Download presentation
Presentation is loading. Please wait.

1
Health Equity Priyank Devta Deepa Patel Alicia Williams

2
Health Equity Health equity refers to the study of differences in the quality of health and health care across different populations. This may include differences in the presence of disease, health outcomes, or access to health care.

3
Health Equity Many different populations are affected by disparities, including: racial and ethnic minorities, residents of rural areas, women, children, the elderly, and persons with disabilities.

4
Assessing Racial and Ethnic Disparities in Health Care Alicia Williams 2012 PharmD Candidate Mercer University COPHS July 22, 2011

5
Overview Background The Commonwealth Fund 2001 Health Care Quality Survey 2010 National Healthcare Quality & Disparities Report Conclusion

6
Background

7
Cultural and socioeconomic factors affect each person’s health and their opportunities to receive the best possible health care. On a wide range of health care quality measures, minority Americans do not fare as well as whites.

8
Background In general, minorities tend to: have worse access to health care receive lower quality care when they are able to access it have worse health outcomes than non- Hispanic whites.

9
Background A recent report estimated that between 2003 and 2006, more than $200 billion could have been saved in direct medical care expenditures if racial and ethnic health disparities did not exist. The direct and indirect costs attributed to health disparities contribute to the growth of health care costs in national health care expenditures, which is one of the reasons Congress has undertaken health reform.

10
The Commonwealth Fund 2001 Health Care Quality Survey

11
Conducted from April 2001 to November 2001 Conducted by the Princeton Survey Research Associates Collected current information on the care experiences of patients of various racial and ethnic backgrounds Focused on 5 core health care quality measures Based on telephone interviews with 6,722 adults age 18 and older 3,488 whites; 1,153 Hispanics; 1,037 African Americans; and 669 Asian Americans

12
Health Care Quality Measures Patient-Physician Communication Cultural Competence in Health Care Services Quality of Clinical Care for Minority Populations Access to Health Care Health Insurance Coverage

13
Patient-Physician Communication

16
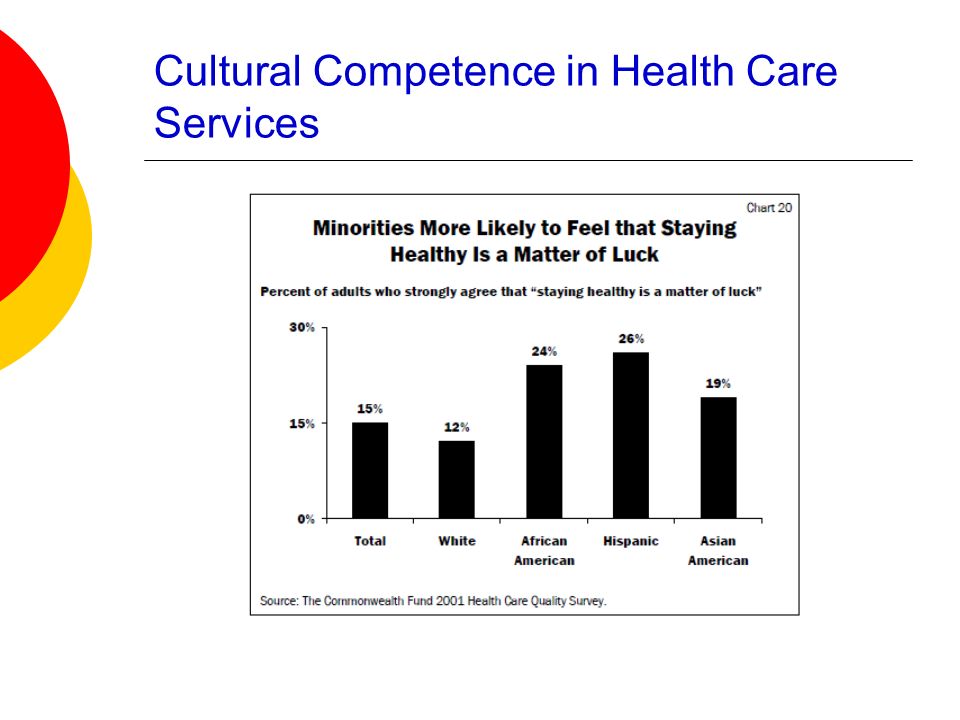
Cultural Competence in Health Care Services Defined as the incorporation of an awareness of health beliefs and behaviors, disease prevalence and incidence, and treatment outcomes for different patient populations.

