Download presentation
Presentation is loading. Please wait.

1
An Approach to Abdominal Pain in the ED Nisarg Shah MD, FACEP

2
Introduction Complaints related to abdominal pain comprise between 5-7% of all visits to the ED. Of those, the most common discharge diagnosis is Abdominal Pain NOS. Although most abdominal pain is non-emergent and self-limited in nature, attention must be paid to not miss medical and/or surgical emergencies.

3
Important Factors Patients rarely present with the classical signs/symptoms of acute abdominal pain. Three important factors to consider are age, gender, and co-morbidities.

4
Age differences Greater than 50 Biliary disease NOS Appendicitis Bowel obstruction Pancreatitis Diverticular disease Cancer Less than 50 NOS Appendicitis Biliary tract disease Gynecologic Pancreatitis Bowel obstruction

5
Gender differences Males Perforated ulcer Gastritis Appendicitis Females Nonspecific Diverticulitis Acute cholecystitis Gynecologic

6
Comorbidities Immunocompromised i.e. age, steroids, HIV, sickle cell disease, malignancy CAD, Atrial fibrillation, Peripheral vascular disease Diabetes Dementia Multiple surgeries

7
Types of Pain Visceral Pain: caused by stretching of fibers innervating the walls of hollow organs or capsules of solid organs, described as crampy or dull pain Parietal Pain: caused by irritation of fibers that innervate the parietal peritoneum, pain is more sharp and localized Referred Pain: pain at a location distant to the diseased organ based on embryonological origin

8
History Most diagnoses can be made by history alone. Careful attention must be paid to: Time/mode of onset Duration Location Character/progression Medical history Contributing symptoms

9
Caveat Although we can agree that history is usually the most important part of the encounter, urgent determination of potential surgical emergencies is essential.

10
History – time/mode of onset Woken up from sleep Abrupt/severe versus gradual Less severe but increasing Gradual onset with slow progression Intermittent pain Associated with certain activities – eating or exercise

11
History-Duration Acute onset of pain vs. chronic pain Acute, severe, and worsening pain suggests a surgical disorder Very long duration often, but not always, suggests a less acute cause

12
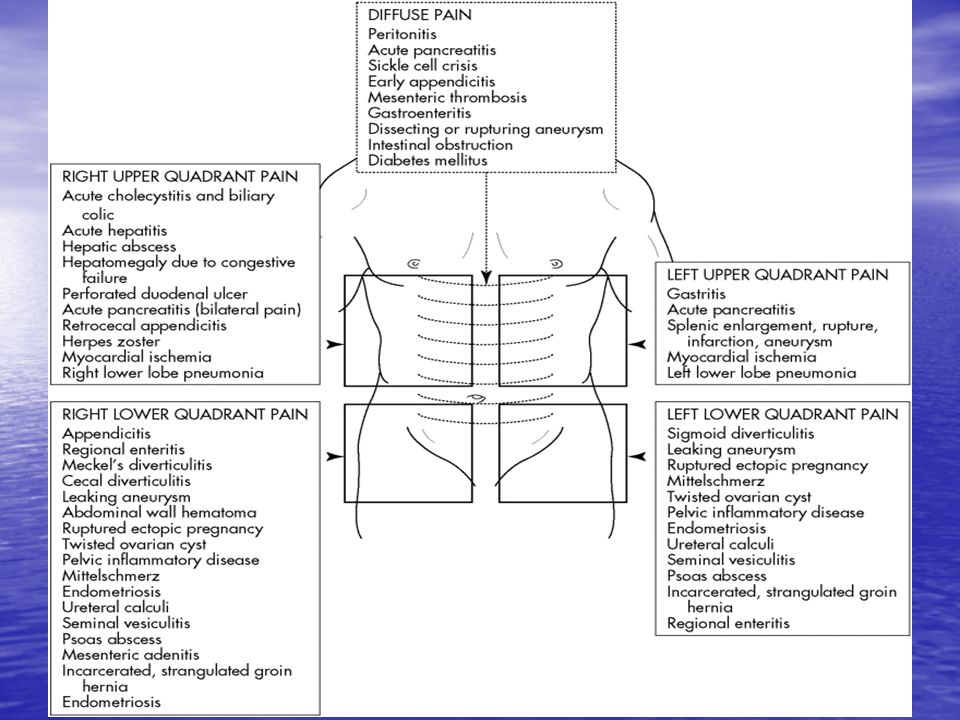
History-Location Four basic quadrants Right upper quadrant Right lower quadrant Left upper quadrant Left lower quadrant Three central areas Epigastric Periumbilical Suprapubic

13
History-Character/Progression Severity/magnitude of stimulus Intermittent crampy Severe and colicky Sudden increase Sudden change in sensation or location

14
Medical History Previous surgery Sexual activity Menstrual history Travel Exposure risk/occupation Psychiatric Medications Comorbidities

