Download presentation
Presentation is loading. Please wait.

1
LMCC Review Course: “Neonatology” Gregory Moore, MD, FRCPC Division of Neonatology March 2012

2
Outline 1. Resuscitation principles 1. Transition to ex-utero life 2. Normal newborn care and assessment 3. Small and Large-for-Gestational Age neonates and their problems 4. Prematurity and its complications 5. Problems of the term infant

3
For Starters … Infant (< 1 yr old) mortality: 5 deaths per 1000 live births (Canada) Due to congenital anomalies, prematurity, asphyxia, infections, SIDS Normal vitals for a baby at term: HR: 120-160/min * RR: 40-60/min * BP: 50-80/30-40 mmHg Sats: >95% by ~1 hr of age *
 mortality: 5 deaths per 1000 live births (Canada) Due to congenital anomalies, prematurity, asphyxia, infections, SIDS Normal vitals for a baby at term: HR: /min * RR: 40-60/min * BP: 50-80/30-40 mmHg Sats: >95% by ~1 hr of age *")
4
For Starters … Gestation (wks) Birth Weight (kg) 271.0 301.5 332.0 352.3 37-40 3.5 (2.5 – 4.5)
 Birth Weight (kg) (2.5 – 4.5)")
5
Newborn Resuscitation Initial steps: warm, dry, ‘stimulate’ Evaluate respirations Evaluate heart rate Evaluate tone Evaluate color Remember - the key to a baby’s transition to the real world is ‘opening’ the lungs: VENTILATION Oxygenation

6
1. ‘Red’ blood from placenta 2. ‘Less red’ blood from right to left atrium via patent foramen ovale 3. Small amount of ‘pink’ blood going to lungs In-utero 4. Pink blood goes from the pulmonary artery to aorta via ductus arteriosus … produces mixing of pink and less red blood

7
1. Cord is clamped Increases SVR 2. Foramen ovale functionally closes 3. Pulmonary arteries vasodilate to increase blood flow to the lungs Ex-utero 4. Ductus arteriosus closes

8
Fluid-filled alveoli in utero Diminished blood flow in-utero through fetal lungs

9
Importance of first breath

10
The End Product

11
Neonatal Resuscitation Program

12
90% of babies

13
9% of babies

14
0.9% of babies

15
0.1% of babies

16
Newborn Resuscitation A: Airway B: Breathing C: Circulation D: Drugs E: Environment F: Fluids G: Glucose “IV, O2, Monitor” … if distressed

17
NB. Newborn Resuscitation MECONIUM in the amniotic fluid AND depressed newborn (limp, not crying): Intubate and suction below cords FIRST Intubate and suction below cords FIRST Suspect diaphragmatic hernia: Intubate ASAP Intubate ASAP Pink when crying … blue when not: Suspect choanal atresia and try an oral airway Suspect choanal atresia and try an oral airway
: Intubate and suction below cords FIRST Intubate and suction below cords FIRST Suspect diaphragmatic hernia: Intubate ASAP Intubate ASAP Pink when crying … blue when not: Suspect choanal atresia and try an oral airway Suspect choanal atresia and try an oral airway.")
18
The Apgar Score

19
Ensure warmth and early nutrient intake Support breastfeeding Monitor weight and hydration status Educate about infant care ** Anticipatory guidance ** Principles of Routine Care