17
Cultural Competence in Health Care Services

20
Compared with whites, minority respondents: feel less welcomed by the health care system, have more reservations about the benefits and value of health care, and are more likely to face significant language barriers.

21
Quality of Clinical Care for Minority Populations The survey assessed: preventive services and management of chronic diseases prevalence of medical errors sources of health information overall patient satisfaction

22
Quality of Clinical Care for Minority Populations

24
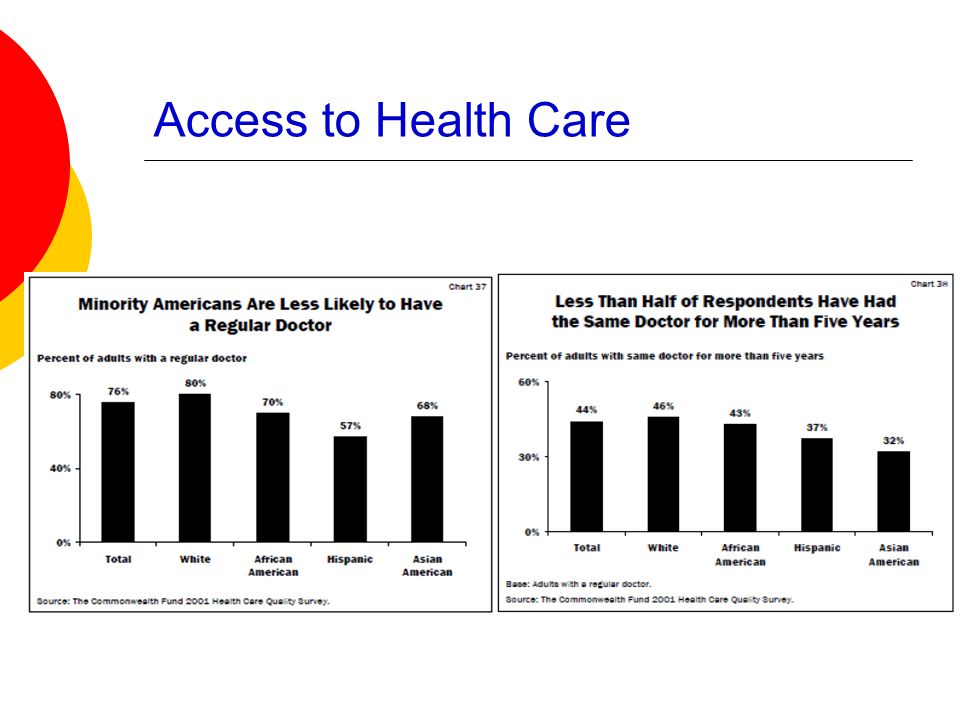
Access to Health Care Survey questions included asking U.S. adults about: their usual source of care, whether they have a regular doctor or a choice of providers, and continuity in their care

25
Access to Health Care

27
Minority adults are more likely to: receive care in hospital- or health center- based facilities. Minority adults are less likely to: have a regular doctor feel they have a choice in where they go for care have a long-term relationship with their doctor

28
Health Insurance Coverage Health insurance plays a critical role in: mediating access to medical care interactions with the health care system ensuring quality of care The uninsured fare worse than the insured on every measure of satisfaction and quality used. Although people of color represent one- third of the U.S. population, they comprise more than half of the uninsured.

