Download presentation
Presentation is loading. Please wait.

1
What’s Trauma Got To Do With It ?
Dr. Allison Sampson Jackson Family Preservation Services Of North Carolina

4
ACE SCREEN

5
223,400,000 223,400,000 317,572,282 Information and slide part of Dr. Allison Sampson's Trauma Presentation

6
Exposure to Violence in Childhood
46 million of 76 million children are exposed to violence, crime and abuse each year Finkelhor, D., et al. (2010). Trends in childhood violence and abuse exposure: evidence from 2 national surveys. Archives of Pediatric and Adolescent Medicine, 164(3), 238–42. Information and slide part of Dr. Allison Sampson's Trauma Presentation
. Trends in childhood violence and abuse exposure: evidence from 2 national surveys. Archives of Pediatric and Adolescent Medicine, 164(3), 238–42. Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
7
Relevance of Trauma to Child Welfare
“Henry” and Some Data

8
Prevalence of Trauma—United States
Each year in the United States, more than 1,400 children—nearly 2 children per 100,000—die of abuse or neglect. In 2005, 899,000 children were victims of child maltreatment. Of these: 62.8% experienced neglect 16.6% were physically abused 9.3% were sexually abused 7.1% endured emotional or psychological abuse 14.3% experienced other forms of maltreatment (e.g., abandonment, threats of harm, congenital drug addiction) Source: USDHHS. (2007) Child Maltreatment 2005; Washington, DC: US Gov’t Printing Office. 26 26
 Source: USDHHS. (2007) Child Maltreatment 2005; Washington, DC: US Gov’t Printing Office")
9
Prevalence of Trauma—United States
Each year in the United States, more than 1,400 children—nearly 2 children per 100,000—die of abuse or neglect. In 2005, 899,000 children were victims of child maltreatment. Of these: 62.8% experienced neglect 16.6% were physically abused 9.3% were sexually abused 7.1% endured emotional or psychological abuse 14.3% experienced other forms of maltreatment (e.g., abandonment, threats of harm, congenital drug addiction) Source: USDHHS. (2007) Child Maltreatment 2005; Washington, DC: US Gov’t Printing Office. 26 26
 Source: USDHHS. (2007) Child Maltreatment 2005; Washington, DC: US Gov’t Printing Office")
10
U.S. Prevalence, cont'd One in four children/adolescents experience at least one potentially traumatic event before the age of 16.1 In a 1995 study, 41% of middle school students in urban school systems reported witnessing a stabbing or shooting in the previous year.2 Four out of 10 U.S. children report witnessing violence; 8% report a lifetime prevalence of sexual assault, and 17% report having been physically assaulted.3 1. Costello et al. (2002). J Traum Stress;5(2): 2. Schwab-Stone et al. (1995). J Am Acad Child Adolesc Psychiatry;34(10): 3. Kilpatrick et al. (2003). US Dept. Of Justice. 27 27
. J Traum Stress;5(2): Schwab-Stone et al. (1995). J Am Acad Child Adolesc Psychiatry;34(10): Kilpatrick et al. (2003). US Dept. Of Justice")
11
Prevalence of Trauma in the Child Welfare Population
A national study of adult “foster care alumni” found higher rates of PTSD (21%) compared with the general population (4.5%). This was higher than rates of PTSD in American war veterans.1 Nearly 80% of abused children face at least one mental health challenge by age 21.2 1. Pecora, et al. (December 10, 2003). Early Results from the Casey National Alumni Study. Available at: E5BAF602294D/302/casey_alumni_studies_report.pdf. 2. ASTHO. (April 2005). Child Maltreatment, Abuse, and Neglect. Available at: 28 28
 compared with the general population (4.5%). This was higher than rates of PTSD in American war veterans.1. Nearly 80% of abused children face at least one mental health challenge by age Pecora, et al. (December 10, 2003). Early Results from the Casey National Alumni Study. Available at: E5BAF602294D/302/casey_alumni_studies_report.pdf. 2. ASTHO. (April 2005). Child Maltreatment, Abuse, and Neglect. Available at:")
12
Prevalence in Child Welfare Population, cont'd
A study of children in foster care revealed that PTSD was diagnosed in 60% of sexually abused children and in 42% of the physically abused children.1 The study also found that 18% of foster children who had not experienced either type of abuse had PTSD,1 possibly as a result of exposure to domestic or community violence.2 1. Dubner et al. (1999). JCCPsych;67(3): 2. Marsenich (March 2002). Evidence-Based Practices in Mental Health Services for Foster Youth. Available at: 29
. JCCPsych;67(3): Marsenich (March 2002). Evidence-Based Practices in Mental Health Services for Foster Youth. Available at:")
13
Mismanagement of Trauma Hendrick, H
Mismanagement of Trauma Hendrick, H. (2012) Creating Trauma-Informed Child Welfare Systems, p. 6 - Reduces likelihood of reunification (1) - Increases placement instability (2) - Increase in restrictive placements (3) - Increases likelihood of using stronger psychotropic medications (4) - Increases child perpetuating intergenerational cycle of abuse and neglect when they become a parent (5) Rubin, O’Reilly, Luan, & Localio (2007) Pediatrics, 119 (2) Hartnett, Leathers, Falconnier & Testa (1999) Placement Stability Study. Pecora et al. (2005) Raghavan et al. (2005) Journal of Child and Adolescent Psychopathology, 15(1), Fang & Corso (2007) American Journal of Preventative Medicine, 33(4),
 Creating Trauma-Informed Child Welfare Systems, p Reduces likelihood of reunification (1) - Increases placement instability (2) - Increase in restrictive placements (3) - Increases likelihood of using stronger psychotropic medications (4) - Increases child perpetuating intergenerational cycle of abuse and neglect when they become a parent (5) Rubin, O’Reilly, Luan, & Localio (2007) Pediatrics, 119 (2) Hartnett, Leathers, Falconnier & Testa (1999) Placement Stability Study. Pecora et al. (2005) Raghavan et al. (2005) Journal of Child and Adolescent Psychopathology, 15(1), Fang & Corso (2007) American Journal of Preventative Medicine, 33(4),")
14
“Our Kids” in Juvenile Justice
“ I am a child” Poem

