Download presentation
Presentation is loading. Please wait.

1
IHS EHR Indian Health Service Electronic Health Record COMMUNITY HEALTH PROGRAMS Marge Koepping, RN, MN, FNP IHS Model Diabetes Education Program

2
Objectives Process changes Pros and Cons

3
Community Health Programs Diabetes Program Public Health Nursing Nutrition Program/WIC Community Health Representatives Maternal Child Health Community Wellness Team Behavioral Health / Social Worker

4
EHR & Community Health EHR oriented towards clinical encounters Community Health visits may be different: Field Visits Field Visits Group Visits: clinic and community Group Visits: clinic and community Social Services Social Services Case management / coordination of care Case management / coordination of care

5
Process Changes: All programs and providers need computer access. Field visits may require portability. Documenting group education/visits. Drop in visits vs scheduled visits. Entering newborns into RPMS.

6
Process Changes: Case Management - Chart Reviews Flow Sheets Protocols, Guidelines, Standing Orders Consult/Referral Process

7
Pros Faster Entry of Case Management Increased Visit Documentation Increased Communication Consults Between Departments Chart Reviews enhanced

8
Cons Group Visit Documentation Case Management Communication Increased Avenues of Referral Increased visit documentation time Drop in visit vs scheduled visit

9
Questions?

10
IHS EHR Indian Health Service Electronic Health Record Lab Betty Hewson, MLT

11
Objectives for this Session Finishing the Lab Order in RPMS Lab Only Visits Lab Process Changes Pros and Cons

12
Finishing the lab order…..

13
Check for Past, Present and Future Orders in RPMS DATE to begin review: TODAY// (FEB 01, 2005) Test Urgency Status Accession Test Urgency Status Accession -Lab Order # 1662 Provider: RUDD,STEPHEN M -Lab Order # 1662 Provider: RUDD,STEPHEN M BLOOD BLOOD GLUCOSE ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:44 GLUCOSE ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:44 Sign or Symptom: : ~For Test: GLUCOSE : ~For Test: GLUCOSE : ~DM II : ~DM II ALT ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:44 ALT ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:44 Sign or Symptom: -Lab Order # 1662 Provider: RUDD,STEPHEN M -Lab Order # 1662 Provider: RUDD,STEPHEN M BLOOD BLOOD HB AIC ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:44 HB AIC ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:44 Sign or Symptom: -Lab Order # 1662 Provider: RUDD,STEPHEN M -Lab Order # 1662 Provider: RUDD,STEPHEN M URINE, CLEAN CATCH URINE, CLEAN CATCH URINALYSIS ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:4 URINALYSIS ROUTINE Requested (SEND PATIENT) for: 02/01/2005@14:4 T+30//March 1, 2005
 Test Urgency Status Accession Test Urgency Status Accession -Lab Order # 1662 Provider: RUDD,STEPHEN M -Lab Order # 1662 Provider: RUDD,STEPHEN M BLOOD BLOOD GLUCOSE ROUTINE Requested (SEND PATIENT) for: GLUCOSE ROUTINE Requested (SEND PATIENT) for: Sign or Symptom: : ~For Test: GLUCOSE : ~For Test: GLUCOSE : ~DM II : ~DM II ALT ROUTINE Requested (SEND PATIENT) for: ALT ROUTINE Requested (SEND PATIENT) for: Sign or Symptom: -Lab Order # 1662 Provider: RUDD,STEPHEN M -Lab Order # 1662 Provider: RUDD,STEPHEN M BLOOD BLOOD HB AIC ROUTINE Requested (SEND PATIENT) for: HB AIC ROUTINE Requested (SEND PATIENT) for: Sign or Symptom: -Lab Order # 1662 Provider: RUDD,STEPHEN M -Lab Order # 1662 Provider: RUDD,STEPHEN M URINE, CLEAN CATCH URINE, CLEAN CATCH URINALYSIS ROUTINE Requested (SEND PATIENT) for: URINALYSIS ROUTINE Requested (SEND PATIENT) for: T+30//March 1, 2005")
14
Finishing the lab order in RPMS

16
Or …Look in EHR instead of RPMS

17
Lab Result in EHR

18
Lab Only Visits

19
Lab Process Changes How does the lab know when the pt is there? Service copy can be printed in lab when the order is signed Service copy can be printed in lab when the order is signed Patients bring a “token” to the window Patients bring a “token” to the window Lab Schedule can be monitored by the receptionist Lab Schedule can be monitored by the receptionist

21
Lab Process Changes How to handle add on labs How to communicate the “Signs and Symptoms” (lab pov) to the lab
 to the lab")
22
Pros & Cons Training Issues: Signs and symptoms aren’t always communicated to the lab Signs and symptoms aren’t always communicated to the lab Ordering provider name =Clinician who signs Ordering provider name =Clinician who signs Training the patients Training the patients

23
Questions

24
IHS EHR Indian Health Service Electronic Health Record Radiology Bonnie Baxter, RTR

25
Objectives for this Session Finishing the Radiology order in RPMS Process Changes Pros and Cons

26
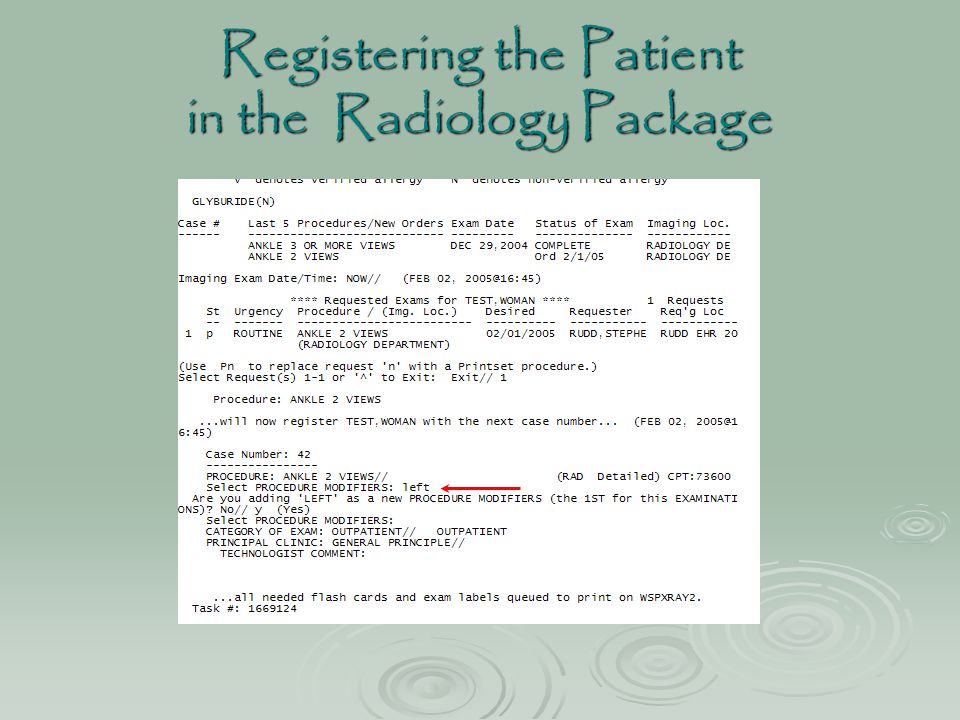
Registering the Patient in the Radiology Package

28
Entering the Exam

29
Radiology Reports in EHR

30
Process Changes Using RPMS Radiology Package Providers order the exam electronically Radiology orders print out automatically

31
Pros and Cons LMP? Modifiers?

32
Questions?

33
IHS EHR Indian Health Service Electronic Health Record Pharmacy LCDR Jim Gemelas, R.Ph. Chief Pharmacist

34
Objectives for this session Demonstrate how to finish a prescription order in RPMS Using EHR in the Pharmacy Process Changes Pros and Cons