20
Prophylaxis for common problems Eye care: erythromycin ointment Eye care: erythromycin ointment Vitamin K: 1 mg IM Vitamin K: 1 mg IM Screening for disease: >24h Newborn screen (24-72 hr) Newborn screen (24-72 hr) PKU (1/15,000)PKU (1/15,000) Hypothyroidism (1/4000)Hypothyroidism (1/4000) 24 other diseases (OA/AA/FA disorders, SCA, Hgb’pathies’, CAH, galactosemia, endocrinopathies)24 other diseases (OA/AA/FA disorders, SCA, Hgb’pathies’, CAH, galactosemia, endocrinopathies) Neurosensory hearing loss (pre-d/c) Neurosensory hearing loss (pre-d/c) Hyperbilirubinemia (pre-d/c) Hyperbilirubinemia (pre-d/c) Blood group and Coombs if mother Rh negative
 Newborn screen (24-72 hr) PKU (1/15,000)PKU (1/15,000) Hypothyroidism (1/4000)Hypothyroidism (1/4000) 24 other diseases (OA/AA/FA disorders, SCA, Hgb’pathies’, CAH, galactosemia, endocrinopathies)24 other diseases (OA/AA/FA disorders, SCA, Hgb’pathies’, CAH, galactosemia, endocrinopathies) Neurosensory hearing loss (pre-d/c) Neurosensory hearing loss (pre-d/c) Hyperbilirubinemia (pre-d/c) Hyperbilirubinemia (pre-d/c) Blood group and Coombs if mother Rh negative")
21
The Newborn History Identification Identification Maternal History: Maternal History: AgeAge Past medical/surgicalPast medical/surgical Medications, Drugs/Smoking/EtOHMedications, Drugs/Smoking/EtOH Past pregnancy(ies) (GTPAL)Past pregnancy(ies) (GTPAL) Current pregnancy (including screening test results, antenatal steroid use)Current pregnancy (including screening test results, antenatal steroid use) Family History Family History Social History Social History Labour and Delivery History Labour and Delivery History Resuscitation History Resuscitation History Early Postnatal Course Early Postnatal Course
 (GTPAL)Past pregnancy(ies) (GTPAL) Current pregnancy (including screening test results, antenatal steroid use)Current pregnancy (including screening test results, antenatal steroid use) Family History Family History Social History Social History Labour and Delivery History Labour and Delivery History Resuscitation History Resuscitation History Early Postnatal Course Early Postnatal Course")
22
Physical Examination Vital signs Measurements plot! Gestational age assessment Overall appearance (well/unwell) System by system (or head to toe) **
 System by system (or head to toe) **.")
23
The depressed newborn Neurological: Asphyxia, CNS Trauma Asphyxia, CNS Trauma Respiratory: Apnea (secondary) Apnea (secondary) Cardiovascular: Hypovolemia/shock/hydrops Hypovolemia/shock/hydrops Congenital: Malformations Malformations Drugs
 Apnea (secondary) Cardiovascular: Hypovolemia/shock/hydrops Hypovolemia/shock/hydrops Congenital: Malformations Malformations Drugs")
24
The Basic Tests Blood gas (arterial or capillary) Glucose Electrolytes Complete Blood Count + differential Blood culture Chest X-ray Consider: Lactate, CRP, echocardiogram, abdominal x-ray Full septic workup if > 72 hours old
 Glucose Electrolytes Complete Blood Count + differential Blood culture Chest X-ray Consider: Lactate, CRP, echocardiogram, abdominal x-ray Full septic workup if > 72 hours old")
25
Perinatal Asphyxia - Must be documented by cordocentesis, fetal scalp blood sampling, cord blood sampling pH 15 mEq/L Apgar less than 5 at 5 minutes Encephalopathy Multiorgan involvement (heart, kidneys, marrow, liver) - Neonatal encephalopathy must be documented for perinatal asphyxia to be considered as a cause of later neurodevelopmental problems
 - Neonatal encephalopathy must be documented for perinatal asphyxia to be considered as a cause of later neurodevelopmental problems")
26
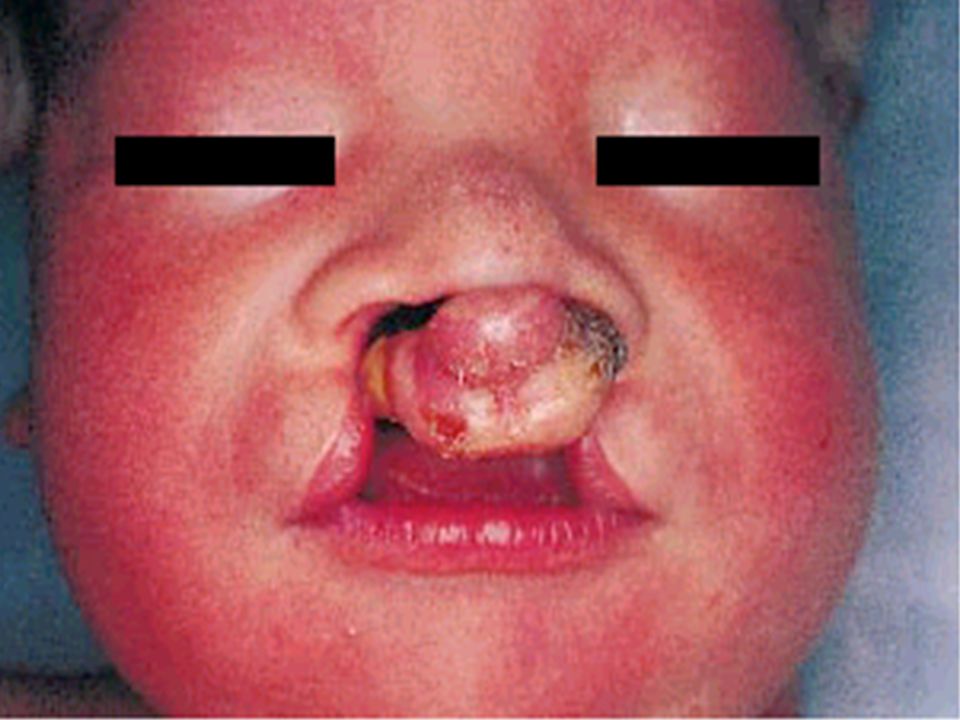
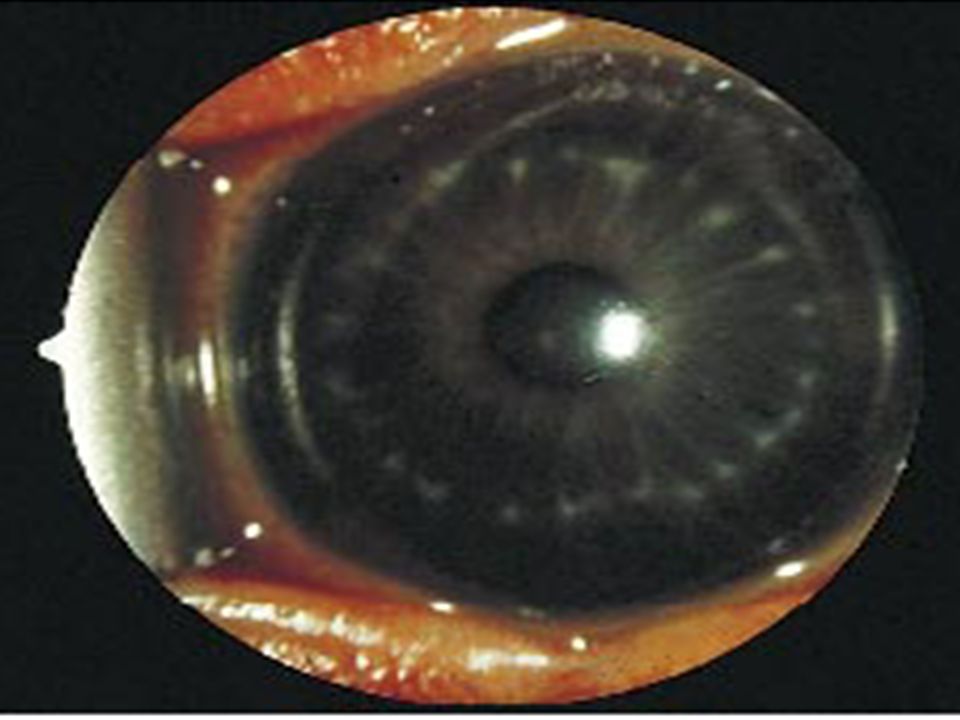
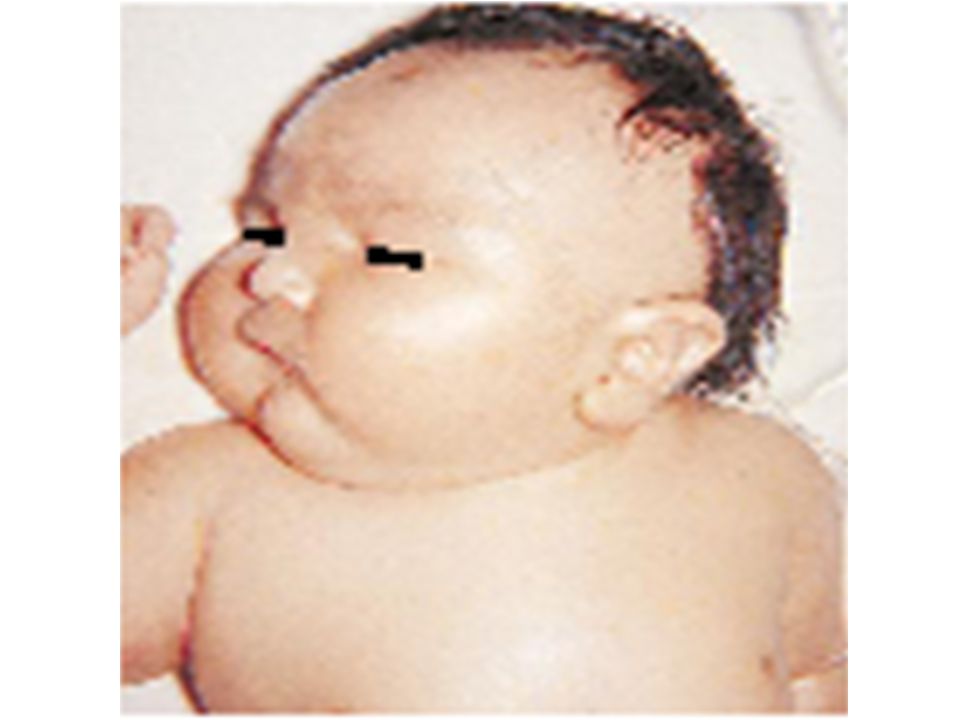
Most common anomalies noted on initial exam

37
Most frequent birth injuries Asphyxia Broken clavicle Facial palsy Brachial plexus injury Fractures of humerus or skull Lacerations or scalp injuries Ruptured internal organs Testicular trauma Fat necrosis

42
Differentiating Scalp Injuries

43
Commonest Congenital Abdominal Masses Renal (55%) Genital (15%) Gastrointestinal (15%) Liver and Biliary (5%) Retroperitoneal (5%) Adrenal (5%)
 Genital (15%) Gastrointestinal (15%) Liver and Biliary (5%) Retroperitoneal (5%) Adrenal (5%)")
44
Common physical findings of clinical significance Apnea, bradycardia, cyanosis (peripheral) Tachypnea, grunting Absent or decreased femoral pulses Heart murmur, cyanosis (central) Hypotonia Organomegaly Absent red reflex Jaundice Plethora or pallor or diffuse petechiae
 Tachypnea, grunting Absent or decreased femoral pulses Heart murmur, cyanosis (central) Hypotonia Organomegaly Absent red reflex Jaundice Plethora or pallor or diffuse petechiae")
45
Disorders of gestation length or of growth Small for gestational age: <2SD below Large for gestational age: >2SD above Prematurity: <37 weeks gestation Postmaturity: >42 weeks gestation