15
Trauma and Juvenile Justice
A growing body of research indicates that victims of violence are more likely than their peers to also be perpetrators of violence, and that individuals most likely to be victims of personal crime are those who report the greatest involvement in delinquent activities (ABA, 2000; Shaffer and Ruback, 2002; Wiebush et al., 2001).
.")
16
“Our Kids” in Juvenile Justice
Studies with antisocial youth have found self reported trauma exposure ranging from 70% to 92% (Greenwald, 2002) Antisocial youth have high rates of Post Traumatic Stress Disorder (PTSD) ranging from 24% to 65% (Greenwald, 2002) Research has indicated high levels of trauma in the experiences of conduct-disorder youth (Bowers, 1990; McMackin, Morissey, Newman, Erwin, & Daley, 1998; Rivera & Widom, 1990; and Steiner, Garcia, & Matthews, 1997) Research suggests that anger and violent acting out often are symptoms of PTSD (Chemtob, Novaco, Hamada, Gross, & Smith, 1997) Information and slide part of Dr. Allison Sampson's Trauma Presentation
 Antisocial youth have high rates of Post Traumatic Stress Disorder (PTSD) ranging from 24% to 65% (Greenwald, 2002) Research has indicated high levels of trauma in the experiences of conduct-disorder youth (Bowers, 1990; McMackin, Morissey, Newman, Erwin, & Daley, 1998; Rivera & Widom, 1990; and Steiner, Garcia, & Matthews, 1997) Research suggests that anger and violent acting out often are symptoms of PTSD (Chemtob, Novaco, Hamada, Gross, & Smith, 1997) Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
17
Trauma and Juvenile Delinquency
Research shows that childhood exposure to domestic and community violence, for example, can cause children to engage in aggressive behavior, suffer from problems such as depression and anxiety, have lower levels of social competence and self-esteem, experience poor academic performance, and exhibit posttraumatic stress symptoms such as emotional numbing and increased arousal (Colley-Quille et al., 1995; ABA, 2000; Osofsky, 1999).
.")
18
The future for “our kids” ….
Being abused or neglected as a child increased the likelihood of arrest as a juvenile by 59 percent and as an adult by 28 percent, and for a violent crime by 30 percent. The abused and neglected cases were younger at first arrest, committed nearly twice as many offenses, and were arrested more frequently (Widom, 1995; Widom and Maxfield, 2001).
.")
19
Data from the National Survey of Adolescents (Kilpatrick et al
Data from the National Survey of Adolescents (Kilpatrick et al., 2003b) 47.2 percent of the sexually assaulted boys reported engaging in delinquent acts, compared with only 16.6 percent of those not sexually assaulted The rate of girls who had been sexually assaulted and then committed delinquent acts was 19.7 percent, five times higher than the rate of girls who had not been sexually assaulted (4.8 percent). The percentage of boys who were physically assaulted and had ever committed an Index offense was 46.7 percent, compared to 9.8 percent of boys who were not assaulted. 29.4 percent of physically assaulted girls reported having engaged in serious delinquent acts at some point in their lives, compared with 3.2 percent of nonassaulted girls. About one third (32 percent) of boys who witnessed violence reported ever engaging in delinquent acts, compared with only 6.5 percent of boys who did not witness violence. About 17 percent of girls who witnessed violence reported lifetime delinquent behavior, compared with 1.4 percent of girls who did not witness violence.
 47.2 percent of the sexually assaulted boys reported engaging in delinquent acts, compared with only 16.6 percent of those not sexually assaulted. The rate of girls who had been sexually assaulted and then committed delinquent acts was 19.7 percent, five times higher than the rate of girls who had not been sexually assaulted (4.8 percent). The percentage of boys who were physically assaulted and had ever committed an Index offense was 46.7 percent, compared to 9.8 percent of boys who were not assaulted percent of physically assaulted girls reported having engaged in serious delinquent acts at some point in their lives, compared with 3.2 percent of nonassaulted girls. About one third (32 percent) of boys who witnessed violence reported ever engaging in delinquent acts, compared with only 6.5 percent of boys who did not witness violence. About 17 percent of girls who witnessed violence reported lifetime delinquent behavior, compared with 1.4 percent of girls who did not witness violence.")
20
Relevance to Education Systems

21
Trauma impacts learning and academic outcomes
Decreased IQ and reading ability (Delaney-Black et al., 2003) Lower grade-point average (Hurt et al., 2001) More days of school absence (Hurt et al., 2001) Decreased rates of high school graduation (Grogger, 1997) Increased expulsions and suspensions (LAUSD Survey)
 Lower grade-point average (Hurt et al., 2001) More days of school absence (Hurt et al., 2001) Decreased rates of high school graduation (Grogger, 1997) Increased expulsions and suspensions (LAUSD Survey)")
22
Impact of being in Child Welfare System for Foster Care Children
25% will be incarcerated within first 2 years of aging out of the system More than 20% will become homeless Only 58% will have a High School Diploma Less than 3% will have a college education by age of 25 Many will re-enter the system as parents For children under age of 5, increase likelihood of developmental delays 13-62% compared to 4-10% Conradi, L. (2012) Chadwick Trauma Informed System Project p. 54 Leslie et. al. (2005). Developmental and Behavioral Pediatrics 26(3),
 Chadwick Trauma Informed System Project p. 54. Leslie et. al. (2005). Developmental and Behavioral Pediatrics 26(3),")
23
1 year of violence= 124 billion dollars in recovery costs
The breakdown per child is: • $32,648 in childhood health care costs • $10,530 in adult medical costs • $144,360 in productivity losses • $7,728 in child welfare costs • $6,747 in criminal justice costs • $7,999 in special education costs

24
Emotional Chain of Custody
System Issue

25
Alcoholism and alcohol abuse
Chronic obstructive pulmonary disease (COPD) Depression Fetal death Health-related quality of life Illicit drug use Ischemic heart disease (IHD) Liver disease Risk for intimate partner violence Multiple sexual partners Sexually transmitted diseases (STDs) Smoking Suicide attempts Unintended pregnancies Early initiation of smoking Early initiation of sexual activity Adolescent pregnancy
 Depression. Fetal death. Health-related quality of life. Illicit drug use. Ischemic heart disease (IHD) Liver disease. Risk for intimate partner violence. Multiple sexual partners. Sexually transmitted diseases (STDs) Smoking. Suicide attempts. Unintended pregnancies. Early initiation of smoking. Early initiation of sexual activity. Adolescent pregnancy.")
26
My story ….

28
Unlocking the Brain At least for today…3 brain levels-they each speak a different language Brainstem-housekeeping of the Body, sleeping, eating, breathing Limbic-smoke alarm, implicit memories Cortex-planning, logic, reason, judgment Brainstem and Limbic-what fires together wires together

29
A Person’s Response to Perceived Danger
Trauma Event Danger Response Fight Flight Freeze Aggression Run Away Dissociate Verbal attack Substance Abuse Non-emotionality Slide from Ellen Williams, LCSW Center for Child & Family Services

30
Looking Through The Eyes of a Traumatized Child- How it looks to Us….
Slide from Ellen Williams, LCSW Center for Child & Family ServicesServices

31
How it looks to The Traumatized Child
Slide from Ellen Williams, LCSW Center for Child & Family ServicesServices

32
Fight Response Fight-discharge energy

33
Fight, Flight, Freeze Flight Response: Movement
PTSD rates New York 6%, Katrina 34%

34
Images of Freeze

35
“Thousands wait” A Forced Freeze
6% of NYC had PTSD 33% had PTSD in New Orleans

36
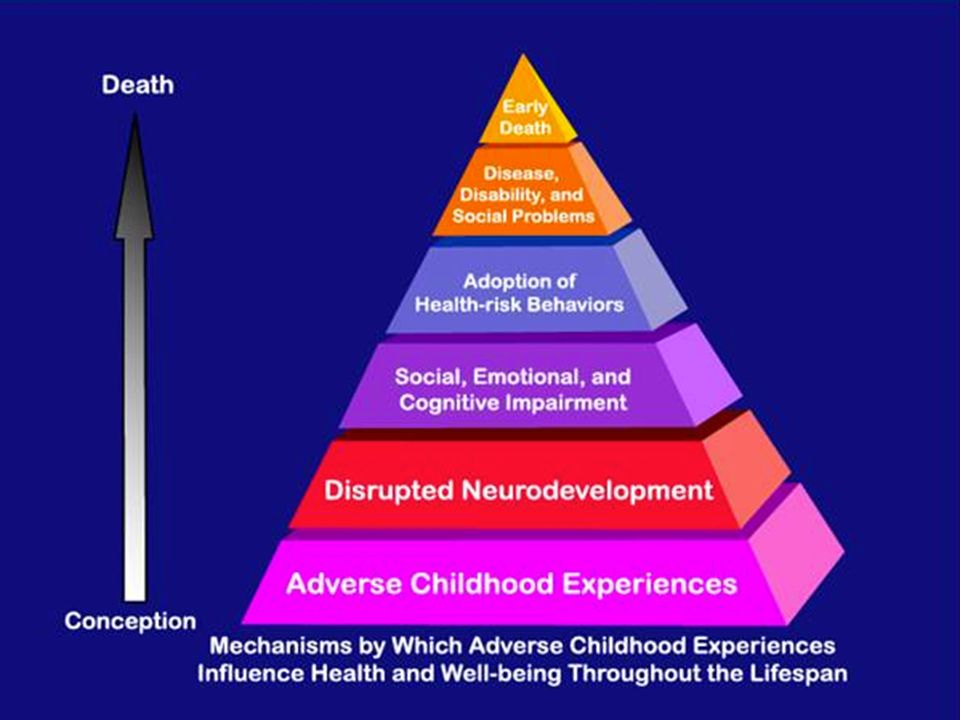
Types of Stress Positive Stress Tolerable Stress Toxic Stress Normal and essential part of healthy development Body’s alert systems activated to a greater degree Occurs with strong, frequent or prolonged adversity Brief increases in heart rate and blood pressure Activation is time limited and buffered by caring adult Disrupts brain architecture and other organ systems Mild elevations in hormonal levels Brain and organs recover Increased risk of stress-related disease and cognitive impairment Example: Tough test at school or a playoff game Example: Death of a loved one, divorce, natural disaster Example: abuse, neglect, caregiver substance dependence or mental illness Social –emotional buffering Parental Resilience Early Detection Effective Intervention Intense Prolonged Repeated Unaddressed Information and slide part of Harris (2013) Buzz on Brain and Babies Presentation
 Buzz on Brain and Babies Presentation.")
37
The Hand Model of the Brain