29
Health Insurance Coverage

31
2010 National Healthcare Quality & Disparities Report

32
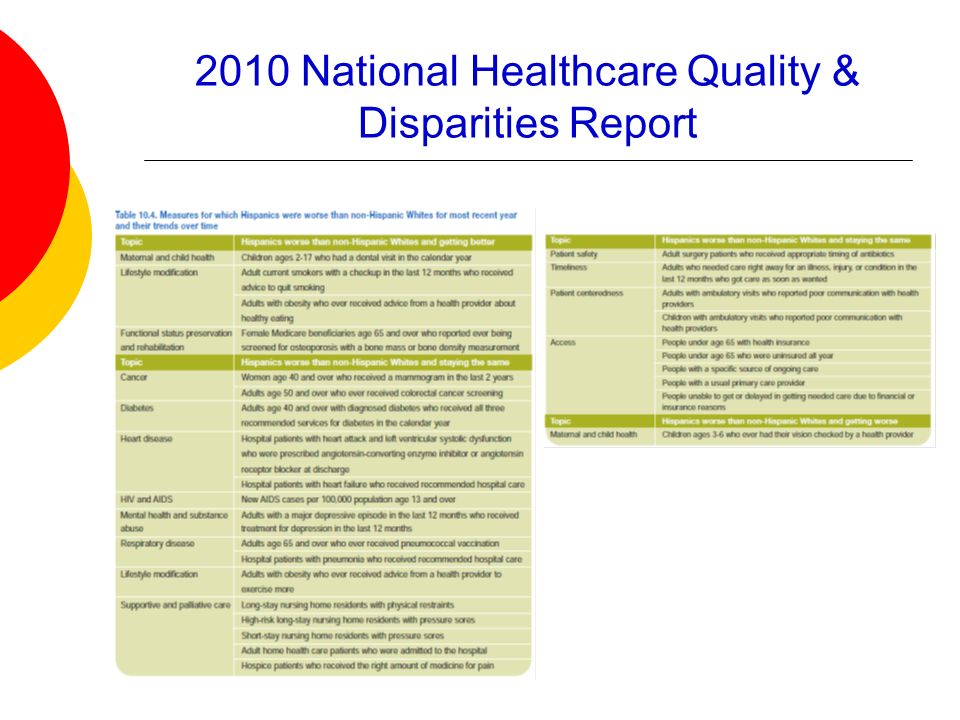
Produced by the Agency for Healthcare Research and Quality (AHRQ) Measures trends in effectiveness of care, patient safety, timeliness of care, patient centeredness, efficiency of care, and access to care in the general U.S. population The report is built on more than 250 measures categorized across these six dimensions.

33
2010 National Healthcare Quality & Disparities Report

37
Conclusion Gaps in health care quality between whites and people of color remain unchanged, and in some cases are getting wider.

38
Deepa Patel Doctor of Pharmacy Candidate, 2012 Mercer COPHS Presented on July 22, 2011

39
Disparities in healthcare by gender can be somewhat linked to the greater need for care throughout the lifespan of a female patient when compared to males Females have a greater need for reproductive and preventative care during their younger yours Females also have a greater need for treatment from numerous chronic disease states at an older age Nearly 80% of women have a usual primary care provider, whereas 72% of males do Females are more likely to be unable to receive or receiveddelayed medical care, dental care, or prescription medications

40
Studies indicate that patients are more receptive to communicating when they are able to relate to the information being presented Female physicians have demonstrated a greater skill of gathering subjective information from patients

41
2010 National Healthcare Quality and Disparities Report

42
Both genders had decreases in hospitalizations for lower extremity amputation from 2005 to 2007 Males, however, had twice as many admissions as women for diabetes

43
The number of female adult hemodialysis patients that were receiving adequate dialysis was higher than that of male adult hemodialysis patients Males are more likely to be registered on a kidney transplant waiting list

44
Leading cause of death Females had higher rates of inpatient heart attack mortality than men Rate of receipt of a fibrinolytic medication was higher in males than women Both male and female patients with heart failure were discharged with appropriate medications at a rate of 82%

45
HIV infection death rate for males was more than twice that of females (5.4 per 100,000 population versus 2.1)
")
46
3 rd most common cancer in adults Rate of advanced stage colorectal cancer in males are significantly higher than women The rate for both genders, however, is decreasing significantly

47
No differences in the treatment of hospitalized pneumonia patients Tuberculosis Both genders increased the percentage of patients who completed therapy Female patients were more likely to complete treatment when compared to males Females had lower rates of post operative respiratory failure, sepsis, and deaths following complications of care

48
Female patients are 11% more likely to receive treatment for a major depressive episode compared to male patients Males had suicide rates four times higher than females

49
Females are significantly less likely to complete substance abuse treatment, 41% compared to 47.1%

50
Pressure ulcers Both genders had decreases in short and long term stay incidence of ulcers Females were less likely to have either type Female patients were more likely to receive potentially inappropriate medications

51
MaleFemale Kidney transplant waiting list registration Inpatient myocardial infarctions Appropriate medication dispensed Completion of substance abuse treatment Diabetes Adequate dialysis in ESRD HIV Colorectal Cancer Tuberculosis Post operative respiratory failure Sepsis Deaths following complications of care Major Depressive Disorder Suicide Attempts Pressure Ulcers