47
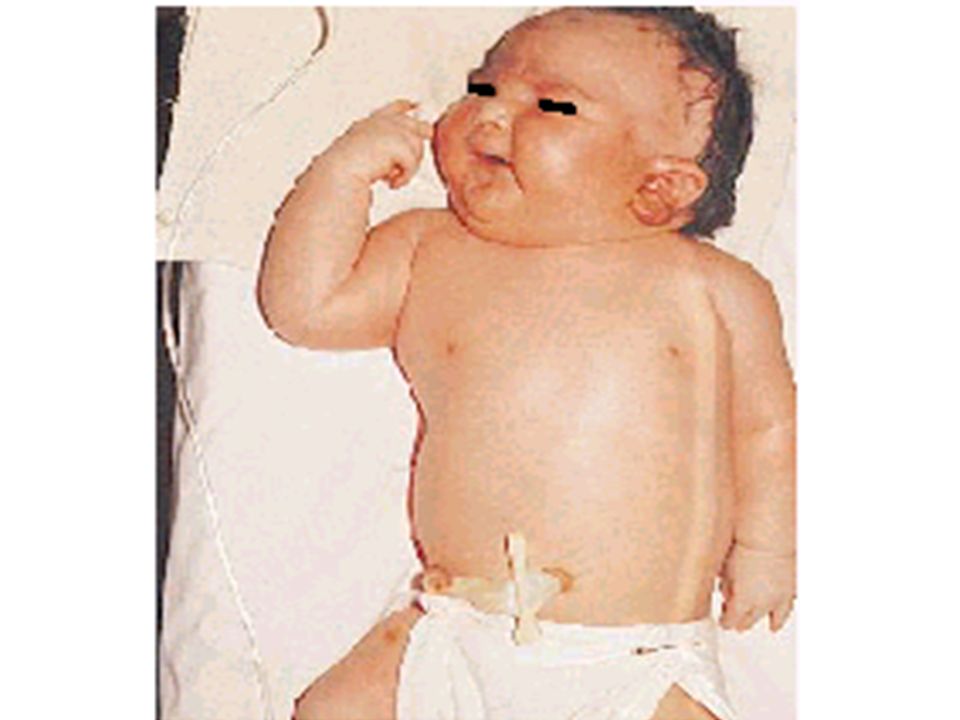
Birth Weight Matters …

48
Small for gestational age: Etiologies Constitutional Maternal Illness, Rx/EtOH/drugs/cigs, nutrition Illness, Rx/EtOH/drugs/cigs, nutrition Placental Fetal Genetic disorder, infections (TORCH) Genetic disorder, infections (TORCH)
 Genetic disorder, infections (TORCH)")
49
Small for gestational age: complications Asphyxia Meconium aspiration Congenital malformations Hypoglycemia Hypothermia Hypocalcemia Polycythemia-hyperviscosity Increased neonatal mortality (OR 2.77) Long term morbidity …
 Long term morbidity …")
50
Small for gestational age: Management Optimal resuscitation Maintenance of body temperature Early feeds or administration of glucose Meticulous history and physical examination, including placenta Work-up for etiology

51
Disorders of gestation length or of growth Small for gestational age: <2SD below Large for gestational age: >2SD above Prematurity: <37 weeks gestation Postmaturity: >42 weeks gestation

53
Large for gestational age: Etiologies Constitutional Abnormal maternal glucose tolerance Syndromes: Beckwith-Wiedemann Sotos Sotos

54
Large for gestational age: Complications Asphyxia Birth trauma Hypoglycemia

55
Large for gestational age: Management Optimal resuscitation Early feeds or administration of glucose

56
Disorders of gestation length or of growth Small for gestational age: <2SD below Large for gestational age: >2SD above Prematurity: <37 weeks gestation Postmaturity: >42 weeks gestation

59
Causes/Risks for Prematurity Fetal: Multiple gestation Fetal hydrops (immune and non-immune) Congenital/Genetic anomalies Placental: Placenta praevia Abruptio placenta Placental insufficiency Uterine: Incompetent cervix Excessive enlargement (hydramnios) Malformations (leiomyomas, septate) Maternal: Previous history of premature delivery Pre-eclampsia Premature rupture of membranes Smoking, substance abuse Chronic medical illnesses, low weight, ‘extremes’ of age Infections (urinary, cervical, amniotic)-group B streptococcus, herpes, TORCH, etc. Iatrogenic (indicated induction of labor)
.")
60
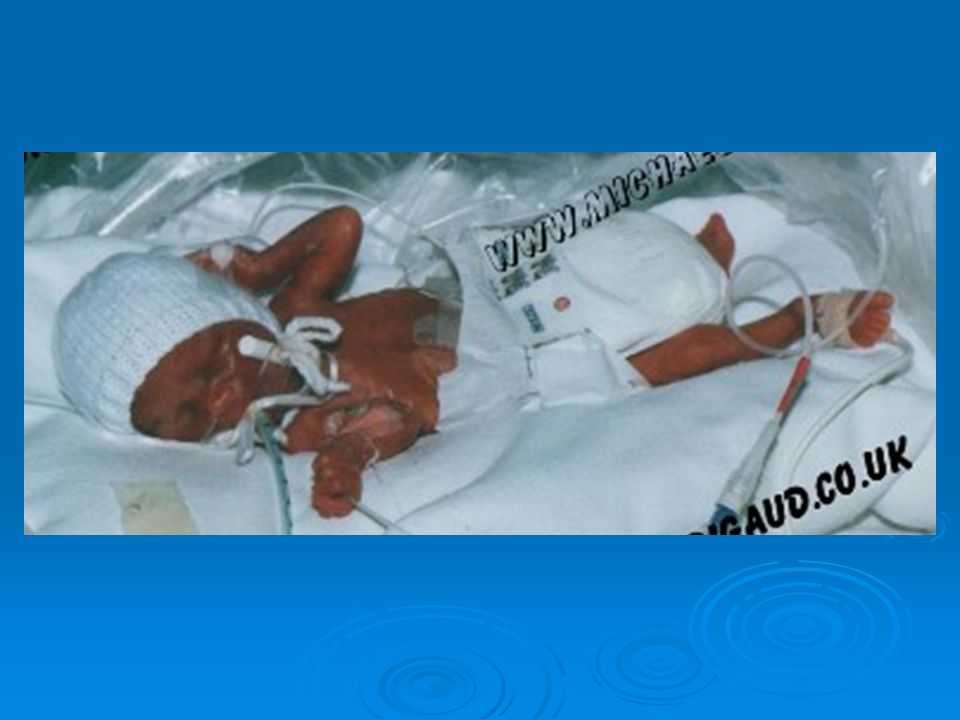
And then there was a baby … Transfer to a level 2 nursery if: < 36 weeks GA < 36 weeks GA < 2 kg < 2 kg Transfer to a level 3 nursery if: < 32 weeks GA < 32 weeks GA Respiratory support required Respiratory support required Need for special care due to: Risk of complications Risk of complications Nutritional needs Nutritional needs Transfer Mom prior to birth if at all possible

61
Prematurity: Complications Respiratory distress syndrome Bronchopulmonary dysplasia Apnea of prematurity Patent ductus arteriosus Intraventricular hemorrhage Periventricular leukomalacia Necrotizing enterocolitis Sepsis Anemia Retinopathy of prematurity

