Download presentation
Presentation is loading. Please wait.

1
The When, How, and Where to of Trauma Screening, Assessment, and Referral

2
Primary prevention requires the provision of safe, nurturing relationships for all children. Attention to care giving system is essential

3
Secondary prevention requires: Early identification of young children and youth who are exposed to traumatic events Timely effective intervention to create or reestablish safety and self-regulation Minimize lasting physiological and psychological harm

4
Pre-event functioning Previous traumatic experience Previous psychological condition Period of post event return to baseline Age: both ends of the spectrum Perceived threat to self or family Lack of resources Initial response to the event

5
Psychological Trauma Crisis Event Threat Perceptions Crisis Exposure Crisis Reactions Personal Vulnerability Assessment of Psychological Trauma

6
High levels of dissociation Flashbacks Nightmares Extreme withdrawal from others Difficulty returning to baseline Severity interferes with functioning May indicate need for additional support and services

7
Functional Screens Less on event or events more on impact of event Samples TSI Belief Scale (Traumatic Stress Institute, South Windsor, CT.) Primary Care PTSD Screen (PC-PTSD) (Prins, Oulmette, Kemerling et al., 2003) Event based Screens An Interview for Children: Traumatic Events Screening Inventory (TESI-C) (The Nat’l Ctr for PTSD, Dartmouth Child Trauma Research Group, 2008) Screening questions ▫a. Have you ever been in a situation when you thought that you might die or be seriously injured (hurt very badly?) ▫b Have you ever seen something terrible happen to someone else and you thought that the person might die or be seriously injured?
 ▫b Have you ever seen something terrible happen to someone else and you thought that the person might die or be seriously injured .")
8
Ongoing relationship is central If we ask the question we ‘own the answer’ Knowing your community’s resources is essential Strategies for managing our response part of a trauma informed system

9
Assessment and treatment should be comprehensive w/ a team of caregivers and providers involved. Caregivers should be trained to recognize behavioral changes that may be associated with trauma due to communication issues and difficulty reporting.

10
Support and promote positive and stable relationships in the life of the child. Provide support and guidance to child’s family and caregivers. Manage professional and personal stress Trauma-informed child mental health practice mirrors well-established child mental health priorities.

11
Trauma Treatment should be phase oriented 1. Stabilization 2. Processing the effects of the trauma 3. Integration Child and Family Trauma Treatment Psychoeducation Family involvement Systems involvement Symbolic ways to tell the story Play therapy Expressive Arts therapies

12
Managing Feelings (Recognizing, Modulating, Tolerating, Integrating) Inner Connection to Others Feeling worthy of life
 Inner Connection to Others Feeling worthy of life")
13
C.L.E.A.R.E.D. Create something (food, art, photography….) Love your family, spouse, and pets and spend lots of time with them Exercise at least 3 times per week Avoid excess in anything (food, caffeine, alcohol, exercise, work…) Relax with a good book, and schedule “nothing” time Eat healthy food Dream about your goals and envision the future you want for yourself and your family
 Love your family, spouse, and pets and spend lots of time with them Exercise at least 3 times per week Avoid excess in anything (food, caffeine, alcohol, exercise, work…) Relax with a good book, and schedule nothing time Eat healthy food Dream about your goals and envision the future you want for yourself and your family.")
14
Women with co-occurring PTSD/Substance Abuse are more likely to have experienced childhood abuse. Men with co-occurring PTSD/Substance Abuse more frequently experienced crime and or war trauma. PTSD symptoms are often a trigger for substance abuse (self medication). Victims are more vulnerable to re-victimization when using substances ( Substance Abuse Treatment for Persons with Co-Occurring Disorders SAMHSA, 2005 )
. Victims are more vulnerable to re-victimization when using substances ( Substance Abuse Treatment for Persons with Co-Occurring Disorders SAMHSA, 2005 ).")
15
75% of persons in substance abuse were victims of physical or sexual violence (SAMHSA, 2000). Dual diagnosis for PTSD and substance abuse ranges from 12-34% for men and 30-59% for women (Brown and Wolfe, 1994). 55-99% of Women with substance abuse problems report physical and/or sexual abuse histories. (Najavits et al., 1997).
. 55-99% of Women with substance abuse problems report physical and/or sexual abuse histories. (Najavits et al., 1997)..")
16
PTSD symptoms may become worse with abstinence. Treatment outcomes are worse for people with PTSD and Substance Abuse than for other dual-diagnosis clients. Treatments that are effective for PTSD or substance abuse separately may not be advisable when the two issues co-occur. Stabilization phase only until sobriety is achieved