38
The Handy Model

40
Self-Destructive Behavior
Chasing Behaviors Agitation Hopelessness Intrusive Memories Nightmares Insomnia Defiance Poor Impulse Control Numbing Traumatic Event Shame & Self-Hatred Depression Panic Attacks Dissociation Somatic Symptoms Withdrawal Self-Destructive Behavior Eating Disorders Substance Abuse T Slide by Trish Mullens, Chesterfield CSB

41
We must …… Respond to the need …. Not react to the behavior

42
Resilience Trumps Aces
From Trish Mullen, Chesterfield Community services Board

43
Trauma and the Brain

44
The Influence of Developmental Stage
Child traumatic stress reactions vary by developmental stage. Children who have been exposed to trauma expend a great deal of energy responding to, coping with, and coming to terms with the event. This may reduce children’s capacity to explore the environment and to master age-appropriate developmental tasks. The longer traumatic stress goes untreated, the farther children tend to stray from appropriate developmental pathways. 52 52

45
Young children who have experienced trauma may:
The Influence of Developmental Stage: Young Children Young children who have experienced trauma may: Become passive, quiet, and easily alarmed Become fearful, especially regarding separations and new situations Experience confusion about assessing threat and finding protection, especially in cases where a parent or caretaker is the aggressor Regress to recent behaviors (e.g., baby talk, bed-wetting, crying) Experience strong startle reactions, night terrors, or aggressive outbursts 53 53
 Experience strong startle reactions, night terrors, or aggressive outbursts")
46
The Influence of Developmental Stage: School-Age Children
School-age children with a history of trauma may: Experience unwanted and intrusive thoughts and images Become preoccupied with frightening moments from the traumatic experience Replay the traumatic event in their minds in order to figure out what could have been prevented or how it could have been different Develop intense, specific new fears linking back to the original danger 54 54

47
The Influence of Developmental Stage: School-Age Children, cont’d
School-age children may also: Alternate between shy/withdrawn behavior and unusually aggressive behavior Become so fearful of recurrence that they avoid previously enjoyable activities Have thoughts of revenge Experience sleep disturbances that may interfere with daytime concentration and attention 55

48
The Influence of Developmental Stage: Adolescents
In response to trauma, adolescents may feel: That they are weak, strange, childish, or “going crazy” Embarrassed by their bouts of fear or exaggerated physical responses That they are unique and alone in their pain and suffering Anxiety and depression Intense anger Low self-esteem and helplessness 56 56

49
The Influence of Developmental Stage: Adolescents, cont’d
These trauma reactions may in turn lead to: Aggressive or disruptive behavior Sleep disturbances masked by late-night studying, television watching, or partying Drug and alcohol use as a coping mechanism to deal with stress Over- or under-estimation of danger Expectations of maltreatment or abandonment Difficulties with trust Increased risk of revictimization, especially if the adolescent has lived with chronic or complex trauma 57 57

50
Adolescents who have experienced trauma may use alcohol or drugs in an attempt to avoid overwhelming emotional and physical responses. In these teens: Reminders of past trauma may elicit cravings for drugs or alcohol. Substance abuse further impairs their ability to cope with distressing and traumatic events. Substance abuse increases the risk of engaging in risky activities that could lead to additional trauma. Child welfare stakeholders must address the links between trauma and substance abuse and consider referrals for relevant treatment(s). 58 58
")
51
The Influence of Developmental Stage: Specific Adolescent Groups
Homeless youth are at greater risk for experiencing trauma than other adolescents. Many have run away to escape recurrent physical, sexual, and/or emotional abuse Female homeless teens are particularly at risk for sexual trauma Special needs adolescents are 2 to 10 times more likely to be abused than their typically developing counterparts. Lesbian, gay, bisexual, transgender or questioning (LGBTQ) adolescents contend with violence directed at them in response to suspicion about or declaration of their sexual orientation and gender identity 59 59
 adolescents contend with violence directed at them in response to suspicion about or declaration of their sexual orientation and gender identity")
52
BIG PICTURE … Many of the symptoms we are seeing in the children we work with are direct results of coping with trauma … When we try to take away their coping, families and children often withdraw and protect themselves from us … Be aware of the “invisible suitcase” that our children and parents bring with them as they move into the system and often away from everything they know …

53
Cross Generational Trauma ...
What about the caregivers ….

54
Perspective of a parent …
Poem … perspective on children of trauma who have now grown up to be parents … Understanding how trauma may be impacting a birth parent Impact of trauma on communication and decision making of adult caregivers Data on caregivers needs

55
Cross- Generational Trauma Histories Hendricks (2012) Chapter 12 of Creating Trauma Informed Child Welfare Systems Using Trauma Informed Services to Increase Parental Protective Factors Why does it matter to us ? -Affects the emotions and behaviors of the parents and thus their communication and decision-making - All that we have learned about trauma, attachment, and the brain now applies to the parents - Is an important consideration in kinship care and relative placements Not addressing parental trauma history decreases the parenting abilities of all caregivers in the child’s life … results in disrupted placements and client recidivism