62
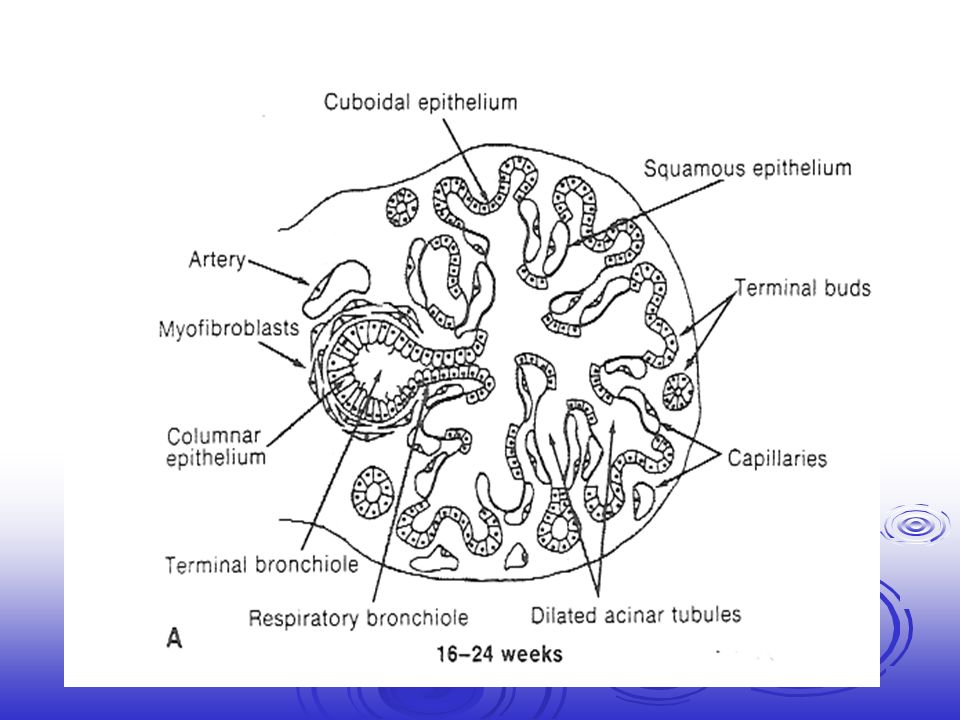
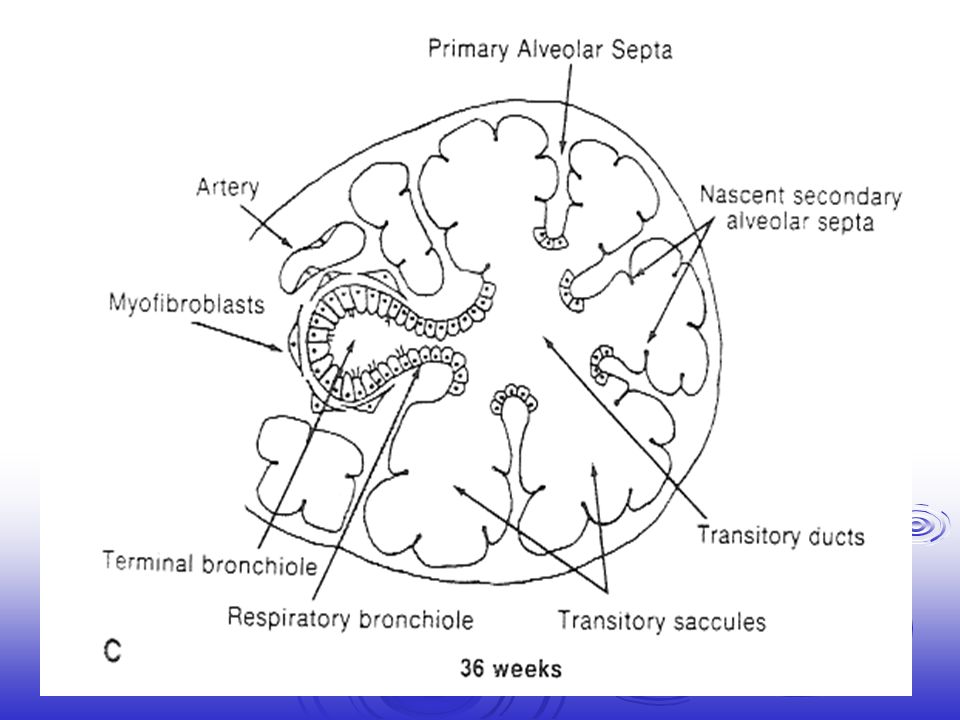
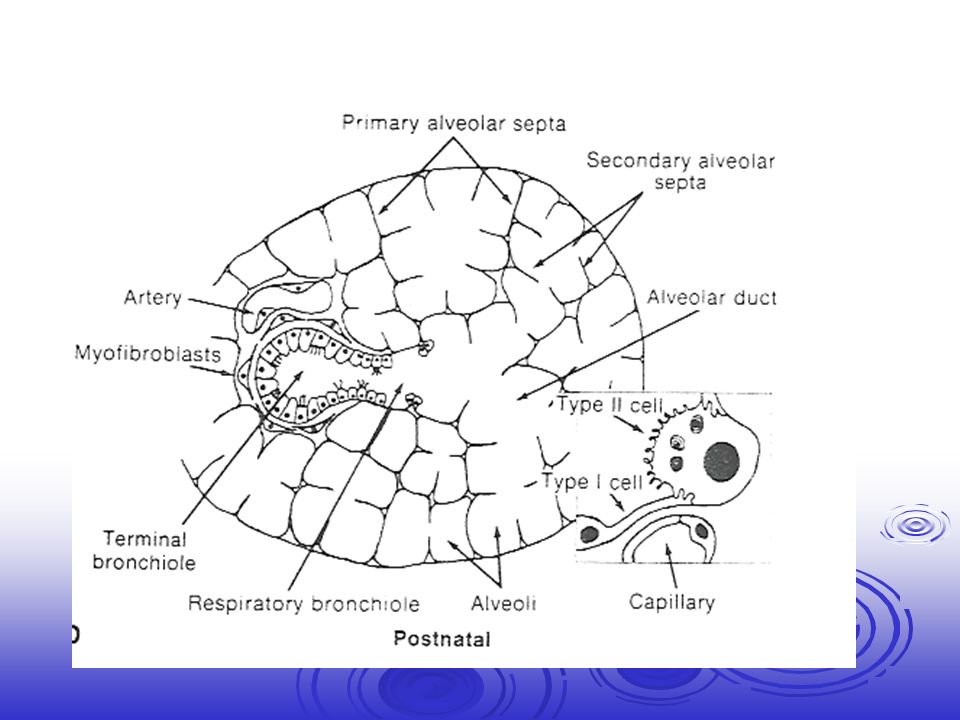
Respiratory Distress Syndrome Etiology Anatomic immaturity of the lung Anatomic immaturity of the lung Increased interstitial and alveolar lung fluid Increased interstitial and alveolar lung fluid Surfactant deficiency Surfactant deficiency

64
Courtesy of Professor Louis De Vos http://www.ulb.ac.be/sciences/biodic/index.html 17 Weeks

65
Courtesy of Professor Louis De Vos http://www.ulb.ac.be/sciences/biodic/index.html 22 Weeks

66
Courtesy of Professor Louis De Vos http://www.ulb.ac.be/sciences/biodic/index.html 25 Weeks

69
CXR: poor aeration, ground-glass appearance, homogenous, air bronchograms

70
Respiratory Distress Syndrome Management: Prevention - antenatal steroids Prevention - antenatal steroids Positive pressure ventilation Positive pressure ventilation Oxygen Oxygen +/- Surfactant (requires intubation) +/- Surfactant (requires intubation)
 +/- Surfactant (requires intubation)")
71
Pressure (cmH 2 0) Volume (ml)
 Volume (ml)")
72
Bronchopulmonary Dysplasia Respiratory symptoms, x-ray abnormalities, and O2 req’t for > 28 d and persisting at 36 wks corrected GA Pathophysiology: Disturbed alveolarization with increased alveolar- to-capillary distance and decreased alveolar-to- capillary ration Secondary to: Lung inflammation Mucociliary dysfunction Airway narrowing Hypertrophied airway smooth muscle Alveolar collapse Constriction of pulmonary vascular bed

76
Bronchopulmonary Dysplasia Management: Prevention: IM Vitamin A, Caffeine Prevention: IM Vitamin A, Caffeine NUTRITION NUTRITION Oxygen +/- ventilation Oxygen +/- ventilation +/- Diuretics +/- Diuretics +/- Steroids: systemic, inhaled +/- Steroids: systemic, inhaled +/- Bronchodilators +/- Bronchodilators Prognosis: Increased respiratory illnesses in childhood Increased respiratory illnesses in childhood Decreased long-term lung function Decreased long-term lung function BUT, fine in the playground by pre-school age (usually …) BUT, fine in the playground by pre-school age (usually …)
 BUT, fine in the playground by pre-school age (usually …)")
77
Apnea of Prematurity Central, obstructive, or mixed ** Majority of <32 weeks Treat with: Adequate positioning Adequate positioning Oxygen Oxygen Methylxanthines (i.e. Caffeine) Methylxanthines (i.e. Caffeine) CPAP CPAP Ventilation if necessary Ventilation if necessary
 Methylxanthines (i.e. Caffeine) CPAP CPAP Ventilation if necessary Ventilation if necessary.")
78
Patent ductus arteriosus Seen in >60% of 60% of <1000 g babies Management strategies: Preload/afterload reduction Preload/afterload reduction Adequate oxygenation Adequate oxygenation Optimize pH Optimize pH Indomethacin/Ibuprofen Indomethacin/Ibuprofen Surgery (PDA ligation) Surgery (PDA ligation) Conservative management Conservative management Prognosis: Multiple associations (NEC, CLD, etc …) but no proven causation Multiple associations (NEC, CLD, etc …) but no proven causation
 Surgery (PDA ligation) Conservative management Conservative management Prognosis: Multiple associations (NEC, CLD, etc …) but no proven causation Multiple associations (NEC, CLD, etc …) but no proven causation")
79
Metabolic Problems of Prematurity Hypoglycemia Fluid/electrolyte imbalance Hypocalcemia/hypomagnesemia Hyperbilirubinemia Hypothermia

80
Intraventricular hemorrhage Common in < 1500 gm babies Usually evident in 1st week of life Reasons: highly vascularized germinal matrix highly vascularized germinal matrix less basement membrane to capillaries less basement membrane to capillaries abnormal cerebral autoregulation abnormal cerebral autoregulation Prognosis: Good - small amounts of bleeding in the ventricles Good - small amounts of bleeding in the ventricles Poorer - large amount intraparenchymally or if post- hemorrhagic hydrocephalus Poorer - large amount intraparenchymally or if post- hemorrhagic hydrocephalus

81
Periventricular leukomalacia Pathophysiology: Ischemic lesion to watershed area around ventricles in premature infants Ischemic lesion to watershed area around ventricles in premature infants Link to inflammation? Link to inflammation? Most often shows up 3-4 wks after delivery Most often shows up 3-4 wks after delivery Prognosis: Correlated with cerebral palsy Correlated with cerebral palsy