52
Male patients are more likely to be uninsured Many associate the incidence of women having insurance coverage with increased ease of availability of programs such as Medicaid for children and prenatal care An argument can be formed that increased needs for healthcare in females makes having insurance a greater need than with male patients

53
March 2010: Two federal statutes colloquially referred to as “Health care reform” passed Patient Protection and Affordable Care Act Health Care and Education Reconciliation Act One of the main goals is to expand insurance coverage, particularly to low and moderate income and uninsured adults

54
In 2006 the state passed its health care insurance reform law Parallels goals with National Reform: State regulated minimum healthcare insurance coverage Free health care for residents below established income levels even if patient doesn’t qualify for Medicaid Reduce burden of EMTALA

55
“Have Gender Gaps in Insurance Coverage and Access to Care Narrowed under Health Reform? Findings from Massachusetts.” Cross sectional study based on surveys Observed differences pre health care reform (2006) and post reform (2009) in adults by gender Insurance coverage Access to health care Use of healthcare Affordability
 and post reform (2009) in adults by gender Insurance coverage Access to health care Use of healthcare Affordability.")
60
Overall, younger and older women continue to use more care than men under healthcare reform Despite increases in insurance coverage, women were still more likely to report unmet needs for health care and problems affording care than men Especially true in younger adults

61
Coverage does not always translate to access to healthcare and affordability of care Particularly in patients with greater healthcare needs, such as women of all age groups Despite mandated healthcare coverage, affordability is a major concern Preventative care coverage standards vary greatly amongst states

62
Medical home Priyank Devta Pharm D candidate 2012

63
Disparity and accessibility Disparity – the condition or fact of being unequal, as in age, rank or degree Many factors lead to differences in health care, especially with respect to aggregate measure of use These include different underlying rates of illness due to genetic predisposition, local environmental conditions, or lifestyle choices There are differences in the care-seeking behavior of patients, which vary due to differing cultural beliefs, linguistic barriers, degree of trust of health care providers, or variations in the predisposition to seek timely care Availability of care is dependent upon such factors as the ability to pay for care, the location, management and delivery of health care services, clinical uncertainty, and health care practitioner beliefs

64
National Healthcare Disparities Report While disparities in health care potentially affect all Americans and individuals from any group, they are not uniformly distributed across populations Racial, ethnic, and socioeconomic disparities are national problems that affect health care at all points in the process, at all sites of care, and for all medical conditions Access to health care is prerequisite to obtaining quality care

65
Examples Minorities are more likely to be diagnosed with late stage breast cancer and colorectal cancer compared with whites Patients of lower socioeconomic position are less likely to receive recommended diabetic services and more likely to be hospitalized for diabetes and its complications When hospitalized for acute MI, Hispanics are less likely to receive optimal care Many racial and ethnic minorities and persons of lower socioeconomic position are more likely to die from HIV Minorities also account for a disproportionate share of new AIDS cases The use of physical restraints in nursing homes is higher among Hispanics and Asian/Pacific Islanders compared with non-Hispanic whites Blacks and poorer populations have higher rates of avoidable hospital admissions (conditions that rarely require hospitalization in the presence of comprehensive primary care)
")
66
National Healthcare Disparities Report Health care disparities are costly Poorly managed care or missed diagnoses result in expensive and avoidable complications – lead to higher cost in future Personal cost of disparities can lead to significant morbidity, disability, and lost productivity at individual level At social level, distal costs follow from proximal opportunities that were missed

67
Examples Without screening, cancers may not be detected until they grow large or metastasize to distant sites and cause symptoms Such lat stage cancers are usually associated with more limited treatment options and poorer survival Minorities and persons of lower socioeconomic status are less likely to receive cancer screening services and more likely to have late stage cancer when the disease is diagnosed Persons with diabetes of lower socioeconomic position are less likely to receive recommended diabetic services and more likely to be hospitalized for diabetes and its complications less likely to receive recommended immunizations for influenza and pneumococcal pneumonia More likely to suffer worse quality of care for pneumonia Differential rates of hospitalization and vaccination present opportunities for provider based and community based interventions to reduce disparities

68
National Healthcare Disparity Report Access to healthcare is an important prerequisite to obtaining quality care Patients may perceive barriers to delay seeking needed care, resulting in presentation of illness at a later, less treatable stage of illness Of the major measure of access, the lack of health insurance has significant consequences When healthcare needs are not met by primary health care system, rates of avoidable admissions may rise