56
If a parents has had chronic trauma in their own childhoods it impacts
Cross-Generational Trauma Hendricks (2012) Chapter 12 of Creating Trauma Informed Child Welfare Systems Using Trauma Informed Services to Increase Parental Protective Factors If a parents has had chronic trauma in their own childhoods it impacts Ability to engage in positive parent child interactions Ability to protect their own children Ability to help their children recover from trauma Ability to cope and function with Child Welfare interventions (including removal) with their children
 Chapter 12 of Creating Trauma Informed Child Welfare Systems Using Trauma Informed Services to Increase Parental Protective Factors. If a parents has had chronic trauma in their own childhoods it impacts. Ability to engage in positive parent child interactions. Ability to protect their own children. Ability to help their children recover from trauma. Ability to cope and function with Child Welfare interventions (including removal) with their children.")
57
Cross-Generational Trauma Hendricks (2012) Chapter 12 of Creating Trauma Informed Child Welfare Systems Using Trauma Informed Services to Increase Parental Protective Factors Women who have experienced trauma are more likely to self- medicate with a substance (55-99%) (1) Intergenerational transmission of trauma (Depression, PTSD) (2) Unresolved childhood trauma can lead to reenactments with partners in adult relationships and/or with their children (3) Unresolved childhood trauma can lead to difficulty forming secure attachments with their children (4) Childhood trauma can result in parenting styles that include threats & violence (2) Childhood sexual abuse survivors can miss “red flags” of sexual abuse with their own children due to avoidance of trauma memories themselves (2) Najavits, Weiss, & Shaw (1997) The American Journal on Addiction, 6 (4), Hendricks, A. (2012). Using Trauma-Informed Services to Increase Parental Factors (pp ) Walker (2007) Journal of Social Work Practice, 21 (1), Main & Hess (1990) In M. Greenberg, D. Cicchetti, & E. Cummings (Eds.), Attachment in the preschool years: Theory, research, and intervention (pp )
 (1) Intergenerational transmission of trauma (Depression, PTSD) (2) Unresolved childhood trauma can lead to reenactments with partners in adult relationships and/or with their children (3) Unresolved childhood trauma can lead to difficulty forming secure attachments with their children (4) Childhood trauma can result in parenting styles that include threats & violence (2) Childhood sexual abuse survivors can miss red flags of sexual abuse with their own children due to avoidance of trauma memories themselves (2) Najavits, Weiss, & Shaw (1997) The American Journal on Addiction, 6 (4), Hendricks, A. (2012). Using Trauma-Informed Services to Increase Parental Factors (pp ) Walker (2007) Journal of Social Work Practice, 21 (1), Main & Hess (1990) In M. Greenberg, D. Cicchetti, & E. Cummings (Eds.), Attachment in the preschool years: Theory, research, and intervention (pp )")
58
- Failure to engage in treatment services - An increase in symptoms
Cross-Generational Trauma Hendricks (2012) Chapter 12 of Creating Trauma Informed Child Welfare Systems Using Trauma Informed Services to Increase Parental Protective Factors Caregiver functioning following a child’s exposure to trauma is a major predictor of (1 & 2) If we want to improve a child’s outcome, we must address parent’s trauma history … failure to do so can result in (2) … - Failure to engage in treatment services - An increase in symptoms - An increase in management problems - Retraumatization - An increase in relapse - Withdrawal from service relationship - Poor treatment outcomes Linares et al (2001) Child Development, 72, Liberman, Van Horn, & Ozer (2005) Development and Psychopathology, 17, Hendricks, A. (2012) pp. 91
 Chapter 12 of Creating Trauma Informed Child Welfare Systems Using Trauma Informed Services to Increase Parental Protective Factors. Caregiver functioning following a child’s exposure to trauma is a major predictor of (1 & 2) If we want to improve a child’s outcome, we must address parent’s trauma history … failure to do so can result in (2) … - Failure to engage in treatment services. - An increase in symptoms. - An increase in management problems. - Retraumatization. - An increase in relapse. - Withdrawal from service relationship. - Poor treatment outcomes. Linares et al (2001) Child Development, 72, Liberman, Van Horn, & Ozer (2005) Development and Psychopathology, 17, Hendricks, A. (2012) pp. 91.")
59
Pro-Active Approaches with Parents
Utilize trauma focused screening and assessment and treatment services with all family members including the birth family Don’t just make a referral to general mental health services, substance abuse services, or domestic violence services Advocate for better trained service providers Promote awareness of parent trauma across Child Welfare System Hendricks, A. (2012) Using Trauma Informed Services to Increase Parental Protective Factors from Chapter 12 of Creating Trauma Informed Child Welfare Systems. (p. 91)
 Using Trauma Informed Services to Increase Parental Protective Factors from Chapter 12 of Creating Trauma Informed Child Welfare Systems. (p. 91)")
60
Perspective on Entering into Child Welfare System
Impact of foster care and connection to biological parent

61
Foster Care Outcomes and Data
Based on Health and Human Services data (2005), children entering foster care …. 60% will return home 15% will be adopted Remaining children “age out” of foster care (19,000 per year)
, children entering foster care …. 60% will return home 15% will be adopted Remaining children age out of foster care (19,000 per year)")
62
Impact of being in Child Welfare System
25% will be incarcerated within first 2 years of aging out of the system More than 20% will become homeless Only 58% will have a High School Diploma Less than 3% will have a college education by age of 25 Many will re-enter the system as parents For children under age of 5, increase likelihood of developmental delays 13-62% compared to 4-10% Conradi, L. (2012) Chadwick Trauma Informed System Project p. 54 Leslie et. al. (2005). Developmental and Behavioral Pediatrics 26(3),
 Chadwick Trauma Informed System Project p. 54. Leslie et. al. (2005). Developmental and Behavioral Pediatrics 26(3),")
63
Foster Care and Family Preservation
Area of great focus is on balance between family preservation and child removal Increased knowledge of parental protective factors and trauma informed practice are being encouraged utilized with the birth parents given positive parental involvement increases positive outcomes for children Entering into the Child Welfare System and Foster Care are traumas, often including multiple placements that lead to problems for child development on top of the trauma child experienced in their home Some studies in Illinois looked at “close margin” cases where investigator may view removal of a child differently. Children remaining in the home demonstrated increased well-being, especially older children (lower risk of delinquency and adult criminal involvement, higher earnings and employment as an adult, possible relationship to lower rate of teen pregnancy) Doyle, J. (2007, 2008)
 Doyle, J. (2007, 2008)")
64
Birth Parent Involvement
Many studies indicate that caregiver functioning is a major predictor of child functioning after child experiences a trauma (Linares et al. 2001, Lieberman, Van Horn, & Ozer 2005) Birth parent involvement can improve children's depression and lower their externalizing behavior problems (McWey, Acock, & Porter 2010) See NCTSN Guide for Attorneys and Judges on Birth Parents and “What Children in Foster Care Want You to Know”
 Birth parent involvement can improve children s depression and lower their externalizing behavior problems (McWey, Acock, & Porter 2010) See NCTSN Guide for Attorneys and Judges on Birth Parents and What Children in Foster Care Want You to Know")
65
Outcomes Depend on Healing Injury From the Brain

66
Trauma and the Brain 3 structures we will pay attention to today
Amygdala-Limbic Prefrontal Cortex Brainstem

67
Trauma and the Brain 2 key structures
Amygdala- Fight, Flight, Freeze Hippocampus-Facts and Time, “PACMAN” for Stress/Cortisol

68
Trauma Trauma is a psychological and emotional injury.
It’s a natural reaction to an unnatural situation! Becoming trauma-informed does not mean we are excusing behavior..its an explanation!

69
Broca’s Area Notice Amygdala in neutral vs. trauma image. Visual and visceral. Broca’s Area comparision

70
Putting It Into Practice-Recognizing Traumatic Stress Symptoms

71
Whole Brain Learning In order to use both sides of the brain, neurons on the left side have to be connected to neurons on the right side. In other words, the electrical charge between brain cells has to pass across the “Bridge” corpus callosum. How do you get this neuronal pattern? How do you get these synapses across the corpus callosum?

72
Infinity 8 Mindfulness Training
Brain Gym Practice Infinity 8 Mindfulness Training

73
Vulnerability Mountain
Information and slide part of Dr. Allison Sampson's Trauma Presentation

74
Invisible Wounds: Realizing the Impact

75
Understanding “why” … Perry PetScan Information and slide part of Dr. Allison Sampson's Trauma Presentation

76
Trauma and Attachment

77
Attachment Many argue that these early relationships (experiences) shape neuronal circuits which regulate emotional and social functioning Information and slide part of Dr. Allison Sampson's Trauma Presentation

78
Attachment’s Purpose Siegel, 1999
Evolutionary Level – biological Infant Survival (Bowlby) Mind Level – biological and social Caregiver’s brain helps child’s brain to organize regulation Caregiver’s brain teaches child self-soothing Child experience of safety allows for exploration Information and slide part of Dr. Allison Sampson's Trauma Presentation
 Mind Level – biological and social. Caregiver’s brain helps child’s brain to organize regulation. Caregiver’s brain teaches child self-soothing. Child experience of safety allows for exploration. Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
79
Attachment’s Purpose Experience of safety is encoded in child’s implicit memory and provides secure base from which to grow and access higher levels of information processing Information and slide part of Dr. Allison Sampson's Trauma Presentation

80
What does this mean for children and adults who have experienced trauma? EXPERIENTIAL EXERCISE

81
Now let’s Practice

82
Teaching About the Brain
Upstairs/downstairs brain teaching practice Using of multiplying connection tools (amazing brain pamphlets) CAPPD Cards Partnering with Parents YOU MUST PRACTICE TEACHING ABOUT THE BRAIN
 CAPPD Cards. Partnering with Parents. YOU MUST PRACTICE TEACHING ABOUT THE BRAIN.")
83
What works in Behavioral Health? Phase Oriented Care
Information and slide part of Dr. Allison Sampson's Trauma Presentation