82
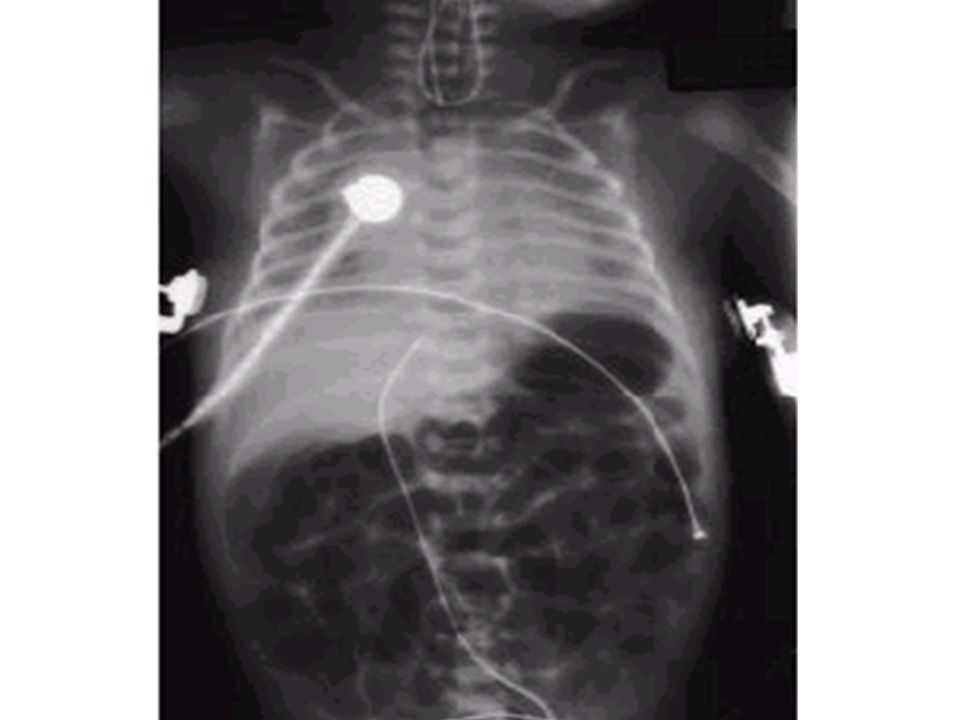
Necrotizing Enterocolitis 1-5% NICU admissions Multi-factorial etiology: Feeds, Prematurity, Ischemia, Infection Feeds, Prematurity, Ischemia, Infection Diagnosis: clinical and radiologic Treatment: Decompression (NPO, NG tube) Decompression (NPO, NG tube) Antibiotics Antibiotics Surgery prn Surgery prn Prognosis: 30% mortality if <1500 g 30% mortality if <1500 g
 Decompression (NPO, NG tube) Antibiotics Antibiotics Surgery prn Surgery prn Prognosis: 30% mortality if <1500 g 30% mortality if <1500 g")
86
Sepsis Suboptimal immune function in preemies plus poor skin barrier, indwelling catheters GBS and coliforms cause early onset sepsis < 5-7 days of life < 5-7 days of life Nosocomial sepsis common in prems Most common = coagulase negative staphylococcus Most common = coagulase negative staphylococcus Fungi can also be problematic in > 1 week of life Fungi can also be problematic in > 1 week of life

87
Anemia of Prematurity Reasons: decreased hemoglobin at delivery decreased hemoglobin at delivery decreased RBC survival decreased RBC survival blunted erythropoietin response blunted erythropoietin response IATROGENIC IATROGENIC Treatment: prevention prevention iron supplementation iron supplementation transfusion transfusion EPO EPO

88
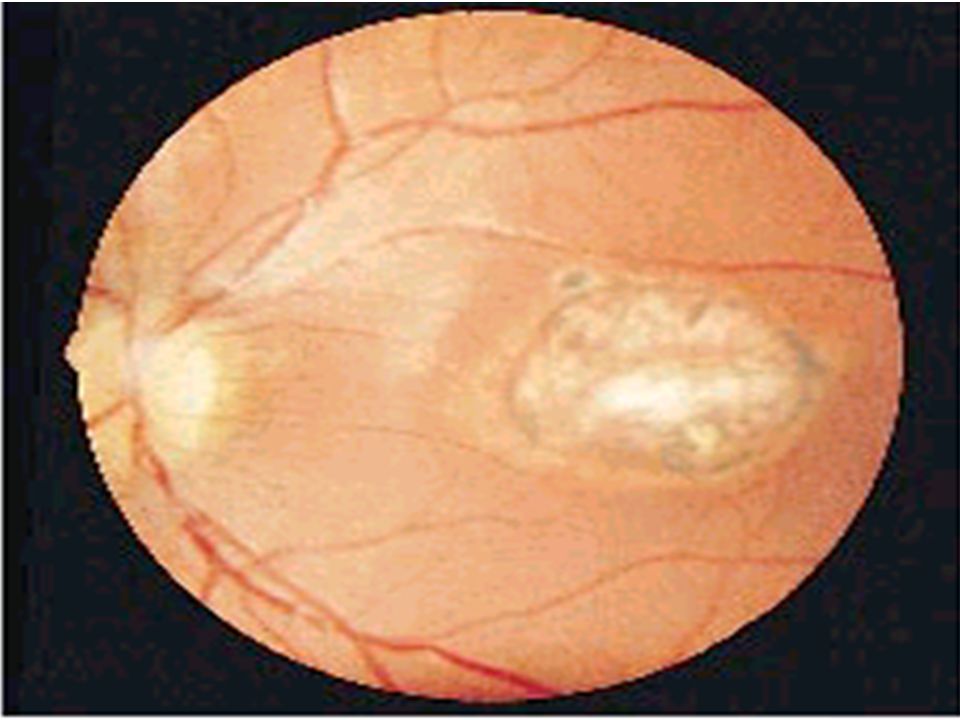
Retinopathy of Prematurity 40-70% NICU survivors < 1000 g Etiology: vasoconstriction leading to abnormal vascular proliferation vasoconstriction leading to abnormal vascular proliferation Diagnosis: Screening Screening Treatment: Close monitoring, laser if necessary Close monitoring, laser if necessary

89
Long Term Outcomes – 24 weeks Local survival (2006-2008)~ 60% Risk of severe disability: very low IQ, unable to walk, blindness and/or deafness ~ 15-20% of survivors Risk of moderate disability: low IQ, walk with aid, impaired vision and/or correctable hearing loss ~ 20-30% of survivors Deafness~ 2% of survivors Blindness1-10% of survivors Overall, chance of being ‘normal’ or mildly impaired ~ 50-65% of survivors
~ 60% Risk of severe disability: very low IQ, unable to walk, blindness and/or deafness ~ 15-20% of survivors Risk of moderate disability: low IQ, walk with aid, impaired vision and/or correctable hearing loss ~ 20-30% of survivors Deafness~ 2% of survivors Blindness1-10% of survivors Overall, chance of being ‘normal’ or mildly impaired ~ 50-65% of survivors")
90
Disorders of gestation length or of growth n Small for gestational age: <2SD below n Large for gestational age: >2SD above n Prematurity: <37 weeks gestation n Postmaturity: >42 weeks gestation

91
Postmaturity Labour tends to be induced to avoid problems of postmaturity, however if dates not accurate may still occur Possible complications Growth disturbances Growth disturbances Asphyxia Asphyxia Meconium aspiration syndrome Meconium aspiration syndrome

92
Problems of the Term Newborn Respiratory Cardiac Sepsis Digestive Jaundice Anemia, polycythemia, hemorrhage Renal Endocrine Neurologic

93
Respiratory Distress in the Newborn Respiratory Cardiac Infectious Neurologic Metabolic Gastrointestinal Hematological Musculoskeletal

94
Respiratory Problems in the Term Newborn Transient tachypnea of the newborn Meconium aspiration Persistent pulmonary hypertension Pulmonary air leaks/Pneumothorax Congenital malformations Pulmonary hemorrhage Pneumonia

95
Transient Tachypnea of the Newborn Failure to clear lung fluid Associated with: Absent labour (planned C/S or C/S without labour) or; Absent labour (planned C/S or C/S without labour) or; Short labour or; Short labour or; Initial weak or absent respirations Initial weak or absent respirations Improves with time
 or; Absent labour (planned C/S or C/S without labour) or; Short labour or; Short labour or; Initial weak or absent respirations Initial weak or absent respirations Improves with time")
97
Pneumonia Can initially be difficult to distinguish from TTN/RDS Group B Strep #1 Consolidation may appear after a few days

99
Meconium Aspiration Syndrome Meconium-stained amniotic fluid Intrauterine insult may lead to gasping Meconium aspirated Pneumonitis Pneumonitis Airway occlusion Airway occlusion Pulmonary air leak syndrome Pulmonary air leak syndrome May lead to persistent pulmonary hypertension