35
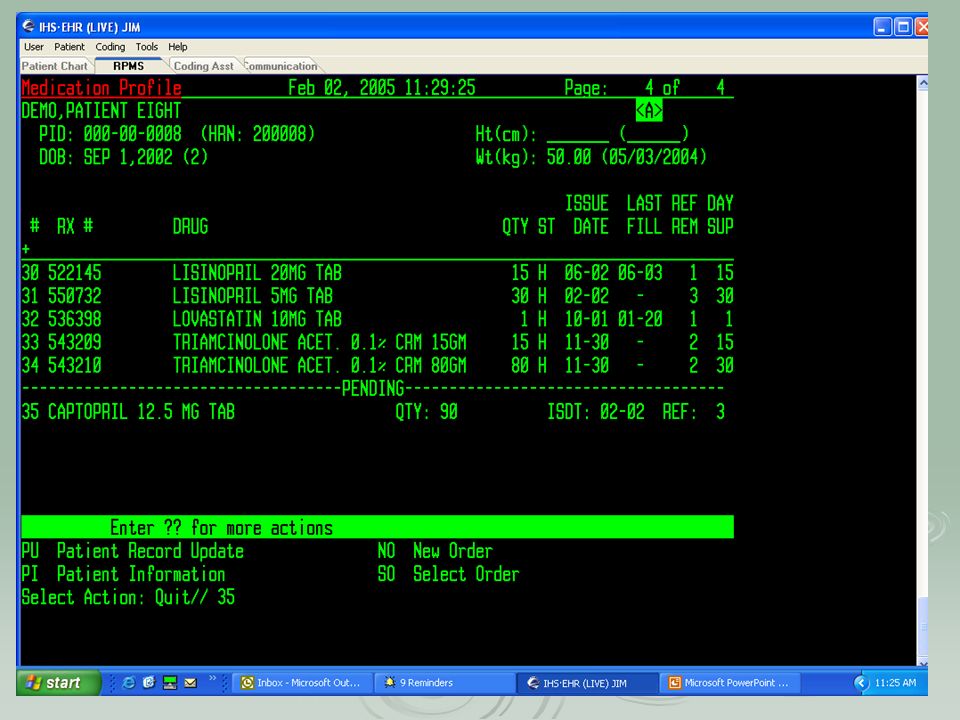
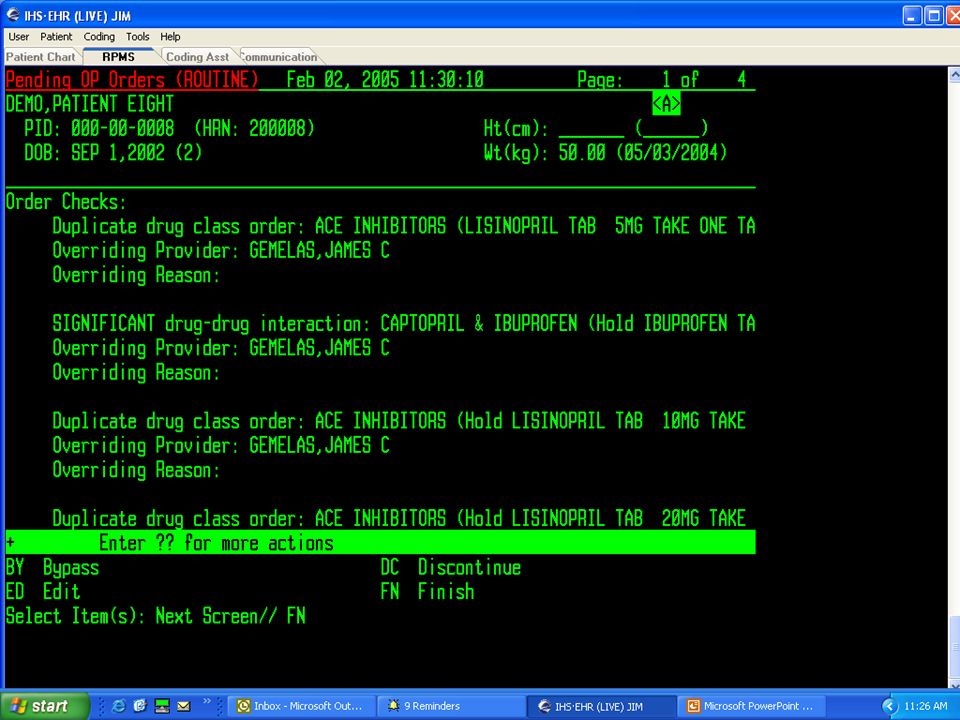
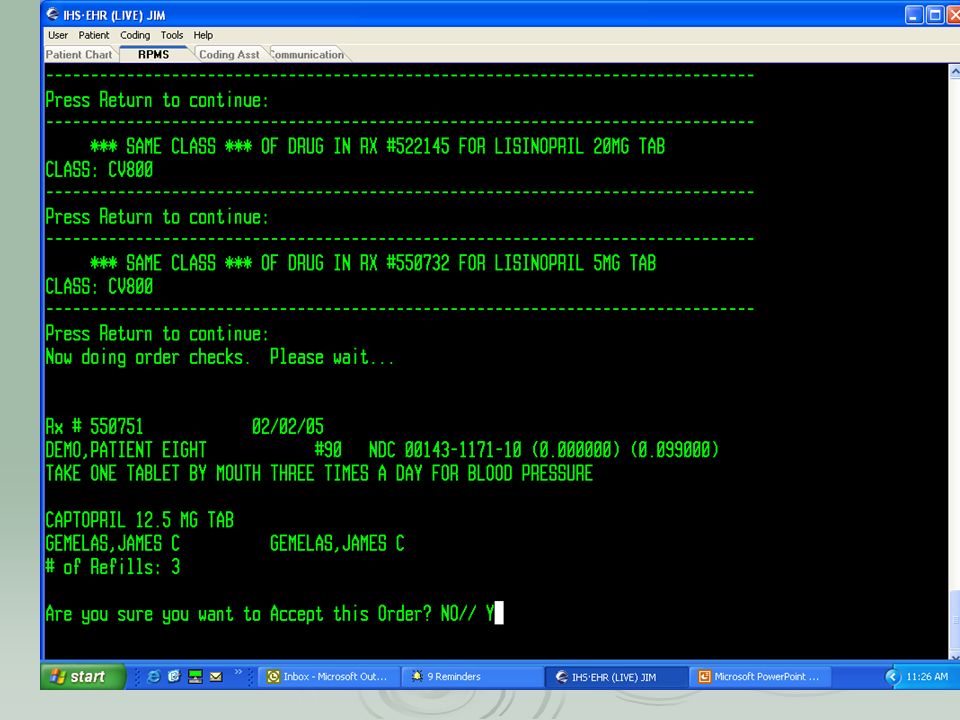
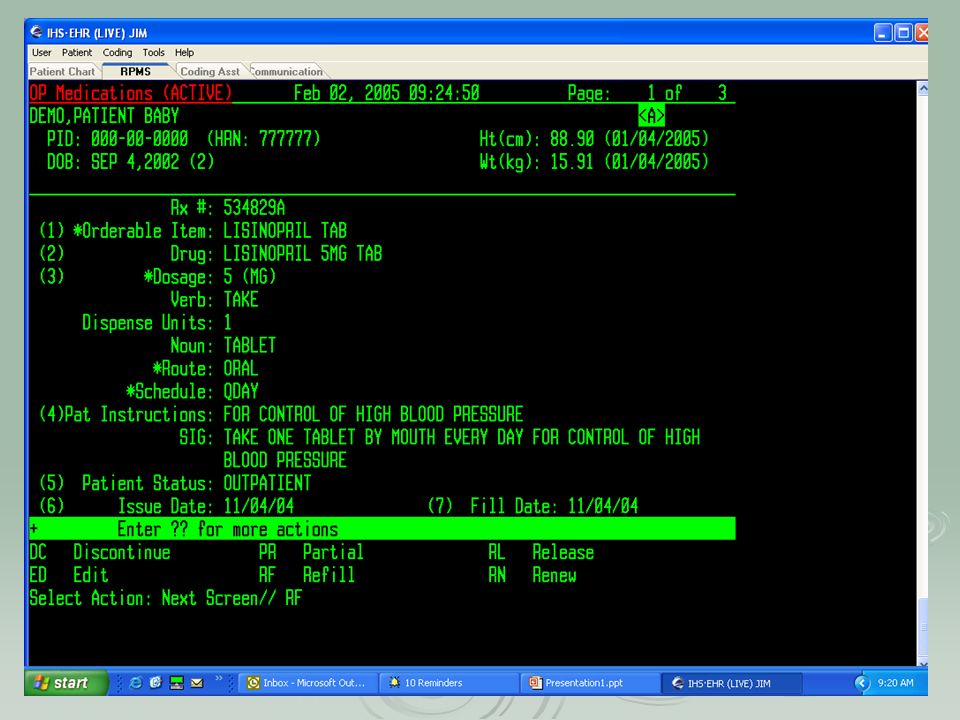
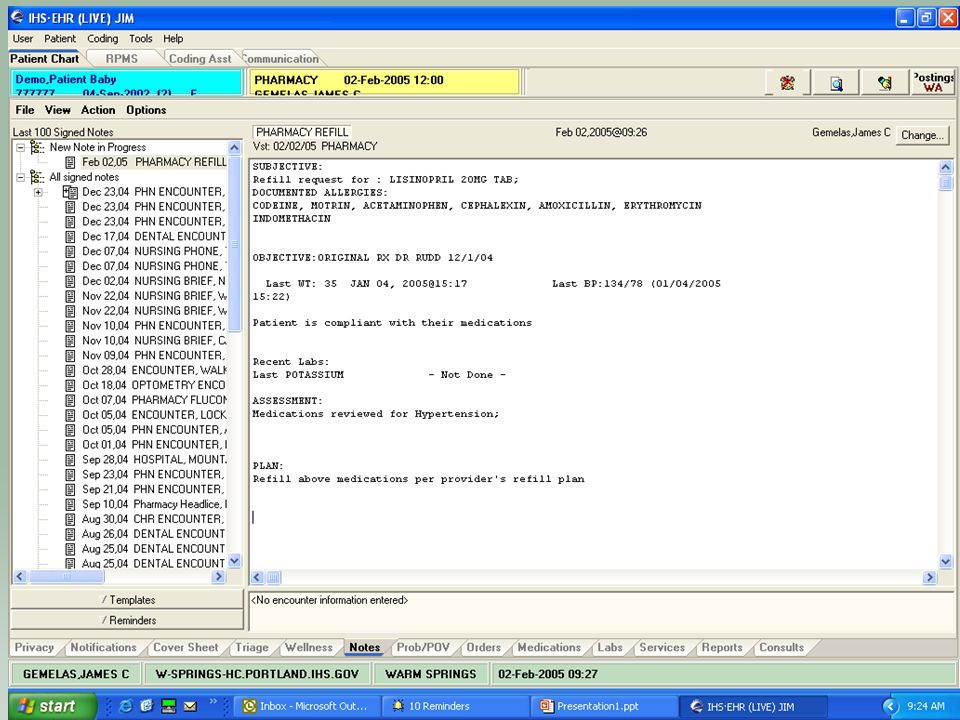
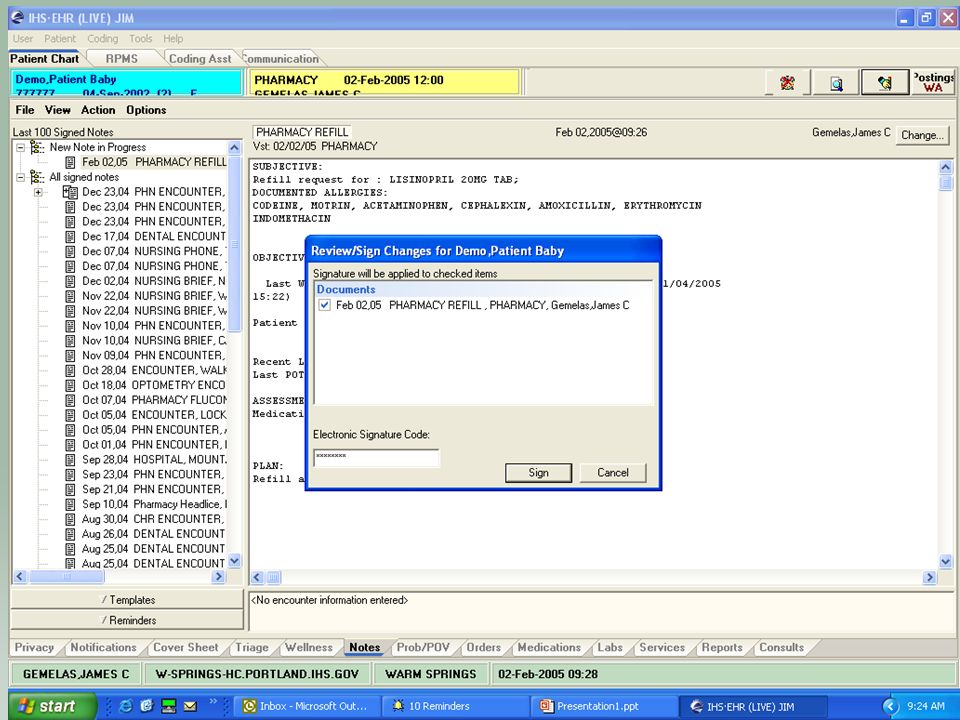
Finishing the Pharmacy Order in RPMS

