33
PCOS Diagnosis Elevated LH serum level Increased LH/FSH ratio
Elevated androstendione serum level Elevated total testosterone serum level Elevated estrone serum level Lowered SHBG Ultrasound – polycystic ovaries, increased volume of ovaries BMI

34
PCOS Treatment OC Metformin
Androgen receptor antagonist – cyproterone acetate 5-alpha reductase inhibitors - finasterid FAH – dexametasone (0,25 md/d) Ovarian stimulation & ovulation induction
 Ovarian stimulation & ovulation induction.")
35
Premenstrual syndrome - PMS
The cyclic recurrence during the luteal phase of the menstrual cycle of a combination of distressing physical, psychologic, or behavioral changes that interfere with family, social, or work-related activities Premenstrual Dysphoric disorder – regular, cyclic occurrence of depressed mood, marked anxiety, affective lability, decreased interest in activities during the last week before the onset of menses Symptoms Somatic – breast tenderness and swelling, bloating, constipation or diarrhea, headache, weight gain Emotional – anxiety, irritability, confusion, crying, depression, changes of libido Behavioral – cravings, increase appetite, poor concentration

36
PMS - Etiology - theories
Psychiatric cyclic manifestations of psychopathology Endocrinologic abnormality in letal phase sex steroid levels – elevated E2, decreased progesterone cyclic occurrence of the symptoms presence of ER and PR in CNS Endorphin decrease of endorphin levels in the luteal-phase PMS symptoms similar to symptoms of opiate withdrawal Alleviation of symptoms after excessive exercise

37
Cyclic, luteal-phase related, occurrence of the symptoms
PMS - Diagnosis No specific historical or physical assessment findings or laboratory markers are diagnostic of PMS Cyclic, luteal-phase related, occurrence of the symptoms Menstrual diary – monitoring and recording of key symptoms and their severity on a daily basis Symptom-free follicular phase Exclusion of organic or functional pathology

38
PMS - Treatment Cooperation of gynecologist, psychiatrist, psychologist, endocrinologist Education of the patient Diet Fresh fruit and vegetables Minimizing refined sugars and fats Frequent small meals Minimizing salt Exercise Medical treatment Induction of anovulation – OC, Danazol, GnRH analogues Progesterone Nonsteroidal anti-inflamatory agents Diuretics Anxiolitic and antidepressant medications

40
Puberty - physical, emotional, and sexual transition from childhood to adulthood
Prerequisites Normal hypothalamus capable of responding to elevated levels of sex steroids by appropriate pulsatile secretion of GnRH Normal pituitary that is sensitive to GnRH and contains a pool of releasable gonadotropins Normal ovaries capable of secreting estrogen and progesterone in response to pituitary gonadotropins (FSH, LH)
")
41
Puberty The onset of the pubertal event in each individual is variable and influenced profoundly by genetic and environmental factors The average onset of puberty is between ages 8 and 13 years The events initiating the onset – unknown Increased maturity of the hypothalamic-pituitary axis – pulsatile GnRH secretion CNS appears to control the onset of puberty – an intrinsic CNS inhibitory mechanism suppressing pulsatile GnRH release Decrease in the CNS inhibitory action increase in pulsatile GnRH release and pituitary responsiveness

42
Puberty Adrenarche – at age 8-10 increased secretion of adrenal androgens (DHEA) – pubic and axillary hair growth – precedes the growth spurt by 2 years Maturation of the axis – increase in Gn response to GnRH Prepubertal children – minimal response to GnRH – small LH response Pubertal children – greater LH response to GnRH – sleep-associated gonadotropin secretion Development of of cyclic release of LH in response to the positive feedback of estradiol
 – pubic and axillary hair growth – precedes the growth spurt by 2 years. Maturation of the axis – increase in Gn response to GnRH. Prepubertal children – minimal response to GnRH – small LH response. Pubertal children – greater LH response to GnRH – sleep-associated gonadotropin secretion. Development of of cyclic release of LH in response to the positive feedback of estradiol.")
43
Puberty Event Age Hormone Breast budding 10-11 Estradiol
Sexual hair growth 10,5-11,5 Androgens Growth spurt GH Menarche 11,5-13 Estradiol Adult breast development 12,5-15 Progesterone Adult sexual hair 13,5-16 Androgens

44
Sources of the androgens in female
Hyperandrogenism Sources of the androgens in female Dehydroepiandrosterone (DHEA) – suprarenal glands Androstendion - suprarenal glands; ovaries Testosterone - suprarenal glands; ovaries; adipose tissue Functions of the androgens in female Precursors of the estrogens Stimulate and maintain sexual hair growth Responsible for female libido
 – suprarenal glands. Androstendion - suprarenal glands; ovaries. Testosterone - suprarenal glands; ovaries; adipose tissue. Functions of the androgens in female. Precursors of the estrogens. Stimulate and maintain sexual hair growth. Responsible for female libido.")
45
Hyperandrogenism - causes
Increased synthesis and release PCOD - ovary and/or adrenal glands Congenital adrenal hyperplasia (21- and 11-hydroxylase deficiency) Ovarian tumors – Androblastoma, Gynandroblastoma Adrenal adenoma Obesity Increased expression and/or sensitivity of the androgen receptors in peripherial tissues Increased 5 reductase activity (TDHT) Constitutional hirsutism Iatrogenic – glucocorticoids, OC, Danazol
 Ovarian tumors – Androblastoma, Gynandroblastoma. Adrenal adenoma. Obesity. Increased expression and/or sensitivity of the androgen receptors in peripherial tissues. Increased 5 reductase activity (TDHT) Constitutional hirsutism. Iatrogenic – glucocorticoids, OC, Danazol.")
46
Hyperandrogenism - symptoms
Hirsutism – excess body hair Appearance of coarse, dark and dense terminal hair Virilization Acne Clitoral enlargement Deepening of the voice Involution of the breast Musculine appearance

Similar presentations










>")





 2014.>")

 is a disorder that causes menstrual and ovulation irregularities, androgen excess, and infertility.>")