100
Congenital Malformations Anomalies anywhere along airways: Nose to alveoli Nose to alveoli Extrinsic or intrinsic Extrinsic or intrinsic Atresias Cysts Diaphragmatic hernia

102
Persistent Pulmonary Hypertension Associated with: Asphyxia Asphyxia Meconium aspiration Meconium aspiration Sepsis Sepsis Right to left shunting through PDA (i.e. persistent fetal circulation) Treatment: Oxygenation, ventilation Oxygenation, ventilation Maintain blood pressure Maintain blood pressure Pulmonary vasodilators Pulmonary vasodilators
 Treatment: Oxygenation, ventilation Oxygenation, ventilation Maintain blood pressure Maintain blood pressure Pulmonary vasodilators Pulmonary vasodilators.")
103
Congenital Heart Disease: Presentations Cyanosis Congestive heart failure Murmurs Dysrhytmias

104
Sepsis: Risk factors Preterm rupture of membranes e.g. weeks e.g. weeks Prolonged rupture of membranes >18 hours >18 hours Maternal group B strep carriage Maternal GBS bacteriuria Previous infant with GBS infection Chorioamnionitis

105
Neonatal Sepsis THINK OF IT! Signs may be subtle, non-specific Signs may be subtle, non-specific Incidence bacterial sepsis = 1-5/1000 live births Incidence bacterial sepsis = 1-5/1000 live births Commonest organisms: Commonest organisms: Group B streptococcusGroup B streptococcus Gram negatives (E coli, Klebsiella)Gram negatives (E coli, Klebsiella) Enterococcus, H flu, staph speciesEnterococcus, H flu, staph species ListeriaListeria Work up and treat if suspect sepsis Use broad spectrum antibiotics Use broad spectrum antibiotics
Gram negatives (E coli, Klebsiella) Enterococcus, H flu, staph speciesEnterococcus, H flu, staph species ListeriaListeria Work up and treat if suspect sepsis Use broad spectrum antibiotics Use broad spectrum antibiotics.")
106
Ophthalmia neonatorum 1st days - differentiate chemical vs infected 2nd-3rd wk - viral or bacterial Gonococcal: within 5 days of birth within 5 days of birth gram negative intracellular diplococci gram negative intracellular diplococci if suspect, Penicillin asap if suspect, Penicillin asap highly contagious highly contagious Chlamydia: 5-14 days 5-14 days conjunctival scraping conjunctival scraping topical antibiotics topical antibiotics

108
Congenital Infections ** CMV: 5-25/1,000 live births 5-25/1,000 live births Asymptomatic vs severe symptoms Asymptomatic vs severe symptoms Microcephaly, thrombocytopenia, hepatosplenomegaly, chorioretinitis Microcephaly, thrombocytopenia, hepatosplenomegaly, chorioretinitis Sequelae of hearing loss and developmental delay Sequelae of hearing loss and developmental delay Rubella 0.5/1,000 0.5/1,000 Cataracts, rash, congenital heart disease, developmental delay Cataracts, rash, congenital heart disease, developmental delay

111
Congenital Infections Toxoplasmosis: 0.5-1.0/1,000 0.5-1.0/1,000 Hydrocephalus, cranial calcifications, chorioretinitis Hydrocephalus, cranial calcifications, chorioretinitis Syphilis: 0.1/1,000 0.1/1,000 Snuffles, osteochondritis/periostitis, rash Snuffles, osteochondritis/periostitis, rash Herpes Simplex Virus: Vesicles, keratoconjuntivitis, CNS findings Vesicles, keratoconjuntivitis, CNS findings ‘Viral’ sepsis ‘Viral’ sepsis

112
Congenital syphilis Treat mother no matter what stage of pregnancy If adequate maternal treatment and no signs of infection in newborn, give one dose IM penicillin If inadequate maternal treatment, give 10 days of IV penicillin

113
Neonatal herpes simplex Only about 1/3 mothers have overt signs Infection can be disseminated or local Usually present at 5-10 days of age If suspect: Cultures, PCR Cultures, PCR Treat with Acylovir Treat with Acylovir

115
Maternal hepatitis B carrier Give baby hepatitis vaccine as soon as possible after birth (first 12 hours) Bath Universal precautions Immune globulin in first 7 days
 Bath Universal precautions Immune globulin in first 7 days")
116
HIV Virus can be transmitted transplacentally, intrapartum, or postpartum Screen mothers Treat mothers with antiretrovirals Treat babies with AZT for 6 wks Universal precautions Look for other infections (HepB/C) No breastfeeding in developed world
 No breastfeeding in developed world")
117
Vomiting in the Newborn Not uncommon for some vomiting in 1st few hours and days after birth Overfeeding, poor burping Overfeeding, poor burping DDx: GI: obstruction, reflux, milk allergy, NEC GI: obstruction, reflux, milk allergy, NEC Infection: Sepsis, Meningitis, UTI Infection: Sepsis, Meningitis, UTI Endocrine: Adrenal hyperplasia Endocrine: Adrenal hyperplasia CNS: Increased ICP CNS: Increased ICP Drugs Drugs Bilious vomiting is a medical emergency!

118
Upper GI problems vomiting Esophageal: first feed, soon after feed first feed, soon after feed excessive drooling excessive drooling if T-E fistula, risk of aspiration if T-E fistula, risk of aspiration Small bowel atresias Malrotation and volvulus Achalasia Chalasia/GER Pyloric stenosis } Need to r/o