84
Core areas of focus in Complex Trauma Courtois, C. & Ford, J
Core areas of focus in Complex Trauma Courtois, C. & Ford, J. (2009), Introduction (p.2) Self-Regulation Affect Regulation Disassociation (difficulty in being “present”) Somatic Dysregulation Self-Identity Impaired Self-Concept Impaired Self-Development Co-regulation Secure working model of caring relationship Disorganized Attachment Patterns Information and slide part of Dr. Allison Sampson's Trauma Presentation
, Introduction (p.2) Self-Regulation. Affect Regulation. Disassociation (difficulty in being present ) Somatic Dysregulation. Self-Identity. Impaired Self-Concept. Impaired Self-Development. Co-regulation. Secure working model of caring relationship. Disorganized Attachment Patterns. Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
85
NCTSN Guidance on Components of Trauma Informed Treatment
Building a strong therapeutic relationship Affect expression and regulation skills Anxiety management Relaxation skills Cognitive processing/reframing Construction of a coherent trauma narrative Strategies that allow exposure to traumatic memories and feelings in tolerable doses so that they can be mastered and integrated into the child’s experience Personal safety/empowerment activities Resiliency and closure

86
Understand what good trauma treatment looks like …
Phase Oriented Treatment “ Gold Standard” Phase I: Safety and Stabilization Phase 2: Trauma Reprocessing Phase 3: Reintegration Handout on questions to ask Mental Health Providers Resource Information and slide part of Dr. Allison Sampson's Trauma Presentation

87
Trauma Informed Organization
Domain 1. Early Screening and Comprehensive Assessment of Trauma Domain 2. Consumer Driven Care and Services Domain 3. Trauma-Informed, Educated and Responsive Workforce Domain 4. Provision of Trauma-Informed, Evidence Based and Emerging Best Practices Domain 5. Create a Safe and Secure Environment Domain 6. Engage in Community Outreach and Partnership Building Domain 7. Ongoing Performance Improvement and Evaluation Information and slide part of Dr. Allison Sampson's Trauma Presentation

88
AIM Forward Model One Example of Trauma Informed Phase Oriented Care

89
Concept of AIM Forward Reviewing the ACE studies and realizing the broad stretch of trauma Dissertation interest in transfer of learning and models that improve assessment and intervention co-development Focus on well-being not just reduction of mental health symptoms Frustration with EBP only offerings and wanting to expand current research knowledge on working with trauma in a real time way that could benefit a larger array of consumers Desire to promote evidence informed consumer driven services

90
Transdiagnostic Skills
Critical pieces of outcome success Offering Voice and Choice (Duncan, Miller, Wampold, & Hubble, 2010)
")
91
Common Factors Relationship factors Motivation
Clarity of expectations of treatment Are common to any psychotherapy, regardless of treatment modality or model (Bickman, 2005; Kelley, Bickman, & Norwood, 2010; Karver, Handelsman, Fields, & Bickman, 2005; 2006)
")
92
Successful treatment models embrace these factors and incorporate them as part of their foundation.

93
Collaborative Approach to Treatment Planning Shared Vision of Goals
Actively engaging the client and family in the treatment planning process has been connected to improved outcomes of treatment (Bohart & Tallman, 2010). Consumer and Counselor Work together to identify and clarify goals Co-develop strategies for achieving goals Goals and strategies are negotiated and shared together rather than imposed by professionals. Plans are regularly reviewed and revised as goals develop, are achieved, or as strategies change.
. Consumer and Counselor. Work together to identify and clarify goals. Co-develop strategies for achieving goals. Goals and strategies are negotiated and shared together rather than imposed by professionals. Plans are regularly reviewed and revised as goals develop, are achieved, or as strategies change.")
94
Trauma Informed Phase Oriented Skills

95
Core areas of focus in Complex Trauma Courtois, C. & Ford, J
Core areas of focus in Complex Trauma Courtois, C. & Ford, J. (2009), Introduction (p.2) Self-Regulation Affect Regulation Disassociation (difficulty in being “present”) Somatic Dysregulation Self-Identity Impaired Self-Concept Impaired Self-Development Co-regulation Secure working model of caring relationship Disorganized Attachment Patterns Information and slide part of Dr. Allison Sampson's Trauma Presentation
, Introduction (p.2) Self-Regulation. Affect Regulation. Disassociation (difficulty in being present ) Somatic Dysregulation. Self-Identity. Impaired Self-Concept. Impaired Self-Development. Co-regulation. Secure working model of caring relationship. Disorganized Attachment Patterns. Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
96
Contextual Models of Care Gold, S. (2009) pp.231-235
Interpersonal Area Collaborative approach Attachment in the therapeutic relationship Practical Area Skill Development Self-Soothe Being in the Present Cognitive Strategies (problem solving) Release of addiction/maladaptive behaviors Traumatic Stress Reprocessing Engaging in Daily Life Conceptual Area Clinician is a guide through the process Client develops the conclusions and outcomes Information and slide part of Dr. Allison Sampson's Trauma Presentation
 Release of addiction/maladaptive behaviors. Traumatic Stress Reprocessing. Engaging in Daily Life. Conceptual Area. Clinician is a guide through the process. Client develops the conclusions and outcomes. Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
97
NCTSN Guidance on Components of Trauma Informed Treatment
Building a strong therapeutic relationship Affect expression and regulation skills Anxiety management Relaxation skills Cognitive processing/reframing Construction of a coherent trauma narrative Strategies that allow exposure to traumatic memories and feelings in tolerable doses so that they can be mastered and integrated into the child’s experience Personal safety/empowerment activities Resiliency and closure

98
Understand what good trauma treatment looks like …
Phase Oriented Treatment “ Gold Standard” Phase I: Safety and Stabilization Phase 2: Trauma Reprocessing Phase 3: Reintegration Handout on questions to ask Mental Health Providers Resource Information and slide part of Dr. Allison Sampson's Trauma Presentation

99
Phase Oriented Treatment Phase Oriented Treatment for Trauma (Herman 1992, Janet 1889) from Courtois, C. “Treating Complex Traumatic Stress Disorders” PHASE ONE: Safety and Stabilization Personal and Interpersonal Safety Established: Education/Support/Safety Planning Enhance Client’s ability to manage extreme arousal (hyper/hypo) Active engagement in positive/negative experiences (deal with automatic avoidance behaviors, self awareness of avoidance, increase coping skills and use of coping skills) Education (psychotherapy, trauma, skills to be learned) Assess and develop relationship capacity (decrease avoidance of relationships or negative thoughts about relationships, build support network, define client’s attachment network) Information and slide part of Dr. Allison Sampson's Trauma Presentation
 Active engagement in positive/negative experiences (deal with automatic avoidance behaviors, self awareness of avoidance, increase coping skills and use of coping skills) Education (psychotherapy, trauma, skills to be learned) Assess and develop relationship capacity (decrease avoidance of relationships or negative thoughts about relationships, build support network, define client’s attachment network) Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
100
Phase Oriented Treatment Phase Oriented Treatment for Trauma (Herman 1992, Janet 1889) from Courtois, C. “Treating Complex Traumatic Stress Disorders” PHASE TWO: Trauma Reprocessing Disclosure of traumatic memories, development of an autobiographical narrative (identify emotions connected to trauma memories, grieve and mourn losses, resolution of relationships when appropriate, increased awareness, increase interpersonal and self-regulation skills) Supporting client in maintaining functioning and not getting lost in memories or seeing themselves as “disabled”, need to affirm strengths, promote positive self-esteem, and internal and external resources now available to them PHASE THREE: Re-Integration Growth and period and reengagement in life Can be time of client realizing losses, discover of unresolved developmental deficits, fine tuning of self-regulation skills
 Supporting client in maintaining functioning and not getting lost in memories or seeing themselves as disabled , need to affirm strengths, promote positive self-esteem, and internal and external resources now available to them. PHASE THREE: Re-Integration. Growth and period and reengagement in life. Can be time of client realizing losses, discover of unresolved developmental deficits, fine tuning of self-regulation skills.")
101
Other critical factors