15
History-Contributing Symptoms Anorexia Vomiting (bilious? blood?)/Nausea Diarrhea Bleeding Constipation Obstipation Dysuria SOB Chest pain
/Nausea Diarrhea Bleeding Constipation Obstipation Dysuria SOB Chest pain.")
16
Physical Examination The exam serves several important purposes To confirm suspicions from the history To localize the area of disease To avoid missing extra-abdominal causes of pain

17
Physical Examination General appearance including facial expression, diaphoresis, pallor, and degree of agitation to distinguish the intensity of the pain Vital signs

18
Physical Examination Inspection: look for distention, ecchymosis, scars, hernias Auscultation: listen for bowel sounds, pitch, bruits Palpation: feel for guarding, masses, tenderness, rebound Percussion: liver size, tympany

19
Differential Diagnosis The next important step in the evaluation of abdominal pain is to formulate a differential diagnosis It is helpful to construct a list based upon location of abdominal pain

21
Laboratory Evaluation Dependent upon initial history and physical examination Most frequently ordered study is the CBC Additional studies may include electrolytes, amylase, lipase, LFTs, BUN, creatinine, urinalysis, Beta Hcg, lactic acid EKG

22
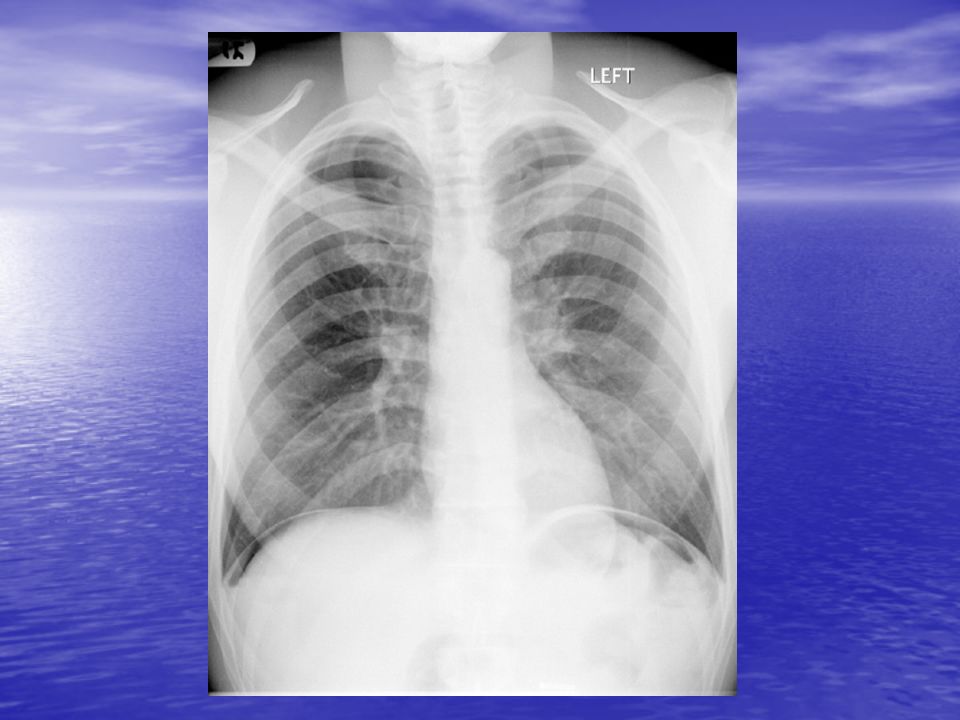
Imaging Studies Plain films: CXR or Upright pCXR Abdominal series

23
Imaging studies cont’d CXR help determine the following: Abdominal pain of pulmonary origin - pneumonia with diaphragmatic irritation Free air under diaphragm - perforated viscous Air filled viscera in chest – diaphragmatic or hiatal hernia Mediastinal air - Boerhave’s tear

25
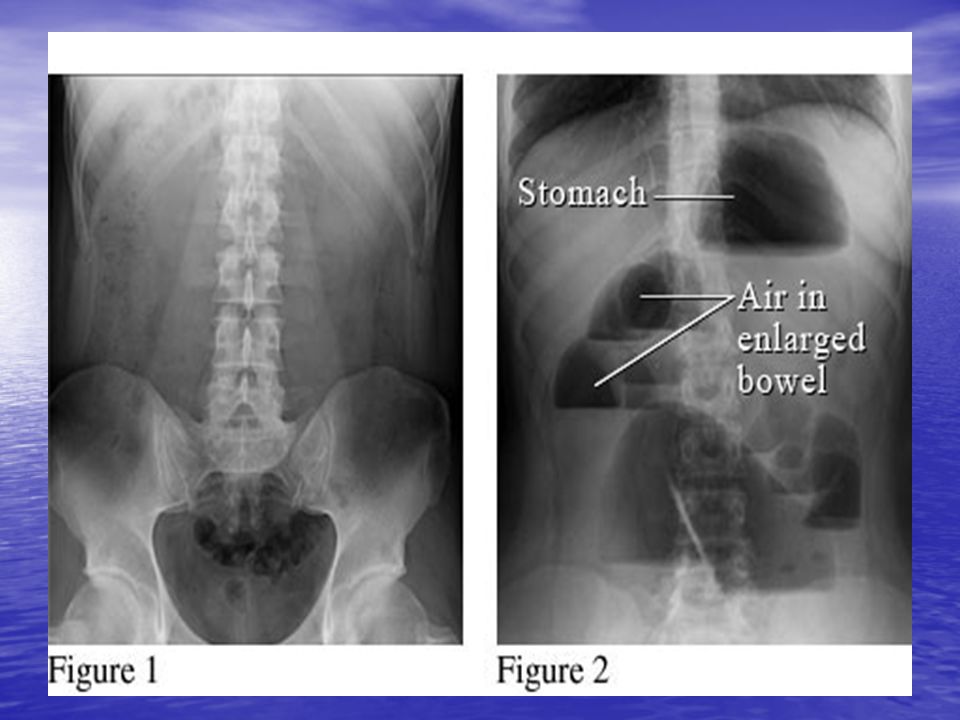
Imaging studies cont’d Abdominal films can help with: Fluid filled loops/air fluid levels – obstruction Renal calculi Gallstones or air in the biliary tree Massive dilation of colon Lots of stool