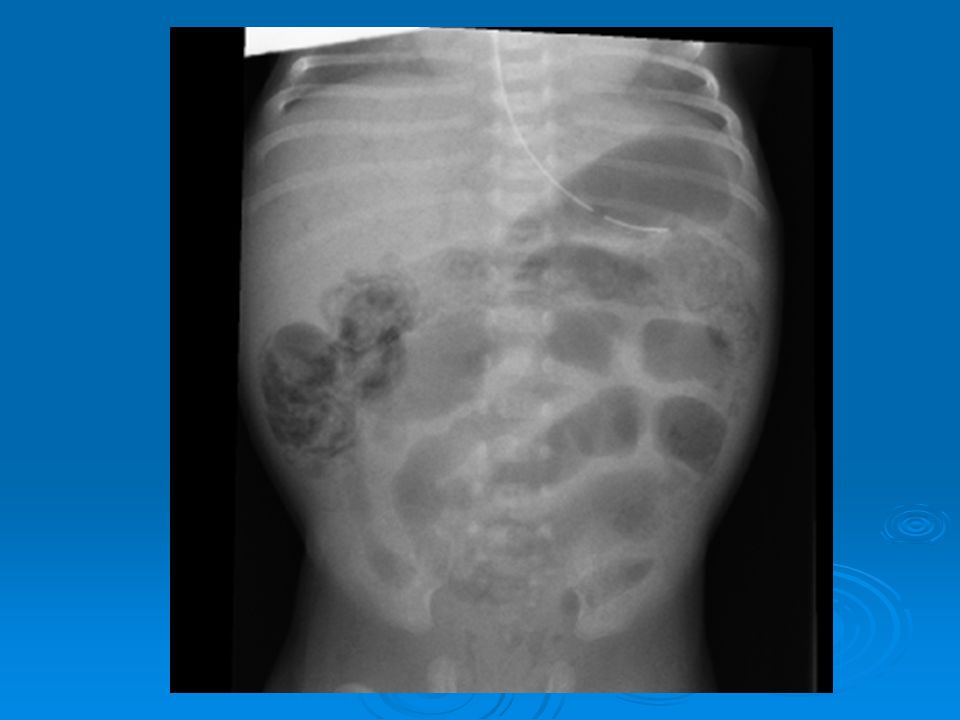
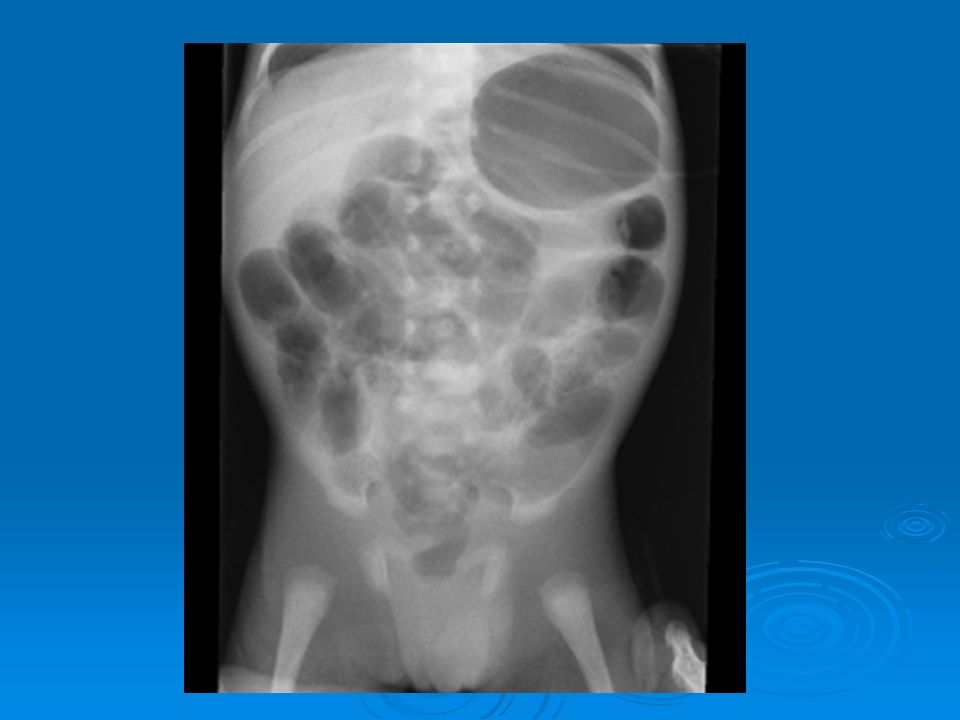
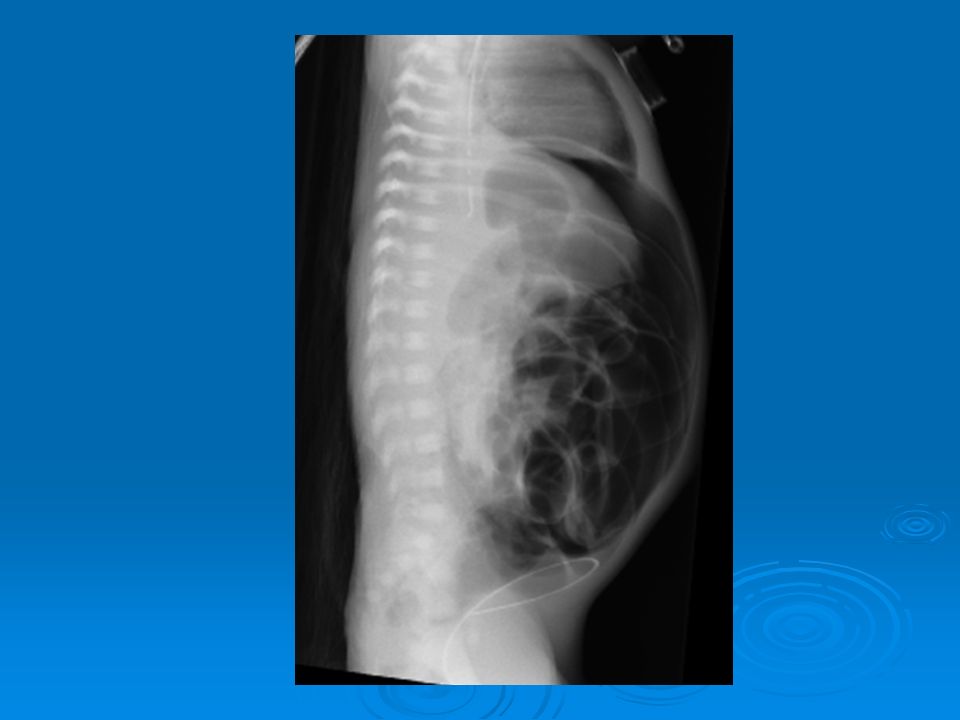
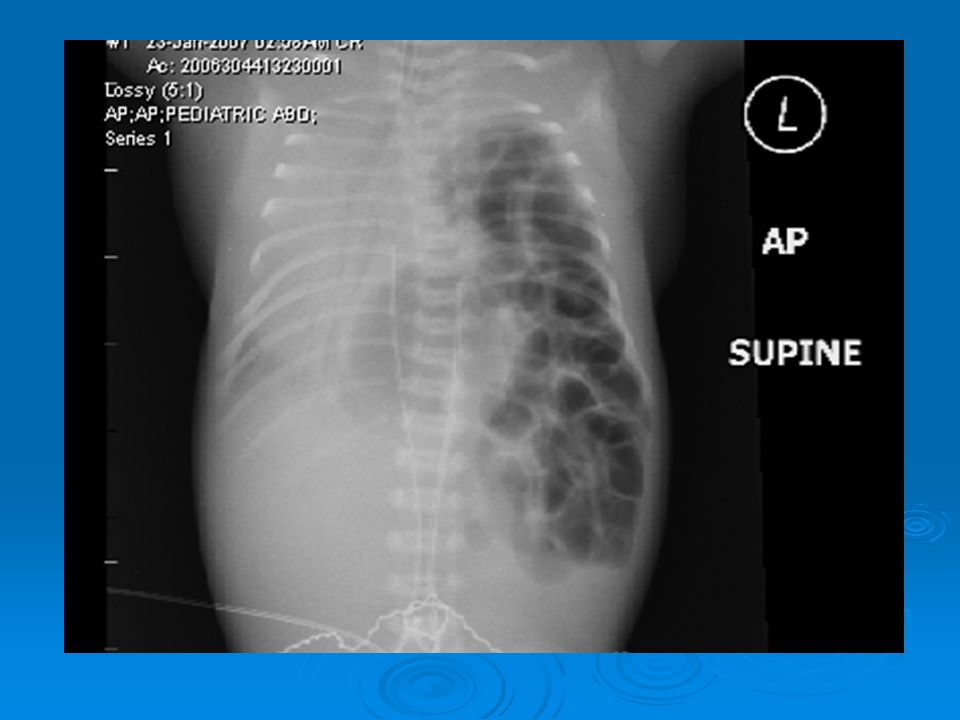
122
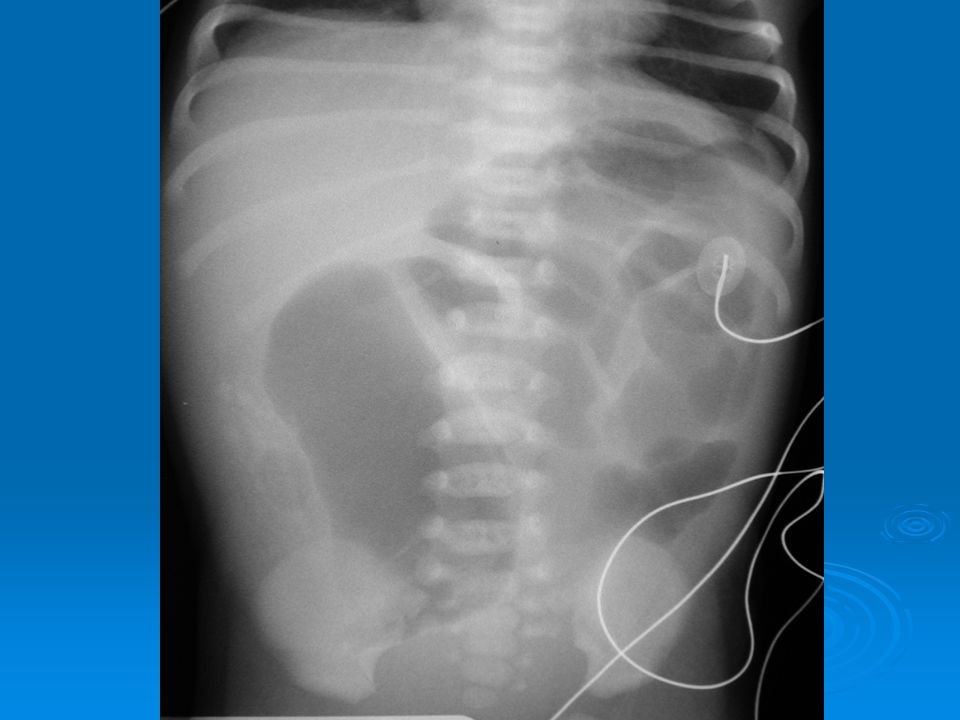
Lower GI Obstruction Presents with: Distention Distention Failure to pass meconium Failure to pass meconium Vomiting is a later sign Vomiting is a later sign Extrinsic vs intrinsic obstruction DDx: Imperforate anus, Hirschprung, meconium ileus, meconium plug, ileal atresia, colonic atresia

