Download presentation
Presentation is loading. Please wait.

1
2LT Larson 2LT Loomis 1LT Moravec
Compartment Syndrome 2LT Larson 2LT Loomis 1LT Moravec

2
AGENDA Introduction/Purpose Involved Anatomy Etiology
Clinical Presentation and Dx Treatment/Intervention Conclusion

3
INTRODUCTION Compartment Syndrome can be a life/limb threatening emergency Related to acute trauma or exertion Affects the muscle tissue, innervation, and vascularization within a MS compartment Has also been described in the foot, thigh, forearm and gluteal regions

4
Types of CS Acute Compartment Syndrome Exertional Compartment Syndrome
Acute-one time episode Chronic- with activity

5
Under Pressure? From Anatomy we all know the Crural Fascia is VERY tight and has a limited ability to expand Increased compartmental pressure can result in ischemia, neuropraxia and if sustained, tissue NECROSIS

6
Anterior Lateral COMPARTMENTS Deep Posterior Posterior

7
Etiology Acute CS: Direct trauma = Fx or soft-tissue injury
More common in men (McQueen et al) Initial injury leads to swelling within compartment Muscle damage theorized to increases osmotic pressure from release of protein-bound ions -During exercise, there can be a 20% increase in muscle volume as well as possible tissue edema. -As these fascial compartments have a limited ability to expand and accommodate the increased muscle volume, the pressure inside these compartments increases with strenuous exercise. CECS is most commonly linked to ischemia of the involved muscles resulting from the increase in intracompartmental pressure. Theories of Ischemia (bottom line: Decreased Blood Flow): -arterial spasm resulting in decrease of arterial inflow -arteriole or venous collapse due to pressure disturbances -When pressure in a compartment increases, the decreased vascular supply to the nerves can also be affected causing parethersias to occur
 Initial injury leads to swelling within compartment. Muscle damage theorized to increases osmotic pressure from release of protein-bound ions. -During exercise, there can be a 20% increase in muscle volume as well as possible tissue edema. -As these fascial compartments have a limited ability to expand and accommodate the increased muscle volume, the pressure inside these compartments increases with strenuous exercise. CECS is most commonly linked to ischemia of the involved muscles resulting from the increase in intracompartmental pressure. Theories of Ischemia (bottom line: Decreased Blood Flow): -arterial spasm resulting in decrease of arterial inflow. -arteriole or venous collapse due to pressure disturbances. -When pressure in a compartment increases, the decreased vascular supply to the nerves can also be affected causing parethersias to occur.")
8
Etiology Exertional CS:
Overexertion- Associated with repetitive axial loading (runners and competitive skaters) Muscle volume can increase up to 20% due to fiber swelling and blood filling from vigorous exercise
 Muscle volume can increase up to 20% due to fiber swelling and blood filling from vigorous exercise.")
9
Etiology Chronic ECS (most commonly in Deep Compartment): No anatomical predisposition has been proven Excessive compensatory pronation of the subtalor joint implicated During gait this would increase activity of deep posterior compartment muscles Usually bilateral involvement (50%-70%); one extremity usually more symptomatic
; one extremity usually more symptomatic.")
10
CLINICAL PRESENTATION
Pnt c/o severe pain out of proportion to injury Pain aggravated by passive muscle stretch Loss of sensation may be useful sign Dorsalis pedis pulse may or may not be affected

11
CLINICAL PRESENTATION
Leg pain described as a dull ache (localized or diffuse) that begins at a predictable time during exercise May also have: Footdrop Giving away of the ankle Paraesthesias in the foot Taut, shiny, warm skin that is TTP
 that begins at a predictable time during exercise. May also have: Footdrop. Giving away of the ankle. Paraesthesias in the foot. Taut, shiny, warm skin that is TTP.")
12
CLINICAL PRESENTATION
Post-exercise Involved compartments are swollen and tense Increased leg girth over involved muscles Passive stretching of involved muscles may increase pain Symptoms usually lessen within 30 min

13
Differential Diagnosis
Rule out stress fractures or periostitis Radiographs, bone-scan, bony tenderness Medial tibial stress syndrome pain and tenderness over soleus bridge pain with exercise which can progress to other activities pain increased by hyperpronation of the foot Compression neuropathies- electromyography