36
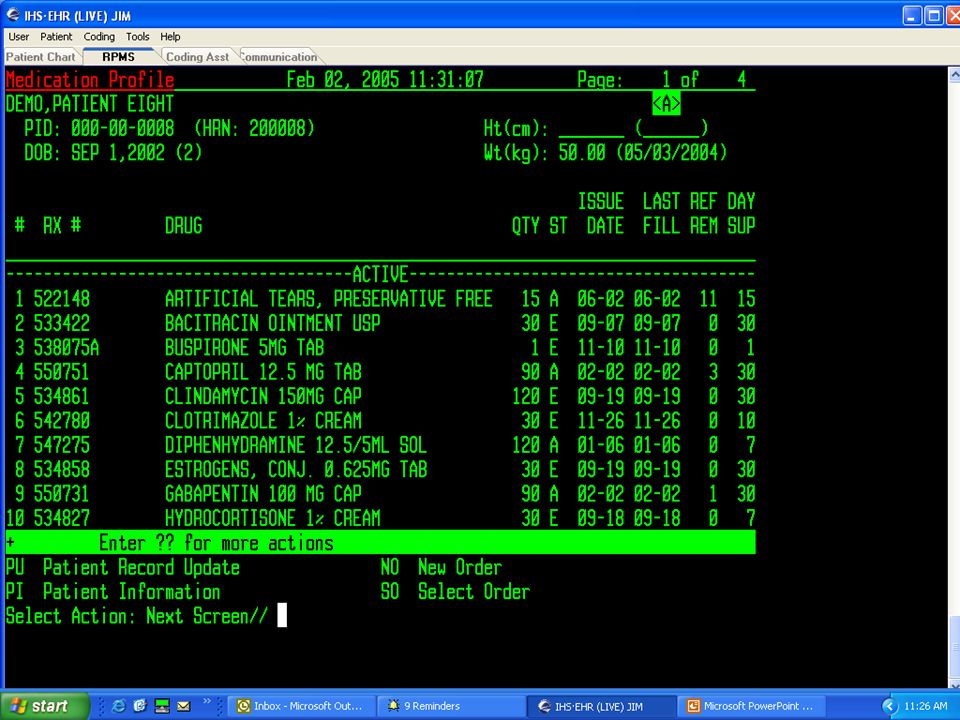
Order prints out in pharmacy and shows in RPMS

41
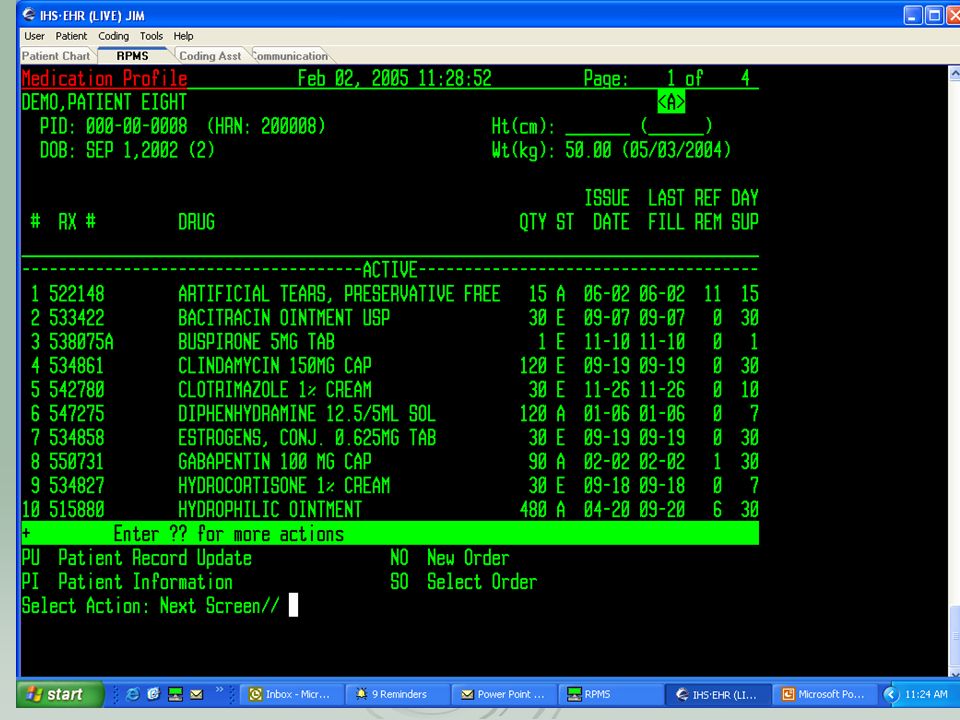
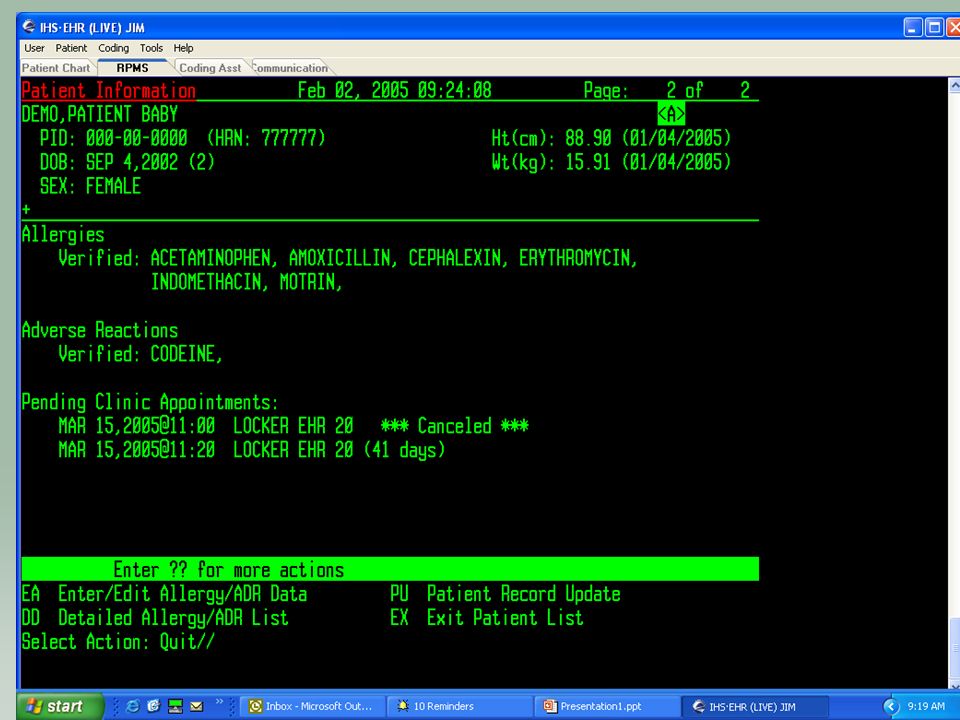
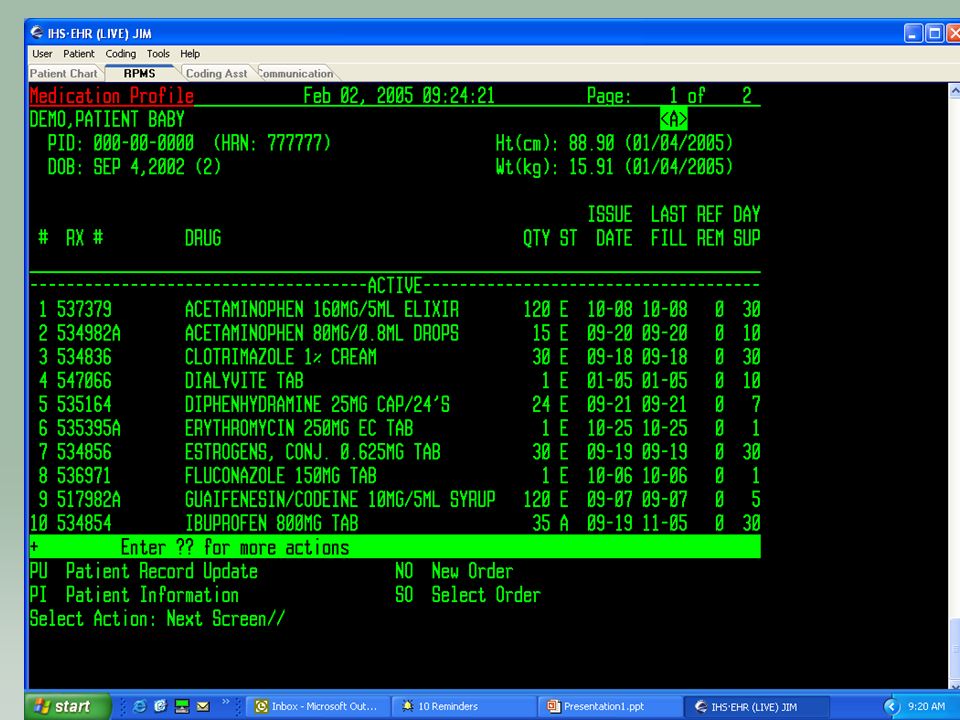
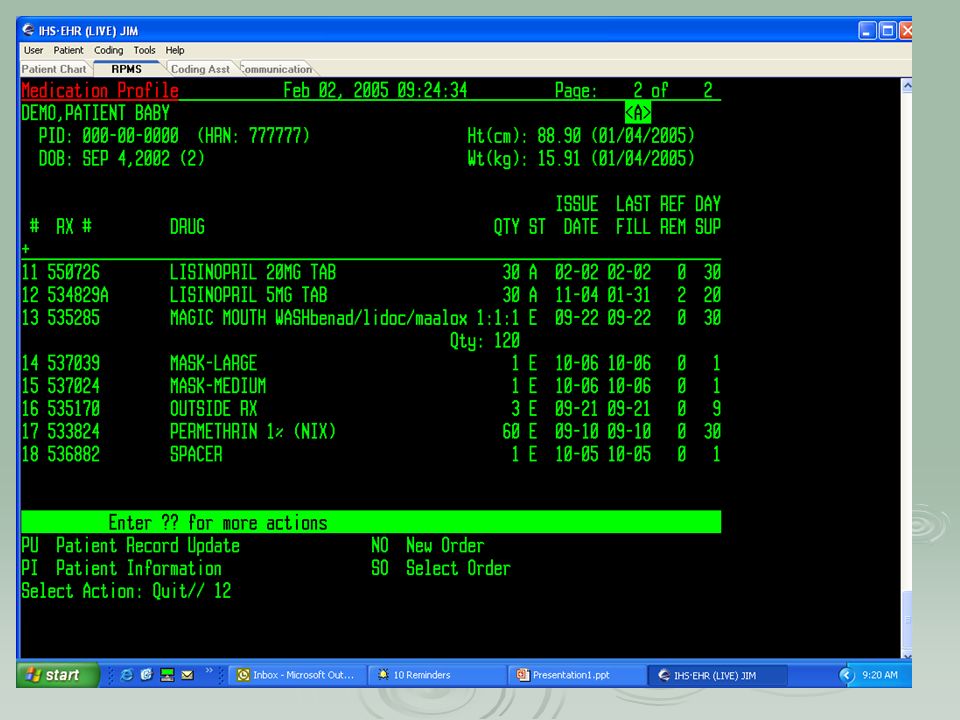
Stop-review provider note Provider note- toggle feature RPMS/EHR Review chart- IHS Pharmacy standards of practice Medication Profile Medication Profile Labs Labs