27
Imaging This person most likely has Large bowel obstr. Small bowel obstr. Generalized ileus Localized ileus Normal bowel gas pattern

28
Imaging This person most likely has Large bowel obstr. Small bowel obstr. Generalized ileus Localized ileus Normal bowel gas pattern

29
Imaging This person most likely has Large bowel obstr. Small bowel obstr. Generalized ileus Localized ileus Normal bowel gas pattern

30
Imaging This person most likely has Large bowel obstr. Small bowel obstr. Generalized ileus Localized ileus Normal bowel gas pattern

31
Imaging This person most likely has Large bowel obstr. Small bowel obstr. Generalized ileus Localized ileus Free intraperitoneal air

32
Imaging Pneumobilia after passage of a gallstone. Take a good look at the liver where the biliary tract is outlined by air. Pneumobilia

33
Imaging

34
Imaging

35
Imaging studies cont’d Likelihood ratio of finding abnormality on xray is increased by Increased/high pitched bowel signs Distention History of abdominal surgery Blood in urine/history of kidney stones Severe abdominal pain and tenderness Abdominal pain for less than one day

36
Imaging studies cont’d Sonography is the study of choice for: Biliary/hepatobiliary disease Pregnant women Evaluation of gynecologic structures – ovarian as well as testicular Rapid evaluation of hemoperitonium AAAs

37
Imaging studies cont’d CT scanning is now the test of choice for: Intraabdominal infections such as diverticulitis, appendicitis, and post operative infections Vasculature of the abdomen Kidney stones Abdominal hernias Defining obstructions, neoplasms

38
Special Considerations Patients bearing special consideration Women of childbearing age Elderly patients Children Patients on immunosuppressives

39
Women of childbearing age Childbearing women – atypical presentations – pregnant women with appendicitis may present with RUQ pain when uterus displaced other organs in 2 nd /3 rd trimesters

40
Elderly patients A low threshold should be used for admitting or admitting elderly patients. Their presentation is rarely typical. Their history is rarely clear. Their comorbidities are many.

41
Children Young children often have difficulty localizing their pain. History is limited. Obtaining imaging is sometimes difficult but imaging has cut down on improper diagnoses.

42
Immunosuppressives Anyone on prednisone or other immunosuppressive medications be more careful with as they often present atypically. Corticosteroids may mask pain.

43
Aside About Radiation We now image a lot in abdominal pain or chest pain. Try to keep in mind the large amount of radiation that we are exposing people to when we are making our diagnostic plan.

44
Time course of ailment Even if you image someone and the results are normal remember to tell people to still watch for warnings.

45
Abdominal Catastrophes Things not to miss MI AAA Mesenteric ischemia Ectopic pregnancy Ruptured viscous

46
MI Consider in patients with risk factors In patients with epigastric pain In patients who are vomiting, particularly inferior wall MIs Diaphoresis is often common diabetics

47
AAA Used to be misdiagnosed commonly as nephrolithiasis. Consider in any patient with CAD, hypertension, testicular pain, flank pain. Check for pulsatile mass, abdominal bruits.

48
Mesenteric Ischemia Pain out of proportion to exam is the classical description. High morbidity/mortality Consider in older patients with comorbidities such as A. Fib., severe CAD, CHF Angiography is test of choice but can be hard to set up in a timely manner so early consultation is essential.

49
Ectopic pregnancy Perform a pregnancy test in any woman of child bearing age. If positive get a BQuant. Depending on the number and your clinical suspicion obtain a pelvic sonogram.

50
Extraabdominal causes Cardiopulmonary – MI, angina, ptx, pna Abdominal wall – cellulitis, shingles Hernias Metabolic – DKA, AKA or adrenal crisis, sickle cell crisis

51
Questions???

Similar presentations









 Calcium phosphate stones (2) Magnesium ammonium phosphate stones (3)Calcium oxalate stones >")



 The McGraw-Hill Companies, Inc. Permission required for reproduction or display. 23-1 Chapter 23 Abdominal and Gastrointestinal Disorders.>")