14
Clinical Diagnosis Intracompartmental pressure recordings (Taken pre/post exercise w/ slit catheter under local anesthesia) -Monitoring of pressures is usually done with wick catheter or slick catheter that allow pre and post exercise testing. Needle tip location and depth of penetration, as well as knee and ankle position are controlled to obtain valid and reliable measurements. (Both methods have proven equally reliable) -Normal intracompartmental pressure is between 0 and 8 mm Hg -An extended delay in normalization of pressures after exercise is also significant Pedowitz et al.
 -Normal intracompartmental pressure is between 0 and 8 mm Hg. -An extended delay in normalization of pressures after exercise is also significant. Pedowitz et al.")
15
Treating ECS Conservative at first
Cross training with low impact activities (swimming, bicycling) Rest, Ice, Elevation No Compression NSAIDS Stretching Address biomechanical problems Gradual return to activity
 Rest, Ice, Elevation No Compression. NSAIDS. Stretching. Address biomechanical problems. Gradual return to activity.")
16
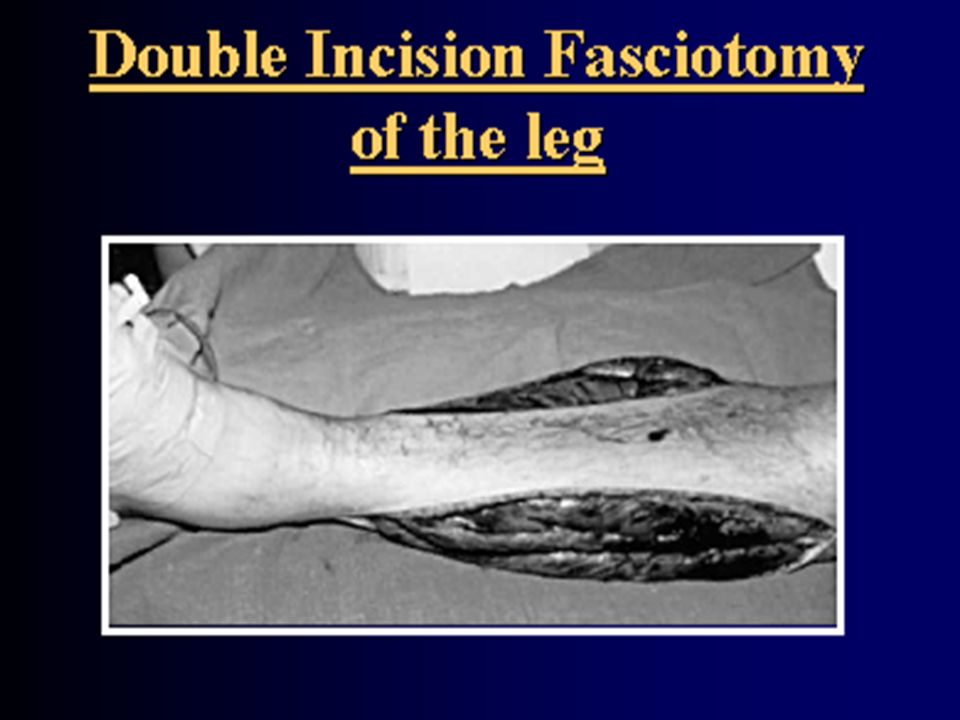
Treatment Options If symptoms persist with activity for > 3 to 6 months A: Stop prevocational activities B: Have Surgery: Fasciotomy of all involved compartments