126
Constipation > 90% pass meconium in first 24 h If ‘constipation’ is present from birth: Consider causes of GI obstruction Consider causes of GI obstruction If present after birth: Consider Hirschprungs, hypothyroidism, anal stenosis Consider Hirschprungs, hypothyroidism, anal stenosis NB: Some breastfed babies normally stool only once every 5-7 days Some breastfed babies normally stool only once every 5-7 days Premature infants often have delayed meconium passage Premature infants often have delayed meconium passage

127
Jaundice First 24 h or conjugated at ANY time = ALWAYS abN Etiology: Unconjugated 1. RBC destruction/hemolytic : Isoimmune, RBC membrane, enzymes, hgbinopathies Isoimmune, RBC membrane, enzymes, hgbinopathies Hematoma Hematoma Sepsis (mixed hemolytic and hepatocellular damage) Sepsis (mixed hemolytic and hepatocellular damage) Hypoxia Hypoxia 2. Conjugation Abnormalities: Breast Milk Jaundice Breast Milk Jaundice Metabolic/Genetic: Gilbert, Crigler-Najjar, Hypothyroidism Metabolic/Genetic: Gilbert, Crigler-Najjar, Hypothyroidism 3. Increased Enterohepatic Circulation: GI dysmotility or obstruction GI dysmotility or obstruction Breast feeding jaundice Breast feeding jaundice
 Sepsis (mixed hemolytic and hepatocellular damage) Hypoxia Hypoxia 2. Conjugation Abnormalities: Breast Milk Jaundice Breast Milk Jaundice Metabolic/Genetic: Gilbert, Crigler-Najjar, Hypothyroidism Metabolic/Genetic: Gilbert, Crigler-Najjar, Hypothyroidism 3. Increased Enterohepatic Circulation: GI dysmotility or obstruction GI dysmotility or obstruction Breast feeding jaundice Breast feeding jaundice.")
128
Later onset: Conjugated 1. Hepatocellular damage: Viral Viral Bacterial Bacterial Metabolic: TPN, CF, tyrosinemia, other Metabolic: TPN, CF, tyrosinemia, other 2. Post hepatic: Biliary atresia Biliary atresia Choledochal cyst Choledochal cyst Jaundice

129
Jaundice - Work-Up History and physical examination Bilirubin - total and direct Blood type and Coomb’s Hemoglobin Reticulocyte count Smear Septic workup +/- Abdominal Ultrasound +/- Metabolic, Viral workup

130
Risk factors for kernicterus Prematurity Hemolysis Asphyxia Acidosis Infection Cold stress Hypoglycemia

131
Treatment of Jaundice Nutrition/hydration Phototherapy Exchange transfusion

132
Anemia Hemorrhage Feto-maternal Feto-maternal Feto-placental Feto-placental Feto-fetal Feto-fetal Intracranial or extracranial Intracranial or extracranial Rupture of internal organs Rupture of internal organs Hemolysis Prematurity Treatment: Transfuse if necessary Transfuse if necessary

133
Endocrine Issues - Hypothyroidism Screen because too late for proper neurodevelopment if wait Signs: Poor feeding Poor feeding Constipation Constipation Prolonged jaundice Prolonged jaundice Large fontanelles Large fontanelles Umbilical hernia Umbilical hernia Dry skin Dry skin

135
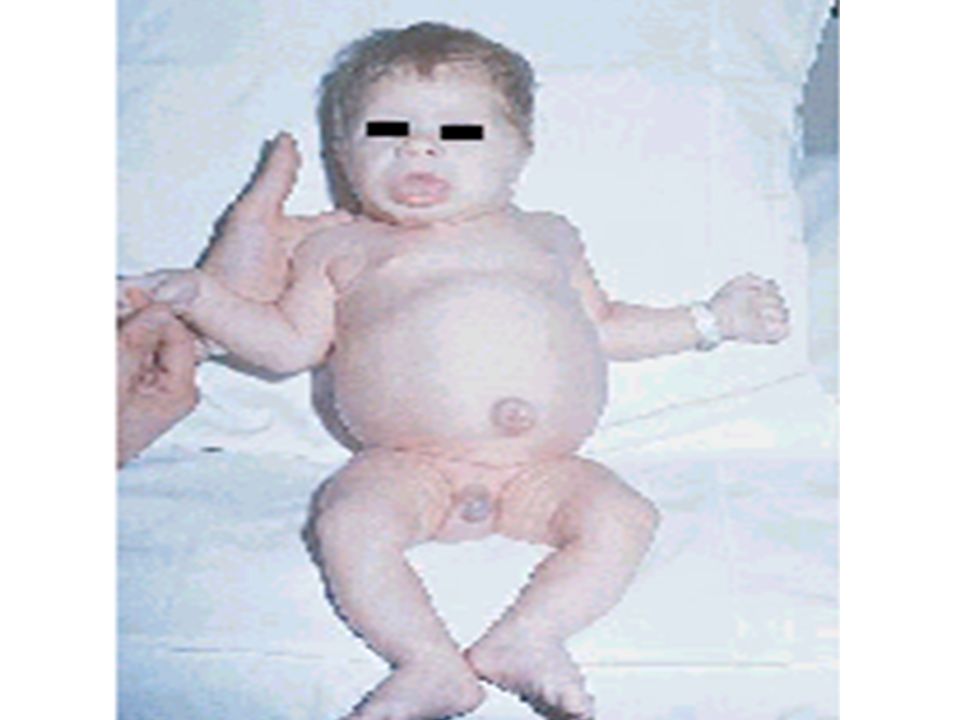
Endocrine Issues – Ambiguous Genitalia Congenital adrenal hyperplasia 21-hydroxylase deficiency = most common enzyme abN 21-hydroxylase deficiency = most common enzyme abN Signs = vomiting, diarrhea, dehydration, shock, convulsions, clitoris or phallic enlargement Signs = vomiting, diarrhea, dehydration, shock, convulsions, clitoris or phallic enlargement Watch for electrolyte imbalances Watch for electrolyte imbalances If suspect, send lab tests and treat with steroids If suspect, send lab tests and treat with steroids

137
Endocrine Issues – Infant of a Mom with Diabetes Increased Risk of: Congenital malformations Congenital malformations Increased incidence with poor glycemic controlIncreased incidence with poor glycemic control Growth disturbances Growth disturbances Metabolic disturbances Metabolic disturbances Hypoglycemia, hypocalcemiaHypoglycemia, hypocalcemia Respiratory: Respiratory: RDS, TTNRDS, TTN Hematologic: Hematologic: Polycythemia HyperbilirubinemiaPolycythemia Hyperbilirubinemia Cardiovascular problems: Cardiovascular problems: Hypertrophic cardiomyopathyHypertrophic cardiomyopathy

139
Hypoglycemia Definition: BS <2.6 prem and bottle fed term BS <2.6 prem and bottle fed term BS <2.0 breastfed BS <2.0 breastfed ** No clear safe cutoff for all ** No clear safe cutoff for all Pathophysiology: Lack of supply Lack of supply Lack of reserve (low glycogen): IUGR Lack of reserve (low glycogen): IUGR Inability to use/produce: metabolic Inability to use/produce: metabolic Increased utilization: sepsis Increased utilization: sepsis Increased insulin production Increased insulin production
: IUGR Lack of reserve (low glycogen): IUGR Inability to use/produce: metabolic Inability to use/produce: metabolic Increased utilization: sepsis Increased utilization: sepsis Increased insulin production Increased insulin production")
140
Hypoglycemia Treat by supplying glucose needs: Term: supply minimum of 4-6 mg/kg/min Term: supply minimum of 4-6 mg/kg/min Preterm: supply minimum of 6-8 mg/kg/min Preterm: supply minimum of 6-8 mg/kg/min Look for cause … if severe or persists beyond 48-72h of life ‘Critical Sample’ of blood and urine ‘Critical Sample’ of blood and urine

141
Neonatal seizures: Etiology

142
Thank you! Questions? gmoore@cheo.on.ca

143
N.B. These slides are all based on the LMCC website areas that related to my expertise and wasn’t covered by my pediatric or obstetric colleagues talks (e.g. Resp, Cardio, Development, Gen Paeds, MFM) Covered: 19-1, 31-2, 36-1, 37-2, 49-1, 64, 65, 74-1, 82, 107-3, 118-3
 Covered: 19-1, 31-2, 36-1, 37-2, 49-1, 64, 65, 74-1, 82, 107-3,")
Similar presentations