46
Document Patient Ed- Wellness Tab

47
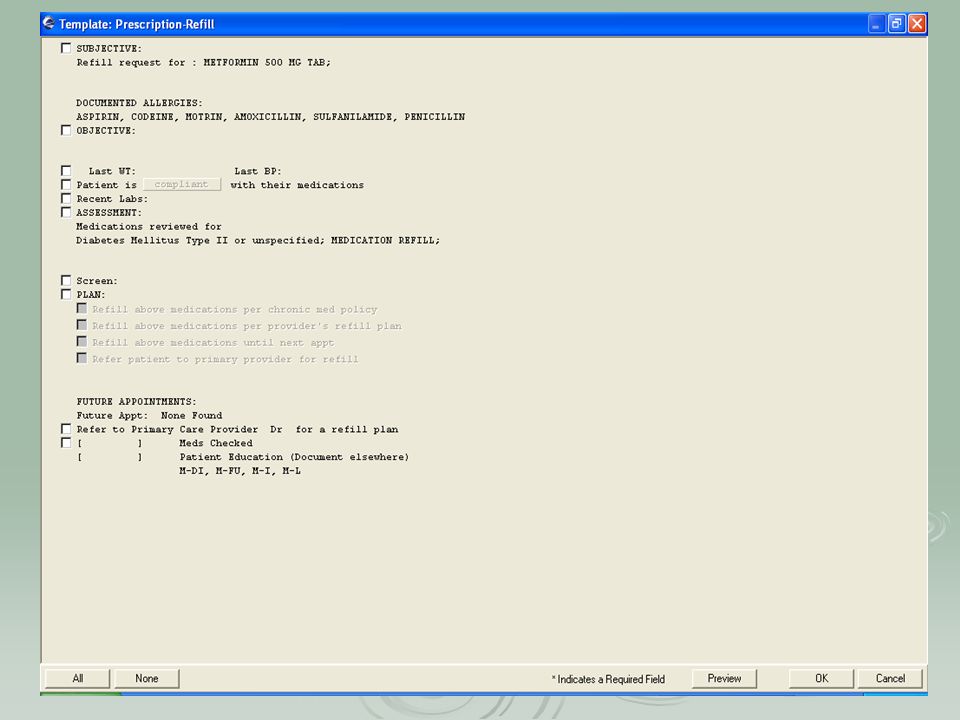
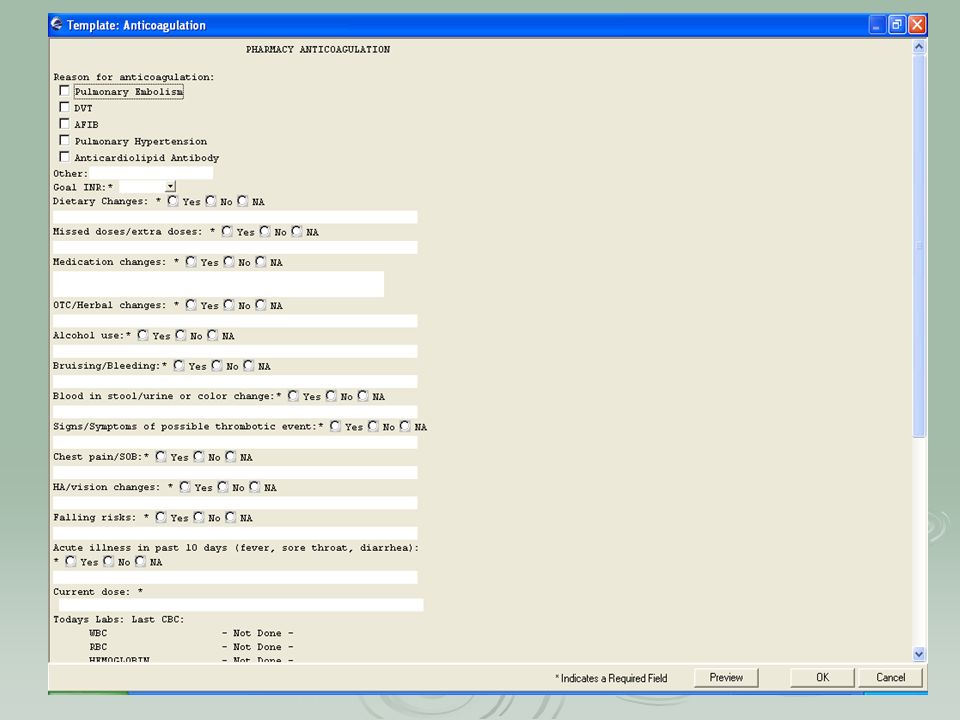
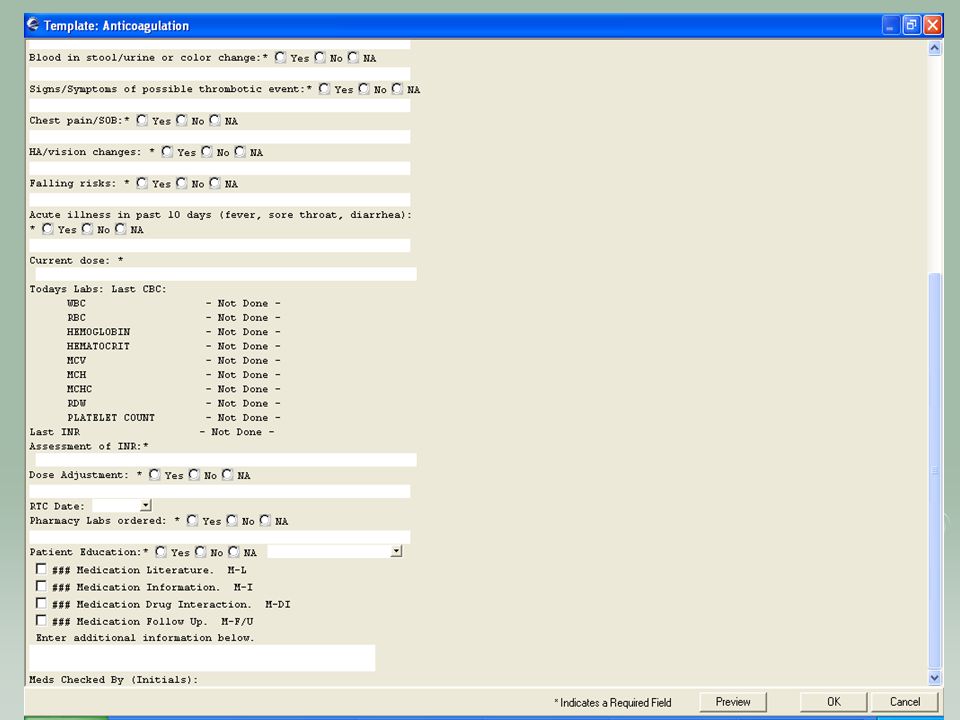
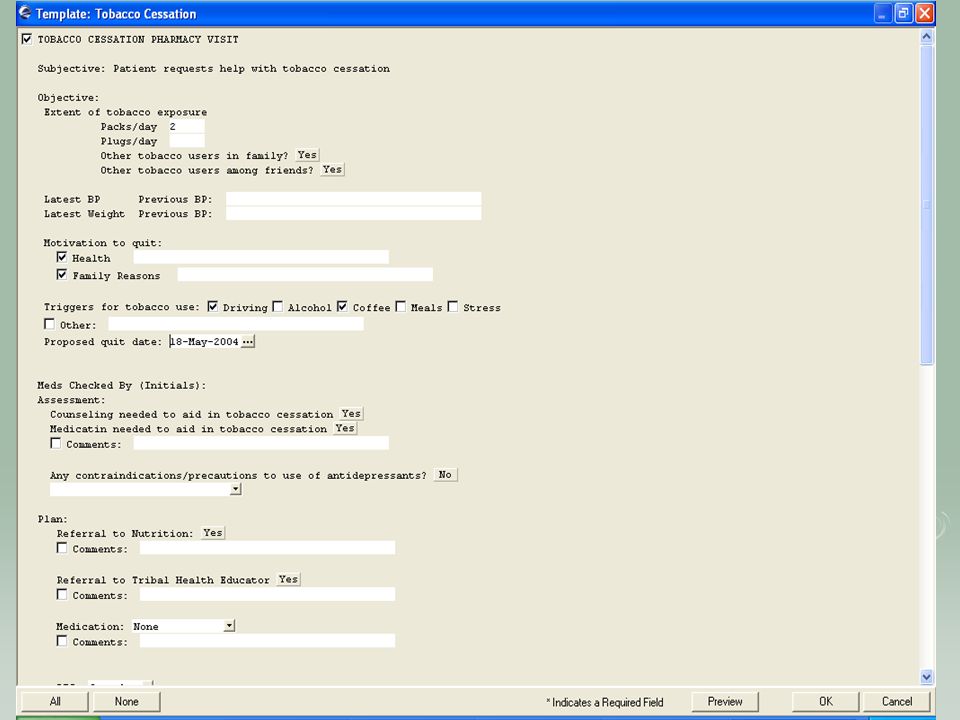
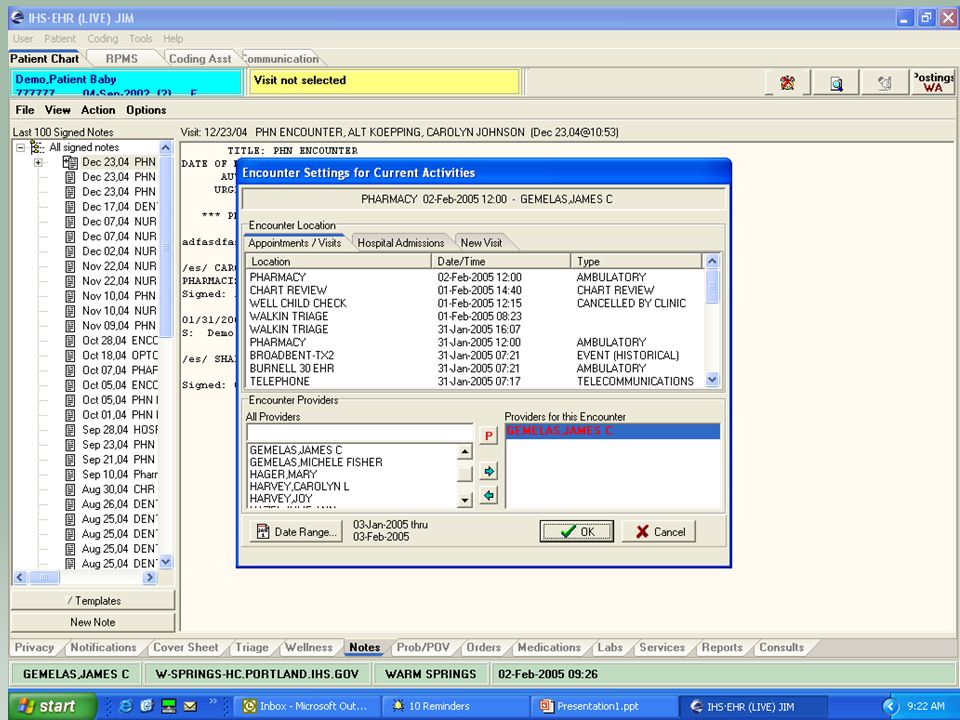