102
Bolstering strengths and resilience “Ask what’s strong, not what’s wrong” Tell the “thriver story”

103
Post-Traumatic Growth Tedeschi and Calhoun (1996, 1999, 2006)
Emergence of new opportunities and possibilities Deeper relationships and greater compassion for others Feeling strengthened to meet future life challenges Reorder priorities and fuller appreciation of life Deepening spirituality Information and slide part of Dr. Allison Sampson's Trauma Presentation

104
Resilience Trumps Aces
From Trish Mullen, Chesterfield Community services Board

105
Gathering feedback … “voice” Collecting meaningful in process data and using it with consumers weekly in shared decision making process

106
CONSUMER Lived Experience of Consumer and Family Recovery Truth
Consumer Driven Best Practice Development of Life Plan (Collaboration) Consumer Markers (mindfulness) Feedback and Personal Evidence Outcomes and Emerging Best Practice Evidence from Research CONSUMER
 Consumer Markers (mindfulness) Feedback and Personal Evidence. Outcomes and Emerging Best Practice. Evidence from Research. CONSUMER.")
107
Exemplars of Measures -NCTSN and Chadwick Guidance on measures
AIM Forward Battery Weekly measures (A and B) and monthly measures Exemplar of Case How data is organized and gathered PTTB if possible, can bring in Diary Card models, show screen shots of EHR … make sure EPOW collects measures that are in line with Common Factors and have symptoms and strength based measures
 and monthly measures. Exemplar of Case. How data is organized and gathered. PTTB if possible, can bring in Diary Card models, show screen shots of EHR … make sure EPOW collects measures that are in line with Common Factors and have symptoms and strength based measures.")
108
Incorporating Measures
Collaborative Treatment Planning and Tracking of Strategy Success (outcomes) Demonstrate Dani Baldwin and example of how we bring these measures into the treatment planning process and into goal writing …
 Demonstrate Dani Baldwin and example of how we bring these measures into the treatment planning process and into goal writing …")
109
Examples Diary Card Re-authorization - EHR

110
But Feedback is Still in the Early Stages of Development
Feedback is Still in Early Stages of Development

111
Professional Development
Foundational Learning Series and focus on competency 17.75 hours of education in transdiagnositic factors with special emphasis on collaborative treatment planning and goal setting Additional 20 hours of education for clinical supervisors on most recent evidenced approaches to clinical supervision

112
Professional Development
Trauma Perspective Series and Competency 19.5 hours of training in latest evidence informed methods of working with complex forms of traumatic lived experiences Courses have been developed over last 10 years Research study using multivariate analysis conducted in demonstrated efficacy in changing the knowledge, attitudes and assessment and intervention behaviors of behavioral healthcare professionals Evidence informed professional development model Courses continually modified with latest research and taught by an expert in the field Content focuses on defining trauma, relevance of ACE studies, attachment theories, neuroscience to work with consumers, models for teaching consumers latest evidence on trauma, engaging consumers and families in phase oriented care

113
AIM Forward ORGANIZATIONAL INVESTMENT IN IMPROVING TRAUMA INFORMED CARE

114
AIM Forward … Part of a National Demonstration Project for Trauma Informed Programs with National Technical Assistance Center for Children’s Mental Health (Georgetown University) In partnership with the National Council of Behavioral Healthcare to further AIM Forward initiatives and trauma informed care within our organization Collecting data on program’s impact Letting consumers, families, and stakeholders know about the program and opportunities
 In partnership with the National Council of Behavioral Healthcare to further AIM Forward initiatives and trauma informed care within our organization. Collecting data on program’s impact. Letting consumers, families, and stakeholders know about the program and opportunities.")
115
Trauma Informed Organization
Domain 1. Early Screening and Comprehensive Assessment of Trauma Domain 2. Consumer Driven Care and Services Domain 3. Trauma-Informed, Educated and Responsive Workforce Domain 4. Provision of Trauma-Informed, Evidence Based and Emerging Best Practices Domain 5. Create a Safe and Secure Environment Domain 6. Engage in Community Outreach and Partnership Building Domain 7. Ongoing Performance Improvement and Evaluation Information and slide part of Dr. Allison Sampson's Trauma Presentation

116
FAMILY PRESERVATION SERVICES

117
Domain 6 – TICN Development
Recognizing that the children and families we serve may be part of a larger service system, community collaboration is a key element of being a trauma informed organization. Important linkages may include: housing corrections courts primary health emergency care social services education mental health treatment services use programs The TIC Community Partnership Network invites trauma informed system stakeholders to meet and shape the continuum of trauma informed care services within a community.

118
Committee Development
Service gap surveys Provider service books with TIC services listed Higher Education Development/Certification Outcomes Groups Provider Certification Committees Communication Groups Screening and Assessment Best Practice Development of Case Planning Integration processes for Child Welfare Workers and Juvenile Justice Workers Education and Training Resources (including people)
")
119
Community Education and Collaboration
Department of Criminal Justice Department of Social Services (child and family) Department of Education Law Schools and Clinics Juvenile Domestic Relation Courts Department of Mental Health Learning Collaborative Child Advocacy Agencies Adoption Advocacy Agencies Local Schools Parent/caregiver groups School Administration Consumer Conferences Judge’s Conferences Court Service Units Truancy Officers
 Department of Education. Law Schools and Clinics. Juvenile Domestic Relation Courts. Department of Mental Health. Learning Collaborative. Child Advocacy Agencies. Adoption Advocacy Agencies. Local Schools. Parent/caregiver groups. School Administration. Consumer Conferences. Judge’s Conferences. Court Service Units. Truancy Officers.")
120
10 percent of the work done …90 percent to go What will you do ?
Understanding what we can do even better …

121
What is next for your agency?
Trauma Informed Care is a Shift in Paradigm and a lens you can use to define the way you Screen and Assess children and families Gather information from clients and families about the services they need and are receiving from you Educate your workforce Make decisions about referrals to trauma informed and evidence informed programs Create safe and secure environments (physically and emotionally) Engage in Community Outreach and Partnership Building Make decisions about ongoing performance of your work, your agency and the quality of the work you offer Information and slide part of Dr. Allison Sampson's Trauma Presentation
 Engage in Community Outreach and Partnership Building. Make decisions about ongoing performance of your work, your agency and the quality of the work you offer. Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
122
Guided discussion … you harness?
When you get back to your offices, we you to schedule a time to think about what you want to do next? What is your biggest take away so far from today … what resonates? Where do you want to start to enhance the trauma informed services you provide in your role? Your agency? you harness? What resources do you need? Who are your partners ? What types of education and development tools will you and your workforce need? Brainstorm and create 3 next action steps for yourself and your agency Information and slide part of Dr. Allison Sampson's Trauma Presentation

123
Use of SOAR Strategic Planning
What STRENGTHS do you have in place to address 7 domains What OPPORTUNITIES for change (barriers) are present to address 7 domains What will your ACTION steps be (within and between agencies) What RESULTS do you expect in 3 months, 6 months, 9 months, next year ? Information and slide part of Dr. Allison Sampson's Trauma Presentation
 are present to address 7 domains. What will your ACTION steps be (within and between agencies) What RESULTS do you expect in 3 months, 6 months, 9 months, next year Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
124
Resilience Trumps Aces
From Trish Mullen, Chesterfield Community services Board

125
Bolster Protective Factors
Positive attitudes, values or beliefs Conflict resolution skills Good mental, physical, spiritual and emotional health Positive self-esteem Success at school Good parenting skills Parental supervision Strong social supports Community engagement Problem-solving skills Positive adult role models, coaches, mentors Healthy prenatal and early childhood development Participation in traditional healing and cultural activities Good peer group/friends Steady employment Stable housing Availability of services (social, recreational, cultural, etc)
")
126
Families who Thrive Clear acceptance of stressor(s)
Characteristics of Families who Thrive Figley and Kiser (2013) Helping Traumatized Families (pg ) Clear acceptance of stressor(s) Family centered locus of problem (shift from individual) Solution oriented problem solving (not blame) High tolerance for each other Clear and direct expressions of commitment and affections Open and Effective Communication High Family Cohesion (fun and enjoyment) Flexible Family Roles Predictability Effective resource utilization Belief in their ability to succeed Shared meaning (collaborative coping skills)
 Helping Traumatized Families (pg ) Clear acceptance of stressor(s) Family centered locus of problem (shift from individual) Solution oriented problem solving (not blame) High tolerance for each other. Clear and direct expressions of commitment and affections. Open and Effective Communication. High Family Cohesion (fun and enjoyment) Flexible Family Roles. Predictability. Effective resource utilization. Belief in their ability to succeed. Shared meaning (collaborative coping skills)")
127
Distress Tolerance

128
Vulnerability Mountain

129
Trauma-Informed Care: What Hurts and What Helps?

130
What Hurts and What Helps? The importance of relationships
Interactions that are humiliating, harsh, impersonal, disrespectful critical, demanding, judgmental WHAT HELPS? Interactions that express kindness, patience, reassurance, calm and acceptance and listening Frequent use of words like PLEASE and THANK YOU How can we avoid re-traumatization?