18
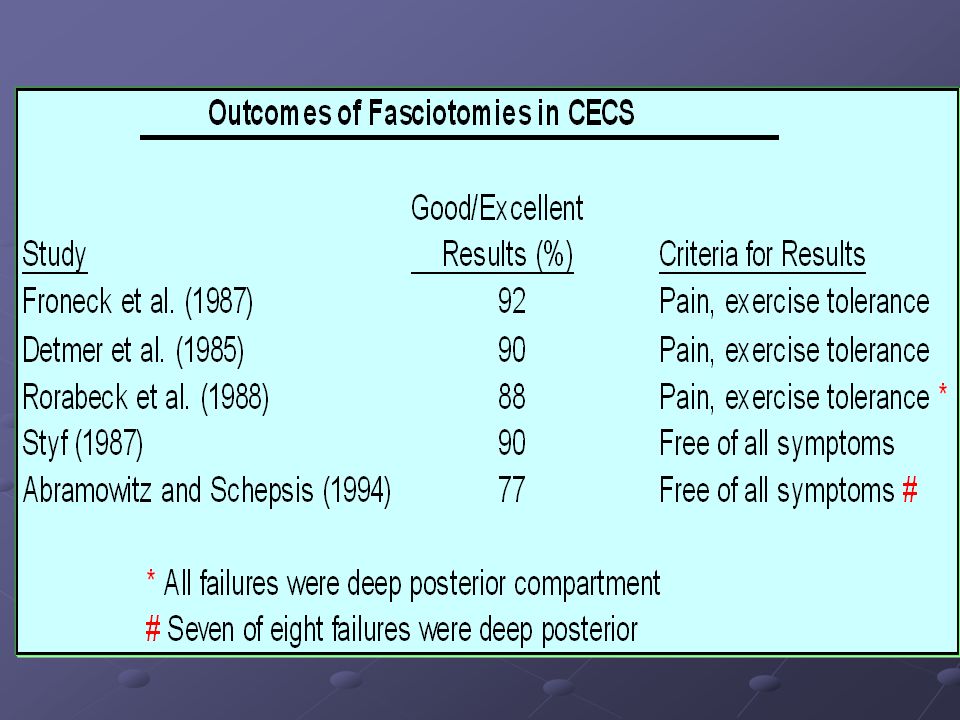
Surgical Outcome Dependent upon compartment involvement
Results of anterior and lateral releases are superior to posterior release Failure of Deep posterior compartment release largely due to insufficient release-as it is harder to get to Management of fasciotomy wounds is controversial

20
PT Intervention Post Surgery
Immediate Ice and Elevation Crutches (TTWB) with gradual progression to FWB (1 week) Gait training to prevent abnormal movement secondary to stiffness and guarding ROM exercises to increase circulation: ankle dorsiflexion, plantar flexion, inversion, eversion, alphabet exercise knee flexion/ extension
 with gradual progression to FWB (1 week) Gait training to prevent abnormal movement secondary to stiffness and guarding. ROM exercises to increase circulation: ankle dorsiflexion, plantar flexion, inversion, eversion, alphabet exercise. knee flexion/ extension.")
21
Rehab Progression Gentle isokinetics Stretching, of involved muscles
Aerobic training: Limited WB (swimming/cycling) 4 weeks: progression to running and resistive weight training as tolerated 2-3 months full return to training
 4 weeks: progression to running and resistive weight training as tolerated. 2-3 months full return to training.")
22
Conclusion Exercise induced ECS is often miss-diagnosed.
Awareness is key due to the dangers of untreated acute ECS. Non-surgical interventions not shown to help long term. Surgery is intervention for reliably high prognosis. PT plays important role in Dx and post surgical Tx.

23
QUESTIONS?

24
REFERENCES 1. Tiwari A, Haq AI, Myint F, Hamilton G. Acute compartment syndromes. British Journal of Surgery. 2002; 89(4): 2. McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk?[comment]. Journal of Bone & Joint Surgery - British Volume. 2000;82(2): 3. Pearse MF, Harry L, Nanchahal J. Acute compartment syndrome of the leg: fasciotomies must be performed early, but good surgical technique is important. British Medical Journal. 14 September ;Volume 325(7364): 4. Garcia-Mata S, Hidalgo-Ovejero A, Martinez-Grande M. Chronic exertional compartment syndrome of the legs in adolescents. Journal of Pediatric Orthopedics. 2001;21(3): 5. Prentice WE, Voight MI. Techniques in musculoskeletal rehabilitation. New York: McGraw-Hill; 2001. 6. Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder? Journal of Orthopaedic Trauma. 2002;16(8): 7. Finkelstein JA, Hunter GA, Hu RW. Lower limb compartment syndrome: course after delayed fasciotomy. Journal of Trauma-Injury Infection & Critical Care. 1996;40(3):
: Pearse MF, Harry L, Nanchahal J. Acute compartment syndrome of the leg: fasciotomies must be performed early, but good surgical technique is important. British Medical Journal. 14 September ;Volume 325(7364): Garcia-Mata S, Hidalgo-Ovejero A, Martinez-Grande M. Chronic exertional compartment syndrome of the legs in adolescents. Journal of Pediatric Orthopedics. 2001;21(3): Prentice WE, Voight MI. Techniques in musculoskeletal rehabilitation. New York: McGraw-Hill; Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder Journal of Orthopaedic Trauma. 2002;16(8): Finkelstein JA, Hunter GA, Hu RW. Lower limb compartment syndrome: course after delayed fasciotomy. Journal of Trauma-Injury Infection & Critical Care. 1996;40(3):")
Similar presentations



>")







>")