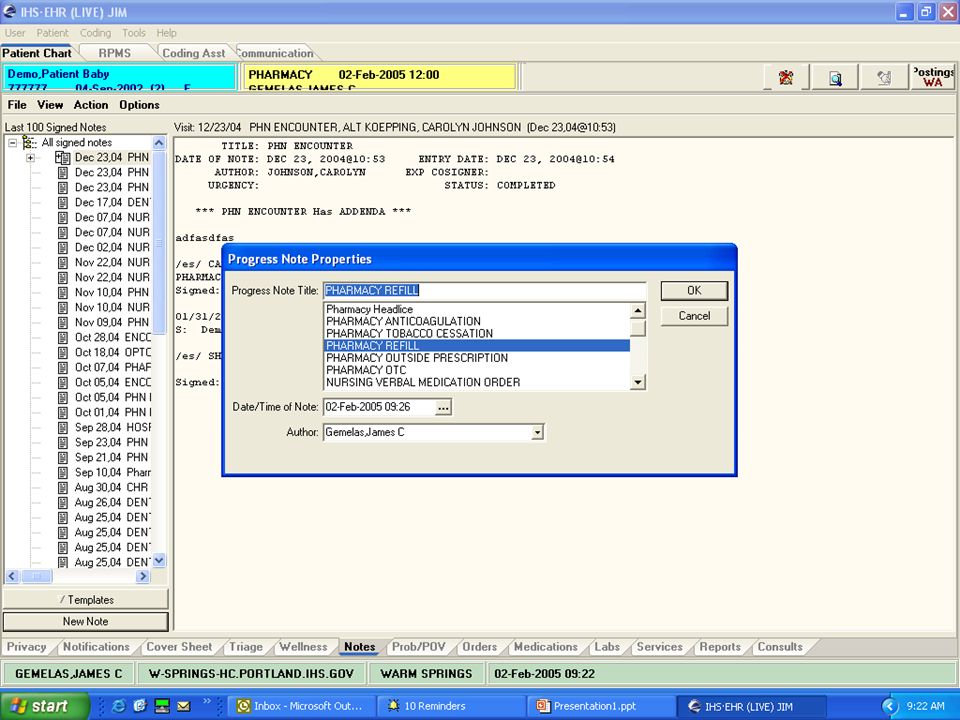
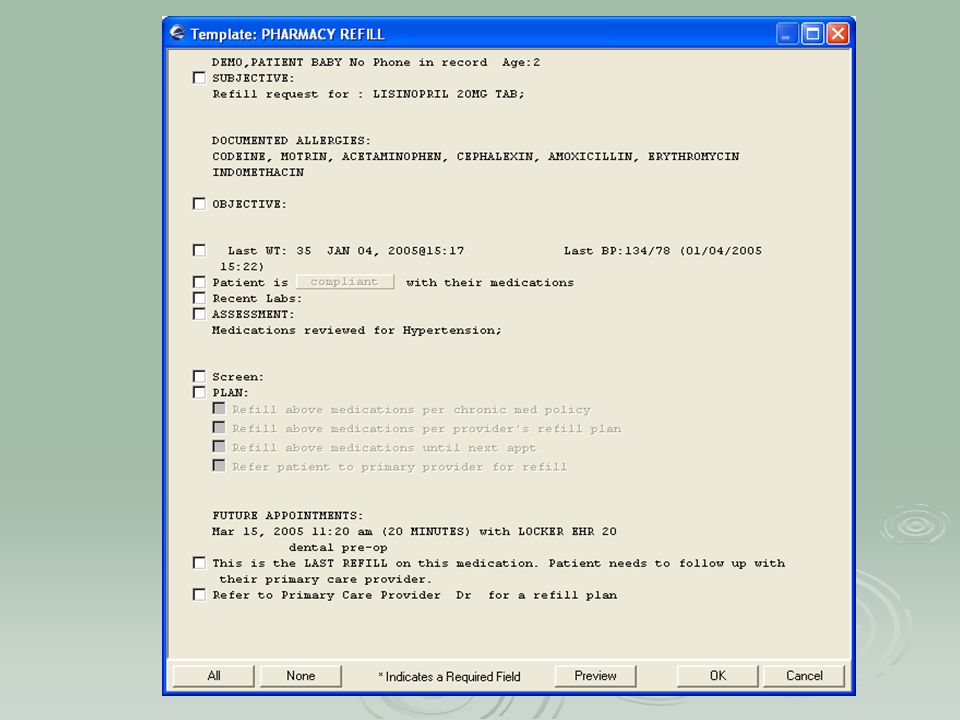
Using EHR in the Pharmacy Pharmacy Only Visits Refill template Anticoagulation template Outside Rx template Tobacco Cessation template