131
The importance of the physical environment
WHAT HELPS? Comfortable, calming, and private treatment and waiting. Furniture is clean and comfortable No wrong door philosophy Integrated restrooms Messages conveyed throughout that are positive and hopeful WHAT HURTS? Congested areas that are noisy Poor signage that is confusing Uncomfortable furniture Separate bathrooms Cold non-inviting colors and paintings/posters on the wall

132
The importance of policies and procedures
WHAT HURTS? Rules that always seem to be broken Policies and Procedures that focus on organizational needs rather than on client needs Documentation with minimal involvement of clients Many hoops to go through before a client’s needs are met Language and cultural barriers WHAT HELPS? Clear, sensible and fair rules (focus on what you CAN DO rather than what you CAN’T) Transparency in documentation and service planning Communication in the person’s language Continual feedback from clients about their experience in the program
 Transparency in documentation and service planning. Communication in the person’s language. Continual feedback from clients about their experience in the program.")
133
The importance of our attitudes and beliefs
WHAT HURTS? Asking questions that convey the idea that “there is something wrong with the person” Judgments and prejudices based on cultural ignorance Regarding a person’s difficulties only as symptoms of a mental health, substance use or medical problem WHAT HELPS? Asking questions for the purpose of understanding what harmful events may contribute to current problems Understanding the role of culture in trauma response Recognizing that symptoms are often a persons way of coping with trauma or are adaptations

134
What are the Benefits of Adopting Trauma-Informed Approaches?
Increases safety for all Improves the social environment Cares for the caregivers Improves the quality of services Reduces negative encounters and events Creates a community of hope, healing and recovery Increases success and satisfaction at work Promotes organizational wellness Improves the bottom line

135
DISTRESS TOLERANCE

136
Distress tolerance skills (taken from the Accepts skills … DBT informed)
o Activities (physical and mental) – mental vacation, bi-lateral movement (walking), temperature change o Contributing – helping others gets you out of yourself and your stress (smiling, give compliment, invite someone to coffee, hold a door, do a favor) o Comparisons – Bringing perspective to current situation, what skills have helped you cope before (have helped your children cope before) … validate yourself o Emotions – Seek out activities that create feelings that are OPPOSITE from the painful ones you are experiencing (listen to music, favorite movie, work on a project --- favorite hobby) o Push Away – Put away distressing memories in a “lock box” or in the “parking lot” for a little while … can do this in writing or mentally o Thoughts – distract your thoughts with “one-thing” exercises, read something inspiring, “just worrying exercise” o Sensations – Any physically vigorous activity or actively awakening senses (brisk walk, cold bath/hot bath, splash cold water on face, lotions on your wrist, strong taste, bold colors (Mandela), music) Pederson, L. (2012). The Expanded Dialectical Behavioral Therapy Skills Training Manual . Eau Claire: CMI Education Institute, Inc. pp
 – mental vacation, bi-lateral movement (walking), temperature change. o Contributing – helping others gets you out of yourself and your stress (smiling, give compliment, invite someone to coffee, hold a door, do a favor) o Comparisons – Bringing perspective to current situation, what skills have helped you cope before (have helped your children cope before) … validate yourself. o Emotions – Seek out activities that create feelings that are OPPOSITE from the painful ones you are experiencing (listen to music, favorite movie, work on a project --- favorite hobby) o Push Away – Put away distressing memories in a lock box or in the parking lot for a little while … can do this in writing or mentally. o Thoughts – distract your thoughts with one-thing exercises, read something inspiring, just worrying exercise o Sensations – Any physically vigorous activity or actively awakening senses (brisk walk, cold bath/hot bath, splash cold water on face, lotions on your wrist, strong taste, bold colors (Mandela), music) Pederson, L. (2012). The Expanded Dialectical Behavioral Therapy Skills Training Manual . Eau Claire: CMI Education Institute, Inc. pp")
137
When you Leave here today …
Use the ACCEPTS Model … Think through activities that will fall under 2 of these categories that you could use with kids and families you work with at work

138
When Downstairs Brain Active … and right brain emotion in gear
Remember Connect … Then Redirect Tone of voice, facial expression, empathic talking, pausing …

139
Practice Examples Distress Tolerance “Down Stairs Brain”
Temperature Change Grounding by looking up Bi-lateral movement Butterfly taps Compassion Hold

140
Compassion Fatigue Who is taking care of you ??
Information and slide part of Dr. Allison Sampson's Trauma Presentation

141
Mirror Neurons

142
Stress within and between our systems
Within and between human service organizations we witness fight flight and freeze When we think about where this comes from … it is very similar to the experience of our clients We bring in our own ACE scores Our environments are stressful, demanding and sometimes abusive Budget Cuts Higher Caseloads Increase paperwork demands Higher expectations for outcomes and evidence informed practices Constantly changing regulations Not having the resources we need within our organization to get the work done Pay freezes and lower pay for very challenging work Vicarious Trauma with and through our clients Information and slide part of Dr. Allison Sampson's Trauma Presentation

143
So we develop coping behaviors to survive within and between the systems
Remember … the “problems” we see in our clients are often their solutions to coping with stress and trauma Our challenges in and between our systems are often the way we cope within and between our agencies Fight/Flight/ Freeze can be our coping behaviors too Information and slide part of Dr. Allison Sampson's Trauma Presentation

144
Cross-System Challenges
Adversarial Relationships Blaming other people or departments for …. Lack of Communication Avoiding Communication with certain People or Agencies Staying close only to those in “our circle” Doing nothing (waiting for the storm to pass) Information and slide part of Dr. Allison Sampson's Trauma Presentation
 Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
145
Cross System Challenges can also be because of …
Lack of Knowledge Lack of Awareness Lack of True Collaboration Lack of Resources Information and slide part of Dr. Allison Sampson's Trauma Presentation

146
When our agencies behave in this way with one another … our clients and families model what we are doing and our often further traumatized … EMOTIONAL CHAIN OF CUSTODY Information and slide part of Dr. Allison Sampson's Trauma Presentation

147
Examples of System Re-traumatization
Uses of touch (lack of it, painful touch) Questioning that is repetitive or triggering Approaches that minimize experiences of client and family Planning that does not ask the client and family for their input Making decisions before the client and family come in the room while still saying it is a “collaborative process” Information and slide part of Dr. Allison Sampson's Trauma Presentation
 Questioning that is repetitive or triggering. Approaches that minimize experiences of client and family. Planning that does not ask the client and family for their input. Making decisions before the client and family come in the room while still saying it is a collaborative process Information and slide part of Dr. Allison Sampson s Trauma Presentation.")
148
Impact of Working with Victims of Trauma
Trauma experienced while working in the role of helper has been described as: Compassion fatigue Countertransference Secondary traumatic stress (STS) Vicarious traumatization Unlike other forms of job “burnout,” STS is precipitated not by work load and institutional stress but by exposure to clients’ trauma. STS can disrupt child welfare, police and juvenile justice workers’ lives, feelings, personal relationships, and overall view of the world. 106 106
 Vicarious traumatization. Unlike other forms of job burnout, STS is precipitated not by work load and institutional stress but by exposure to clients’ trauma. STS can disrupt child welfare, police and juvenile justice workers’ lives, feelings, personal relationships, and overall view of the world")
149
WHO WILL HEAL THE HERO ???