19
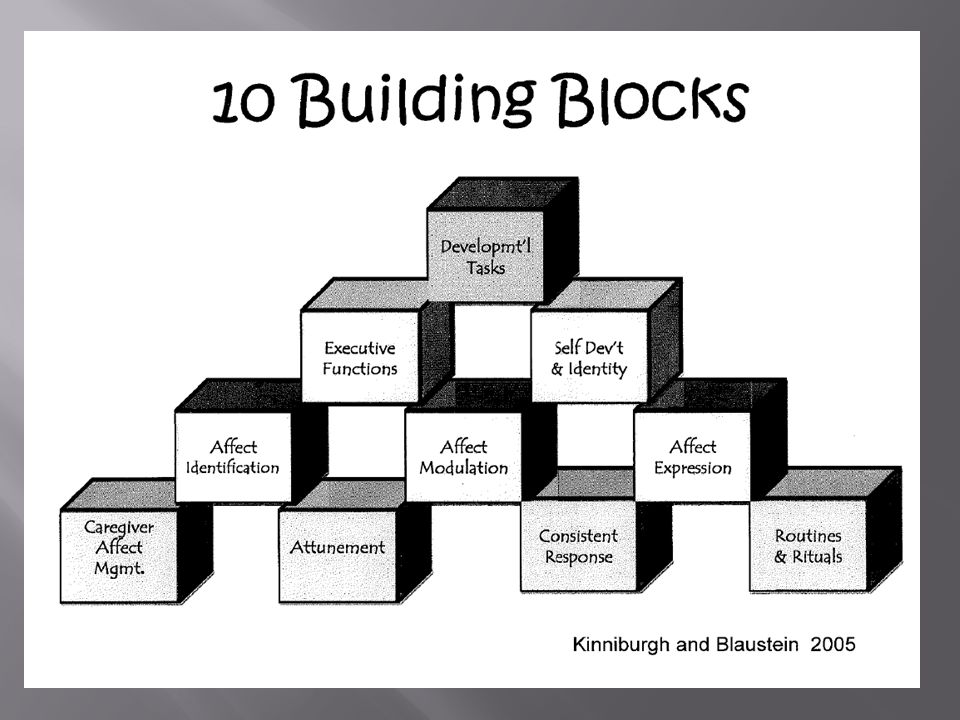
Figure 1. Attachment, self-regulation, and competency (ARC): A framework for intervention with complexly traumatized youth. Adapted from “Attachment, Self-Regulation, and Competency: A Comprehensive Framework for Intervention With Complexly Traumatized Youth. A Treatment Manual,” by K. Kinniburgh and M. Blaustein, 2005, p. 426. Copyright 2005 by authors. Reprinted with permission.Kinniburgh and M. Blaustein, 2005
: A framework for intervention with complexly traumatized youth. Adapted from Attachment, Self-Regulation, and Competency: A Comprehensive Framework for Intervention With Complexly Traumatized Youth. A Treatment Manual, by K. Kinniburgh and M. Blaustein, 2005, p Copyright 2005 by authors. Reprinted with permission.Kinniburgh and M. Blaustein,")
Similar presentations















 Thorbjorg Sveinsdottir MSc Psychology Barnahus 31. mai.>")