52
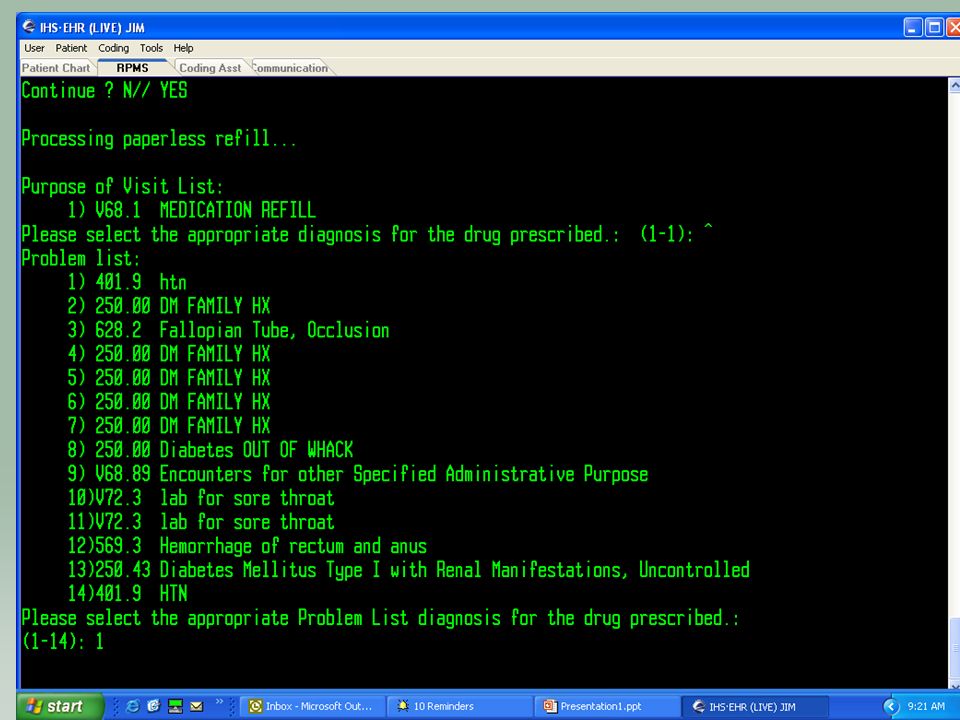
Paperless Refills

58
Pharmacist will use refill template

64
Pharmacy Process Changes Pharmacists Finish all new prescriptions Finish all new prescriptions All refills with a note Include screen captures All refills with a note Include screen captures Pharmacy Technicians No more data entry No more data entry Assemble and batch all prescriptions (ScriptPro) Assemble and batch all prescriptions (ScriptPro) Customer Service- phone calls, initial patient contact Customer Service- phone calls, initial patient contact Outside Prescription Orders Printing pharmacy service copies for orders Printing controlled substances How to incorporate pharmacy patient signature log Pharmacy Requirement for Completed/Signed Notes Pain contract
 Assemble and batch all prescriptions (ScriptPro) Customer Service- phone calls, initial patient contact Customer Service- phone calls, initial patient contact Outside Prescription Orders Printing pharmacy service copies for orders Printing controlled substances How to incorporate pharmacy patient signature log Pharmacy Requirement for Completed/Signed Notes Pain contract")
65
Where are the charts? “I don’t look back darling, it only distracts from the now!” …Edna Mode

66
Pharmacy Pros and Cons Dislikes- lots of preparation and teamwork! (this was a good process for the clinic! Tidal wave to smooth sailing) (this was a good process for the clinic! Tidal wave to smooth sailing) Providers finishing notes Providers finishing notes Dual system of charts and EHR Dual system of charts and EHR Chronic Medication List in EHR Chronic Medication List in EHR Likes No charts No charts Better documentation and clinical practice Better documentation and clinical practice Refill and New prescriptions aren’t always grouped
 (this was a good process for the clinic. Tidal wave to smooth sailing) Providers finishing notes Providers finishing notes Dual system of charts and EHR Dual system of charts and EHR Chronic Medication List in EHR Chronic Medication List in EHR Likes No charts No charts Better documentation and clinical practice Better documentation and clinical practice Refill and New prescriptions aren’t always grouped.")
67
IHS EHR Indian Health Service Electronic Health Record PCC/Coding Krisanne Billy

68
Objectives for this Session PCC Coding Process PCC Error Report Pros and Cons

69
PCC Coding Process Coding and Data entry is combined position at our facility Coders are assigned to provider teams Coding/Auditing from daily reports (VGEN and Audit Report) We code from EHR/RPMS not the chart Corrections communicated to provider via notification (demonstration)
 We code from EHR/RPMS not the chart Corrections communicated to provider via notification (demonstration)")
70
Demonstration

71
PCC Error Report Instead of 2 data entry clerks, we have 70 data entry providers who encode data Daily Error Reports should be run Most Common Errors: Missing POV Missing POV Missing E&M Code Missing E&M Code.9999 - Uncoded diagnosis.9999 - Uncoded diagnosis Duplicate Visits Duplicate Visits 2 visits created on the same day – have to be merged2 visits created on the same day – have to be merged Dental makes 2 visits that need to be mergedDental makes 2 visits that need to be merged Patch comingPatch coming

72
PCC-Business Office Communications Bills are generated before PCC has reviewed the visit

73
Pros & Cons Enjoy Paperless We don’t have to bring the chart to the provider to fix, we can communicate Incorrect Patient Selected-easier to fix Providers cant correct a code after the claim has been approved

74
Questions?

75
IHS EHR Indian Health Service Electronic Health Record Carolyn Johnson & Michele Miller Warm Springs Health & Wellness Center

76
Objectives Preparation & Implementation Cost Estimates

77
New Terminology POE – Provider Order Entry POE – Provider Order Entry CAC – Clinical Application Coordinator CAC – Clinical Application Coordinator GUI – Graphical User Interface GUI – Graphical User Interface OE/RR – Order Entry/Results Reporting OE/RR – Order Entry/Results Reporting CPRS – Computerized Patient Record System CPRS – Computerized Patient Record System VueCentric Framework VueCentric Framework Server side applications – roll and scroll; back end applications Server side applications – roll and scroll; back end applications PIMS – Patient Information Management System PIMS – Patient Information Management System TIU – Text Integration Utilities TIU – Text Integration Utilities Vista – Veterans Health Information System & Technology Architecture Vista – Veterans Health Information System & Technology Architecture

78
Preparation/Implementation

79
Implementation-Commitment Confirmed Leadership support Tribal Endorsement Area Office Support Patient Awareness Clinician driven

80
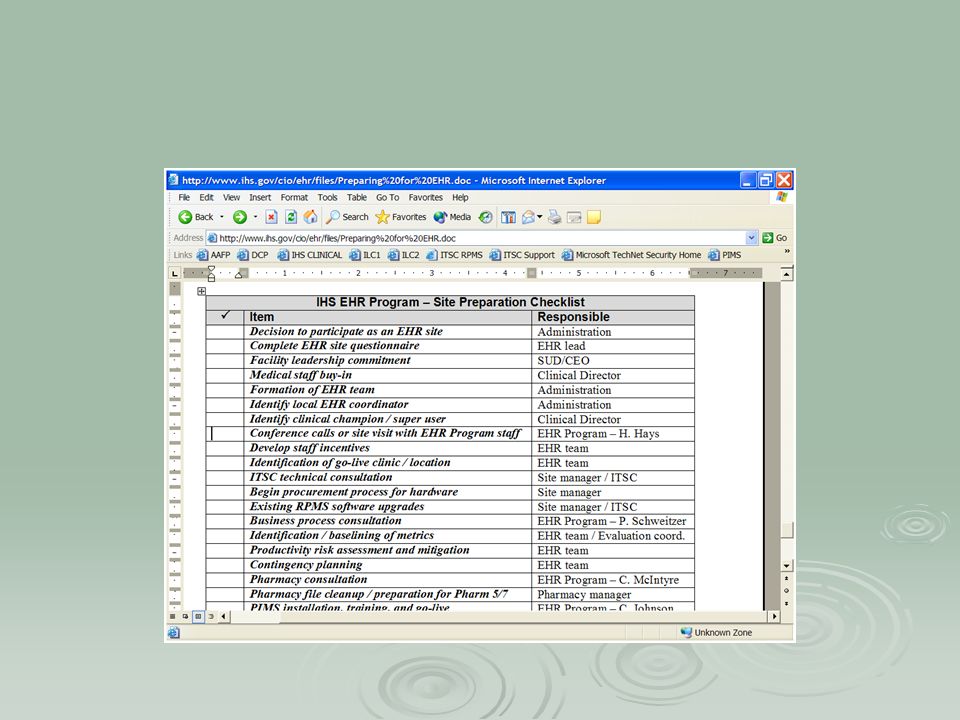
Software

81
Ballpark Timeline PIMS install Radiology 5.0 install – after PIMS EHR-Pharmacy 5/7 - needs to be scheduled Requires several months of preparation Requires several months of preparation Pharmacy needs to be used 3-6 months before implementing medication order entry. Pharmacy needs to be used 3-6 months before implementing medication order entry. Installation of GUI client – after Pharmacy EHR Set-up; Site visits - after Pharmacy Go-live – 3-6 months after Pharmacy

82
Pharmacy Preparation Adverse drug reactions :1 month RPMS/Scriptpro Format :1-2 days Dosages in Pharmacy 7: 1 week Quick orders : 1 week

83
Implementation- Hardware/Infrastructure upgrade RPMS server Training server Network Lab Interface Upgrade Workstation Access-Everywhere Backup Power

84
Implementation Team Members Clinical Champions from each discipline (lab,rn, rph,md,etc) Administration/Executive Leadership Information Technology Include Area IRM representation Clinical Application Coordinator
 Administration/Executive Leadership Information Technology Include Area IRM representation Clinical Application Coordinator")
85
Implementation Team Roles Identify and define Policies and Procedures Identify and define Policies and Procedures Address staffing and scheduling during transition Address staffing and scheduling during transition Peer Training & Marketing Peer Training & Marketing Monitor and Execute Implementation Plan Monitor and Execute Implementation Plan Design and Approve templates, menus, and ordering lists for E.H.R. Design and Approve templates, menus, and ordering lists for E.H.R.