150
Impact of Chronic Stress http://www.helpguide.org/mental/stress_signs.htm
raise blood pressure suppress immune system increase the risk of heart attack and stroke contribute to infertility speed up the aging process (life expectancy) create vulnerability for anxiety and depression obesity skin conditions (ex: eczema) sleep problems digestive problems
 create vulnerability for anxiety and depression. obesity. skin conditions (ex: eczema) sleep problems. digestive problems.")
151
Managing Stress when working with you and families who have experienced trauma
Request and expect regular supervision and supportive consultation. Utilize peer support. Consider therapy for unresolved trauma, which the child welfare work may be activating. Practice stress management through meditation, prayer, conscious relaxation, deep breathing, and exercise. Develop a written plan focused on maintaining work–life balance. 107 107

152
Self Care: Need Options
Time and Connection: 10 second exercises 2 minute exercises 5-10 minute exercises 20-30 minute GI, Walking Meditation

153
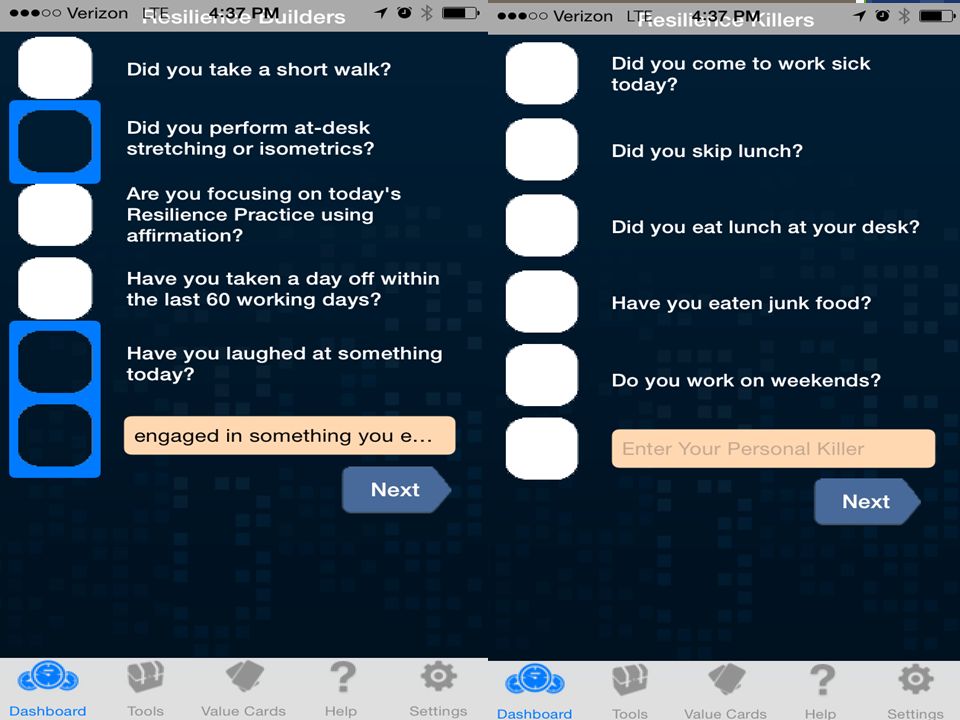
Self Care Apps Provider Resilience GPS for the Soul
Ichill app (Peter Levine work) Mediation Oasis Apps Mindfulness Training System Narrative Therapy Questions NCTSN Self Care Inventory
 Mediation Oasis Apps. Mindfulness Training System. Narrative Therapy Questions. NCTSN Self Care Inventory.")
154
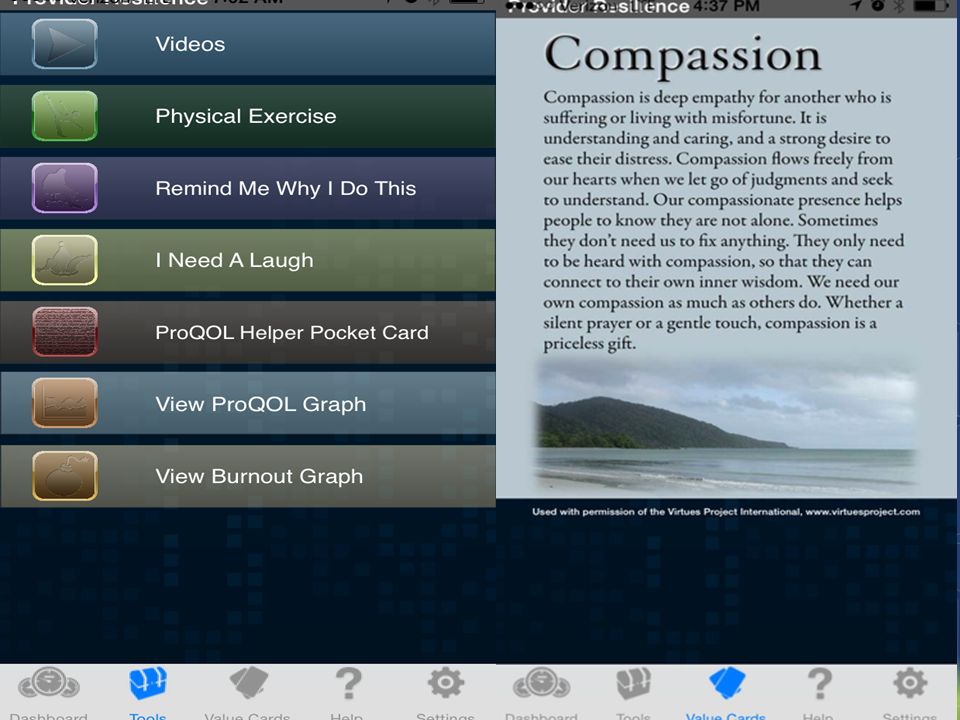
Provider Resilence

155
Provider Resilence

158
GPS for the Soul

162
FLIPOGRAM

163
Pocket TM … by Trish Mullen, LPC
Challenge: Working with children who are in their downstairs brain and getting them back up to their upstairs brain … when we all use primarily upstairs techniques in our work … Self care targeted to the right brain and lower brain … HAPPY PLACE

164
Caring For Yourself

165
Creating Internal Awareness

167
Creating Awaresness

168
Window of Tolerance Pat Ogden

169
Using Grounding Techniques to Stay in the Window of Tolerance
Mental Grounding Physical Grounding Soothing Grounding Somatic Grounding Najavitis, L.M. (2002). Seeking safety: A treatment manual for PTSD and substance abuse. NY: Guilford.
. Seeking safety: A treatment manual for PTSD and substance abuse. NY: Guilford.")
170
“Dig where the ground is soft” Chinese proverb
Conclusion: “Dig where the ground is soft” Chinese proverb Instead of picking your trickiest area, pick the issue that you can most easily visualize improving on. (e.g.: “making a commitment to going for a walk every lunch time vs. getting rid of my difficult supervisor”). You may not notice it right away, but making one small change to your daily routine can have tremendous results in the long term. Imagine if you started walking up two flights a stairs per day instead of using the elevator, what might happen after three months?
. You may not notice it right away, but making one small change to your daily routine can have tremendous results in the long term. Imagine if you started walking up two flights a stairs per day instead of using the elevator, what might happen after three months")
171
Questions…. “…We are stewards not just of those who allow us into their lives but of our own capacity to be helpful...” TRISH MULLEN, LPC (804)
")
172
Light and Dark … My story …

173
Hands in …. What will you do to support trauma informed recovery ???

174
THANK YOU …… Dr. Allison Sampson-Jackson Family Preservation Services, Inc

Similar presentations