69
Examples Many racial and ethnic minorities and individuals of lower socioeconomic status are less likely to have a usual source of care Hispanics and people of lower socioeconomic status are more likely to report unmet health care needs While most of the population has health insurance, racial and ethnic minorities are less likely to report health insurance compared with whites Lower income persons are also less likely to report insurance compared with higher income persons Higher rates of avoidable admissions by blacks and lower socioeconomic position persons may be explained by lower receipt of routine care by these populations

70
National Healthcare Disparities Report Opportunities to provide preventive care are frequently missed Our healthcare system emphasize care that occurs after an illness occurs, rather than preventive services that could potentially prevent the illness or reduce the burden of disease Significant disparities in the use of evidence based preventive services for certain populations – smoking remains the single most preventable cause of mortality, rates of smoking cessation counseling during hospitalization are only 40%; 29% in blacks

71
Examples Blacks and people of lower socioeconomic status tend to have higher rates of death from cancer – early treatment of cancers can lead to reductions in mortality Less likely to receive screening and treatment for cardiac risk factors Less likely to receive childhood immunizations and recommended immunizations for influenza and pneumococcal disease

72
National Healthcare Disparities Report While blacks and poor patients are more likely to present with later stage cancers with higher death rates, black women have higher screening rates for cervical cancer and no evidence of later stage cervical cancer presentation. Significant investment in community based cancer screening and outreach programs for cervical cancer may be responsible for the lack of disparity Quality improvement efforts have resulted in demonstrable reductions in black-white differences in hemodialysis A greater perceived risk for significant cardiovascular disease among blacks may result in appropriately increased screening rates and treatment for risk factors

73
Accessibility of Health Care 2 choices of healthcare available: Government control of the medical system (socialized medicine as in Canada) which needs a lot of thought and consideration Private sector medical care system whose accountability remains more involved with its investors We have a split between private sector control (for those who can afford it) and public medical care system for those who can not (medicaid) Pharmaceutical companies claim that drug prices are higher because they need the money to continue researching new drugs for treatment Companies are businesses – have accountability is to stockholders and less to general public Government enact laws to prevent people from getting medications from cheaper sources like Canada which they claim is for benefit of American population instead of performing quality checks on the meds
 which needs a lot of thought and consideration Private sector medical care system whose accountability remains more involved with its investors We have a split between private sector control (for those who can afford it) and public medical care system for those who can not (medicaid) Pharmaceutical companies claim that drug prices are higher because they need the money to continue researching new drugs for treatment Companies are businesses – have accountability is to stockholders and less to general public Government enact laws to prevent people from getting medications from cheaper sources like Canada which they claim is for benefit of American population instead of performing quality checks on the meds")
74
Patient Centered Medical Home (PCMH) PCMH is an approach to providing comprehensive primary care for children, youth and adults PCMH is a health care setting that facilitates partnership between individual patients, and their personal physicians, and when appropriate, the patient’s family Principles to describe the characteristics of the PCMH have been developed by physicians
 PCMH is an approach to providing comprehensive primary care for children, youth and adults PCMH is a health care setting that facilitates partnership between individual patients, and their personal physicians, and when appropriate, the patient’s family Principles to describe the characteristics of the PCMH have been developed by physicians")
75
Principles Personal physician Physician directed medical practice – physician leads a team Whole person orientation – personal physician is responsible for providing referrals Care is coordinated and/or integrated across all elements of health care system (subspecialty care, hospitals, home health agencies, nursing home) and the patient’s community
 and the patient’s community")
76
Principles (cont.) Quality and safety – compassionate, robust partnership between physicians, patients, and the patient’s family; evidence based medicine, physicians accept accountability for continuous quality improvement, patients actively participate in decision making and feedback, information technology is used adequately, patients and family participate in quality improvement activities at the practice level Enhanced access – open scheduling, expanded hours, new options for communication
 Quality and safety – compassionate, robust partnership between physicians, patients, and the patient’s family; evidence based medicine, physicians accept accountability for continuous quality improvement, patients actively participate in decision making and feedback, information technology is used adequately, patients and family participate in quality improvement activities at the practice level Enhanced access – open scheduling, expanded hours, new options for communication")
77
Principles (cont.) Payment – should reflect the value of physician patient centered care management, should pay for coordination of care both within a given practice and between consultants, ancillary providers, and community resources, should support use of technology, allow for additional payments for achieving measurable and continuous quality improvements
 Payment – should reflect the value of physician patient centered care management, should pay for coordination of care both within a given practice and between consultants, ancillary providers, and community resources, should support use of technology, allow for additional payments for achieving measurable and continuous quality improvements")
78
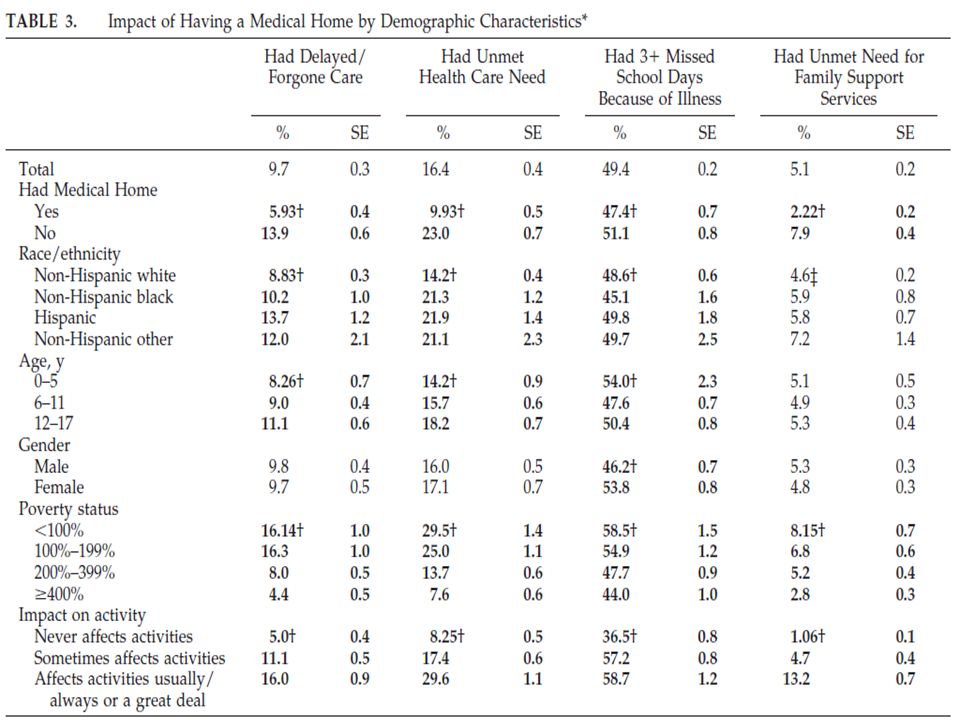
PCMH Table shows that most aspects of care and health outcomes, identification of a particular practitioner provides better services than mere identification of a particular place