86
Project Plan

88
Implementation Strategy Implementation-Who and When Everyone at once Lab ordering, then radiology ordering, then pharmacy ordering, then notes Bring up one team/dept at a time

89
Implementation Sample Schedule

90
Medical Clinic Preparations Formed Teams Practiced EHR (on paper) Defined Roles
 Defined Roles")
91
Lab Preparations All Labs need to be entered in RPMS On-site Labs On-site Labs Reference Labs Reference Labs State Labs State Labs Computer Access Points Changing from Esig to EHR

92
DM Program Preparations Have Good Templates for Diabetes Care Prompts for DM standards of care, DM audit, GPRA Prompts for DM standards of care, DM audit, GPRA Templates for DM ed assessment, Community BP/BS screening Templates for DM ed assessment, Community BP/BS screening Diabetes Program Referrals Review forms,flowsheets DM Curriculum flowsheet DM Curriculum flowsheet Case management review form Case management review form Education assessment form Education assessment form

93
Preparation-EHR Configuration Design templates Design Menus and Quick Orders Meds, Labs, Rad, Nursing Meds, Labs, Rad, Nursing Define consults Pick lists and Superbills Note Titles User Setup (keys) Parameters Printing Chart Copy and Orders Print Formats
 Parameters Printing Chart Copy and Orders Print Formats")
94
EHR beforeConfiguration EHR before Configuration

95
EHR after Configuration

96
Preparation-Setting up Orders

97
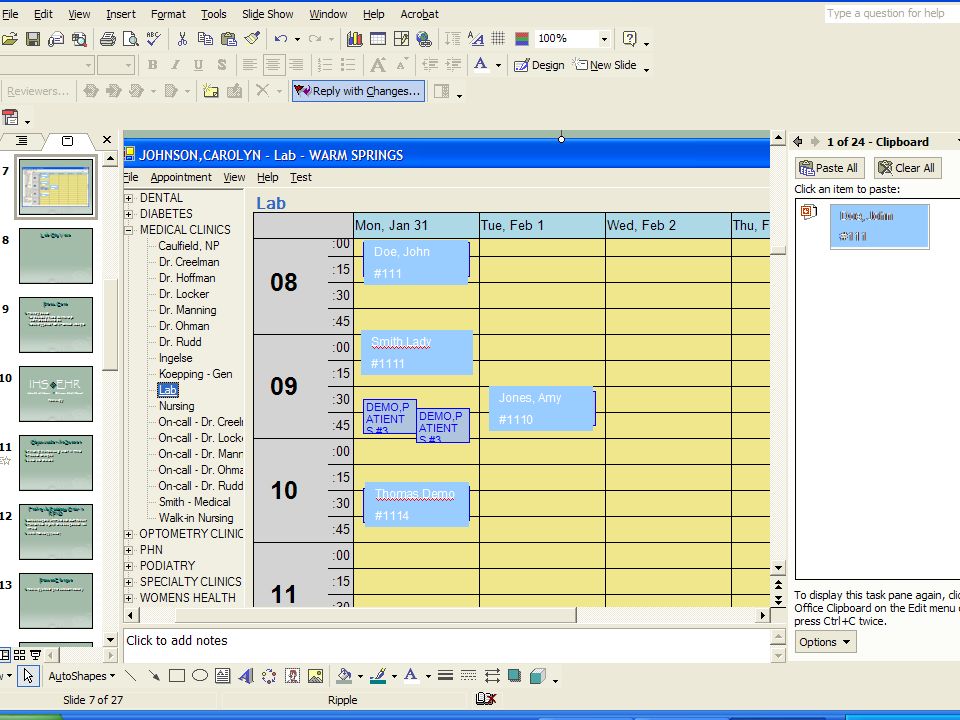
Lab Quick Orders

98
Preparation-Setting up templates

99
Training/Marketing Staff Training: EHR Demo Movie EHR Demo Movie Pharmacy Training Module: Pharmacy Training Module: CPRS Training Module: CPRS Training Module: National Programs Web-Ex Demo for our clinic National Programs Web-Ex Demo for our clinic

100
Pre-Implementation Training View Patient data in EHR Everyone got to Play Show and Tell Newsletters Newsletters Web Updates Web Updates Meeting Updates Meeting Updates

101
Training – Go Live Week 4-6 hours training outside of clinic Departmental Trainings Use Knowledgeable Trainers (IHS/VA) One-On-One Training Also Competency Checklists
 One-On-One Training Also Competency Checklists")
102
Going Live Week I can’t take it anymore!!

103
How the Week First Goes Growling at CAC’s Crying, gnashing of teeth Excited TGIF Cat in the microwave Excited

104
Going Live Intense CAC and IT Support Make Appropriate Scheduling Adjustments Daily Debriefings…. Procedural Questions Procedural Questions Technical Issues Technical Issues How did it work before EHR? How did it work before EHR? More Training More Training

105
Daily Debriefings MONDAY and TUESDAY of Go-Live Week Tom

107
Miscellaneous Policies/Procedures Use of personal templates Template approval process Use of chat and broadcast

108
Things to Think About Referral / Consults Patient Registration: Centralized / Decentralized People who aren’t using E.H.R. yet- how are they handled? Handle the missing PCC elements? SHX, colonscopy, refusal,mammogram (offsite)
.")
109
Medical Records Process When to stop pulling the chart Filing notes in chart? Print And File Chart Copies? Batch Print? Release Of Information? Outside Consults? Scanning? Incorrect Entries?

110
Impact on Staffing Provider support during implementation Staff shift from Medical Records to other departments : 2 Medical Records are in PCC part time 2 Medical Records are in PCC part time 1 Med rec tech is a nurses aid 1 Med rec tech is a nurses aid 1 Med rec tech is a Benefits Coordinator 1 Med rec tech is a Benefits Coordinator More nurses aids after EHR More nurses aids after EHR

111
Staffing-Clinical Applications Coordinator Duties Works cooperatively with Site Manager Coordinates Implementation EHR User Support Training Customize Software Workflow

114
What does EHR cost?

115
Cost Estimates-WSP

117
Questions?

118
Quality Improvement, Risk Management and Lessons Learned from EHR Michele Gemelas, R.Ph. QI/RM/GPRA Coordinator Warm Springs Health and Wellness Center

119
If there’s one thing we can say about EHR, it’s that it is an enormous, cataclysmic, earth shattering, life altering....

120
AWESOME CHANGE !!! Where the most trivial of things can become deadly projectiles

121
Decreasing the emotional impact of change Communication with providers and patients about any impending change will decrease the number of issues demanding attention during the change. Without communication about every important aspect of the change, expect to hear more from everyone who is affected by the change.

122
Pre-EHR –Communication Newspaper articles, radio interviews Flyers to hand out during implementation Facilitators and greeters Bulletin Boards For patients For patients For employees For employees

123
Why measure? Michele’s Top 4 #4: If you don’t know where you’re coming from, how will you know if you’ve gone anywhere? #3: To gain support for the change from those doing the changing (provide reinforcement) #2: So that you can say the change was bad and we need to re-design, or to rejoice because the change was good. And…the #1 reason to measure……….
 #2: So that you can say the change was bad and we need to re-design, or to rejoice because the change was good. And…the #1 reason to measure………..")
124
You need to monitor and maintain patient safety during implementation!!!!!

125
We can’t measure everything, so how do we select?

126
Consult all departments who will use EHR then: Create a list of meaningful measurements for each discipline Chose metrics based on everyday QI rules: high risk, high volume, problem prone Don’t reinvent the wheel,consult others that have gone before you Make staff part of this process!!!

127
Remember……. Sometimes, no change in pre- and post-EHR results equals success! Depends on where you started.

128
Subjective Measures/Metrics Staff satisfaction at various intervals after implementation Patient satisfaction based on survey Patient complaints/concerns

129
Objective Metrics Provider productivity – expect a dip, and plan for this in your staffing Medication errors – don’t expect improvement until all “old” errors have had time to surface. Compliance with health maintenance reminders (smoking, various cancer screens, etc.)
.")
130
Provider Productivity

131
Productivity Comparison

132
Pharmacy Medication Errors

133
Objective Metrics Error reports in PCC-expect an increase Coding – takes time to build the tools and convince providers to use them. Coding – takes time to build the tools and convince providers to use them. Missing E&M codes Missing E&M codes Missing POVs, Providers, Multiple providers Missing POVs, Providers, Multiple providers Data Entry backlog-expect it to increase Data Entry backlog-expect it to increase Billing backlog-due to data entry backlog Changes in revenue – patience…… Changes in revenue – patience……

134
Pages in the Error Report * Before 26-Apr-04

135
Things We Have Done Coding tools in EHR Links to coding sites, reference guides, E&M Coder Links to coding sites, reference guides, E&M Coder

136
Things We Have Done (cont.) Pick Lists ICD-9 ICD-9 Superbills Superbills
 Pick Lists ICD-9 ICD-9 Superbills Superbills")
137
Things We Have Done (cont.) Coding training for users (MD,RN,etc) Provider gets an automatic notification for the missing purpose of visit or E&M Code Quality Improvement Uncoded Diagnosis Uncoded Diagnosis Provider Audits Provider Audits Errors are communicated to provider via notifications
 Coding training for users (MD,RN,etc) Provider gets an automatic notification for the missing purpose of visit or E&M Code Quality Improvement Uncoded Diagnosis Uncoded Diagnosis Provider Audits Provider Audits Errors are communicated to provider via notifications")
138
Objective Metrics Time Study (before and after) Discipline specific peer review – use basic criteria to assure that patient care remains appropriate and that all correct data is gathered. GPRA performance – keep an eye on it, but expect results in 6 months to a year.

139
GPRA Indicators - Flu Vax

140
GPRA Indicators – Pneumovax over 65 y/o

141
GPRA Indicators – Tobacco Use Assessment

142
GPRA Indicators – DV/IPV

143
GPRA Indicator – BMI 2-74 y/o

144
GPRA Indicators – Med Ed

145
Other Improvments – Non-GPRA

146
DM audit impacts: PROVIDER ENTRY vs. CLERK DATA ENTRY affects the capture of some audit data: DM and Nutrition educationDM and Nutrition education ImmunizationsImmunizations Eye ExamsEye Exams Dental ExamsDental Exams Foot ExamsFoot Exams HISTORICAL & REFUSED EXAMS and IMMUNIZATIONS train providers/nurses to entertrain providers/nurses to enter review DMS taxonomy to ensure it recognizes both.review DMS taxonomy to ensure it recognizes both.

147
Diabetes QI : Aspirin Therapy EHR Implementation Begins

148
More QI: Diabetes Education Documentation by Provider EHR Implementation Begins

149
Diabetes QI: Annual Eye Exams EHR Implementation Begins

150
Risk Management

151
Every time a person is asked to change their role or a make a change in a process, there are inherent risks. We must quickly identify and eliminate these risks in order to protect patients. Here are examples of the good, the bad and the ugly from EHR.

152
The Good

153
Good Stuff: EHR helps to manage risk by: Virtually eliminating legibility problems and transcription errors Increasing the likelihood that information will get into the Medical Record, i.e. significant medical advice (JCAHO and AAAHC standards).
..")
154
Good, continued Allowing up to the minute information to be accessed from any computer in the clinic, and some computers outside the clinic by private network as well. Using templates to help decrease opportunity for omissions/errors And much, much more!

155
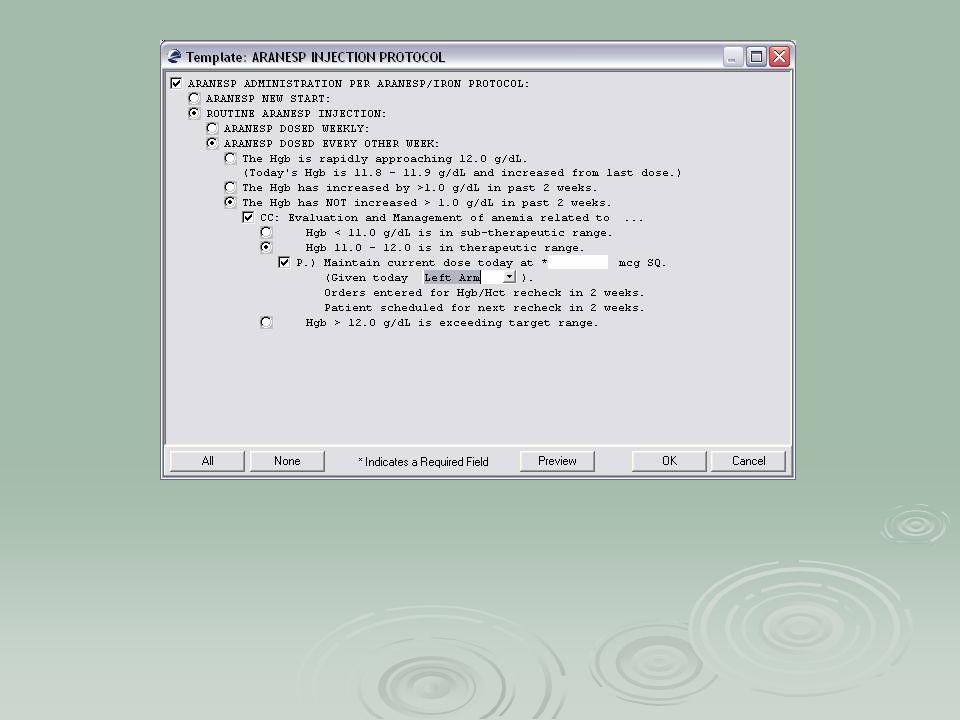
Example: Solution to RM Issue Using EHR Template Erythropoietin (formulary change to darbo) Complex protocol difficult to follow. Things needing to be addressed include: Adequacy of iron stores important to address.Adequacy of iron stores important to address. Safety issue of overshooting hematocrit targets, screening for symptoms of adverse events required.Safety issue of overshooting hematocrit targets, screening for symptoms of adverse events required. High cost if patient ends up on large doses or Medicare doesn’t cover because patient over targetHigh cost if patient ends up on large doses or Medicare doesn’t cover because patient over target

156
Solution Using EHR Template created to help decrease risk: used as decision-making tool charting template that ensures both quality of care and comprehensive documentation for meeting billing requirements.

158
Bad Dragging labs and vitals into the note and forgetting to address a wildly abnormal value Documenting your treatment in the note and prescribing something totally different w/o an addendum

159
Ugly Using EHR to document a QI finding Using EHR to indicate that you’ve asked a provider to do something a hundred thousand times Using EHR to identify which GPRA indicator we failed to address Using EHR to tell IT folks that there is a problem and, by golly they need to come fix it

160
RM issues During EHR Implementation Be aware that weirdness can happen in the beginning until you figure it out. Monitor ALL your processes and pay attention to ALL end users. This is how you discover problems and fix them!

161
Lessons Learned EHR implementation does NOT necessarily decrease overall waiting time—we’ll see in February! People document the darndest things in charts. EHR makes these things more apparent because you can more easily see everything at the click of the mouse. Every provider has a vastly different slope on their learning curve

162
Lessons Learned - continued Everyone wants to start the visit! This generates errors. Doctors, Nurses and Pharmacists are NOT coders We will always need Data Entry folks, but their roles are changing (more coding and sleuthing) Having a “table of contents” for notes makes reviewing records more efficient
 Having a table of contents for notes makes reviewing records more efficient.")
163
Lessons Learned, Cont’ Case Management and Chart Reviews Templates can be built with objects that pull in the needed data. Also the ability to document patient reminder letters at the same time they are created. Templates can be built with objects that pull in the needed data. Also the ability to document patient reminder letters at the same time they are created. Per Dr. Howard Hays: “Integrated Case Management is in the conceptual development phase at the present time. We hope to have it available for general use in about a year. It will be available either in the traditional RPMS format or as a component of the EHR.” (December, 2004) Per Dr. Howard Hays: “Integrated Case Management is in the conceptual development phase at the present time. We hope to have it available for general use in about a year. It will be available either in the traditional RPMS format or as a component of the EHR.” (December, 2004)
 Per Dr. Howard Hays: Integrated Case Management is in the conceptual development phase at the present time. We hope to have it available for general use in about a year. It will be available either in the traditional RPMS format or as a component of the EHR. (December, 2004).")
164
Lessons Learned, continued Flow Sheets –why is a flow sheet needed and is it still an issue with EHR? Ex: erythropoietin- same information entered on a flow sheet is available to view in EHR. Ex: erythropoietin- same information entered on a flow sheet is available to view in EHR. Notes with continuous addendums can sometimes take the place of a flow sheet. Notes with continuous addendums can sometimes take the place of a flow sheet. Use note titles to be able to retrieve related visits- may eliminate the need for a flow sheet. Use note titles to be able to retrieve related visits- may eliminate the need for a flow sheet. Protocols, Practice Guidelines, Standing Orders – can be addressed by using templates that contain decision trees as with darbopoeitin (Aranesp).
..")
165
Take home message EHR is no different than the paper record. It is the legal document that will go to court when things go wrong. It is important to monitor regularly what is going in the record. Charting mantras that have not changed: If it wasn’t documented, it wasn’t done If it wasn’t documented, it wasn’t done Just the (pertinent) facts, Jack Just the (pertinent) facts, Jack
 facts, Jack Just the (pertinent) facts, Jack.")
166
Quality Improvement, Risk Management and Lessons Learned from EHR Michele Gemelas, R.Ph. QI/RM/GPRA Coordinator Warm Springs Health and Wellness Center

Similar presentations




 Urban Health Programs August 2010.>")









 and Patient Care Component (PCC) configuration.>")
” versus “Vuecentric” Template Review keys required.>")