79
PCMH Primary care-oriented countries (Denmark, Finland, Netherlands, Spain, UK) achieve notable better outcome for health in early childhood: low birth weight ratios, postneonatal mortality, infant mortality, and child mortality, including deaths from injury USA ranks near the bottom or at the bottom on all of these measures and is rated the lowest in primary care orientation of all the countries Advantages of primary care are most notable for health outcomes in childhood, although they are also marked for some health outcomes later in life
 achieve notable better outcome for health in early childhood: low birth weight ratios, postneonatal mortality, infant mortality, and child mortality, including deaths from injury USA ranks near the bottom or at the bottom on all of these measures and is rated the lowest in primary care orientation of all the countries Advantages of primary care are most notable for health outcomes in childhood, although they are also marked for some health outcomes later in life")
80
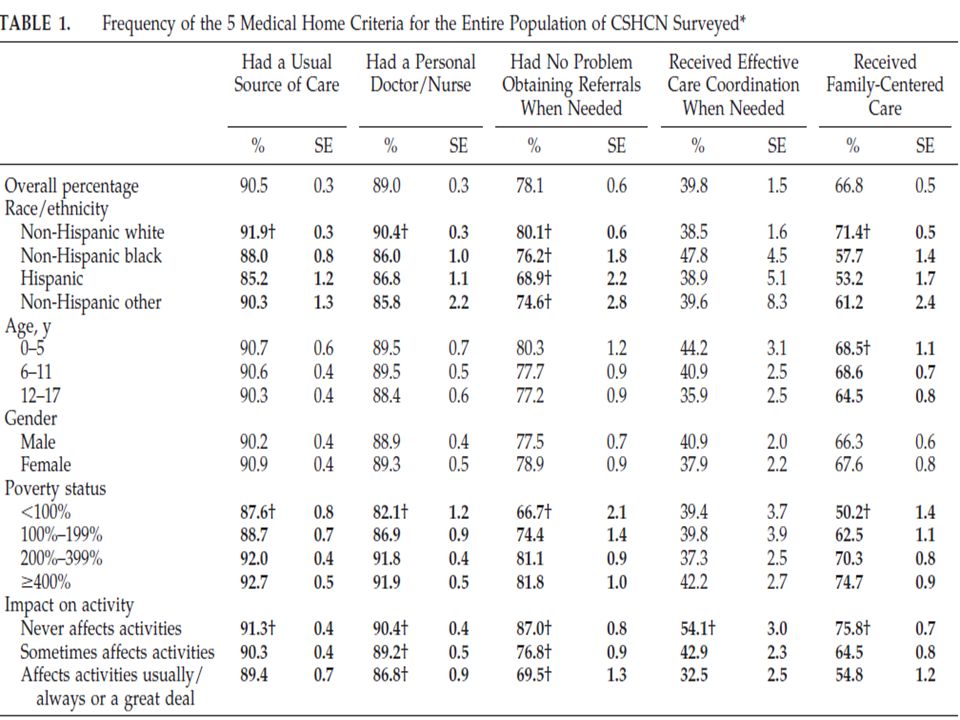
Results Article reports the findings of the National Survey of Children with Special Health care Needs regarding parent perception of the extent to which children with special health care needs(CSHCN) have access to a medical home 5 criteria to qualify as medical home – usual source of care, personal doctor or nurse, referrals for specialty care, coordinated care, family centered care prevalence of CSHCN in 2001 is 12.8% nationally Among CSHCN 52.6% had access to a medical home 90.5% of CSHCN had a usual source care Percentage of CSHCN who had usual source of care decreased as poverty level increased, 92.7% for nonpoor children to 87.6% for poor children 91.9% of non hispanic white children had a usual source of care, 85.2% of hispanics and 88% of AA
 have access to a medical home 5 criteria to qualify as medical home – usual source of care, personal doctor or nurse, referrals for specialty care, coordinated care, family centered care prevalence of CSHCN in 2001 is 12.8% nationally Among CSHCN 52.6% had access to a medical home 90.5% of CSHCN had a usual source care Percentage of CSHCN who had usual source of care decreased as poverty level increased, 92.7% for nonpoor children to 87.6% for poor children 91.9% of non hispanic white children had a usual source of care, 85.2% of hispanics and 88% of AA")
81
Results 11% of CSHCN did not have a personal doctor This number increased as poverty increased 82.1% of poor children compared to 91.1% of non poor children had a personal doctor or a nurse 90.4% of whites had personal doctor or nurse compared to 86% AA and 86.8% of hispanics

82
Results 78.1% reported having no difficulty getting needed referrals for specialty care 66.7% poor children had no difficulty compared to 81.8% of non poor children 80.1% white had no difficulty compared to 68.9% Hispanics, 76.2% AA, 74.6% of other races had no difficulty

83
Results 11.7% of CSHCN reported the need for care coordination Care coordination was adequate for 39.8% Care coordination was not provided when needed in 18.1% Communication between doctors and other programs was reported as very good or excellent by only 37.1% of patients

84
Results 66.8% of parents reported that doctors provided all elements of family centered care 50.2% of poor children receiving family centered care, as opposed to 74.7% of non poor children

87
Conclusion For the 90% of CSHCN who have a usual source of care, that source of care was most often a doctor’s office, a setting usually associated with the comprehensive care component of a medical home Poor and non white people were far less likely to use a doctor’s office as their usual source of care mainly due to lack of access as a result of insurance and other financial barriers Sociocultural factors and preferences may also play a role in determining where people of non white background receive their routine health care

88
References Collins K, Hughes D, Doty M, et al. Diverse communities, common concerns: assessing health care quality for minority Americans. New York: Commonwealth Fund; 2002. AHRQ (Agency for Healthcare Research and Quality). 2010. National Healthcare Disparities Report. Rockville, MD: AHRQ. Kaiser Family Foundation. September 2010. Health Reform and Communities of Color: Implications for Racial and Ethnic Health Disparities. Menlo Park, CA: KFF
 National Healthcare Disparities Report. Rockville, MD: AHRQ. Kaiser Family Foundation. September Health Reform and Communities of Color: Implications for Racial and Ethnic Health Disparities. Menlo Park, CA: KFF.")
Similar presentations