Download presentation
Presentation is loading. Please wait.

1
Syncope Victoria E Judd

2
Disclosure Slide Nothing to disclose

5
Syncope Is the abrupt and transient loss of consciousness
associated with absence of postural tone followed by complete and usually rapid spontaneous recovery

6
Syncope alarming for the individual, witnesses, family, and providers
most often benign and self-limited a harbinger of a multitude of disease processes injuries resulting from syncopal attacks occur in about one-third of patients recurrent episodes can be psychologically devastating can be a premonitory sign of cardiac arrest, especially in patients with organic heart disease

7
Syncope The most frequent age for first syncope is 15 years.
The lifetime incidence of ≥ 1 fainting episodes is ∼40%.

8
Vasovagal Syncope Mediated by emotional distress: fear, pain, instrumentation, blood phobia Mediated by orthostatic stress

9
Situational Syncope Cough, sneeze
Gastrointestinal stimulation (swallow, defecation, visceral pain) Micturition (postmicturation) Post-exercise Postprandial Others (e.g., laughter, brass instrument playing, weightlifting) Carotid sinus syncope
 Micturition (postmicturation) Post-exercise. Postprandial. Others (e.g., laughter, brass instrument playing, weightlifting) Carotid sinus syncope.")
10
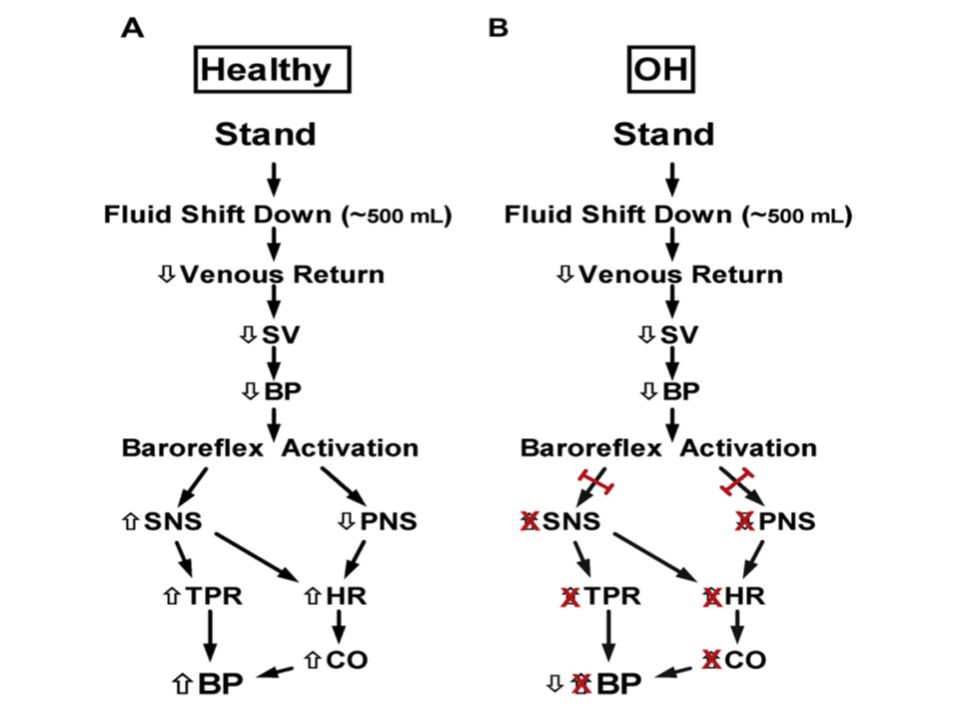
Syncope Due to Orthostatic Hypotension
Primary autonomic failure: Pure autonomic failure, multiple system atrophy, Parkinson's disease with autonomic failure, Lewy body dementia Secondary autonomic failure: Diabetes, amyloidosis, uremia, spinal cord injuries Drug-induced orthostatic hypotension: Alcohol, vasodilators, diuretics, phenothiazine's, antidepressants Volume depletion: Hemorrhage, diarrhea, vomiting, etc.

11
Cardiac Syncope Arrhythmia as primary cause: Bradycardia:
Sinus node dysfunction (including bradycardia/tachycardia syndrome) Atrioventricular conduction system disease Implanted device malfunction Tachycardia: Supraventricular Ventricular (idiopathic, secondary to structural heart disease or to channelopathies) Drug-induced bradycardia and tachyarrhythmias
 Atrioventricular conduction system disease. Implanted device malfunction. Tachycardia: Supraventricular. Ventricular (idiopathic, secondary to structural heart disease or to channelopathies) Drug-induced bradycardia and tachyarrhythmias.")
12
Cardiac Syncope Structural disease:
Cardiac: cardiac valvular disease, acute myocardial infarction/ischemia, hypertrophic cardiomyopathy, cardiac masses (atrial myxoma, tumors, etc.), pericardial disease/tamponade, congenital anomalies of coronary arteries, prosthetic valves dysfunction Others: pulmonary embolus, acute aortic dissection, pulmonary hypertension
, pericardial disease/tamponade, congenital anomalies of coronary arteries, prosthetic valves dysfunction. Others: pulmonary embolus, acute aortic dissection, pulmonary hypertension.")
13
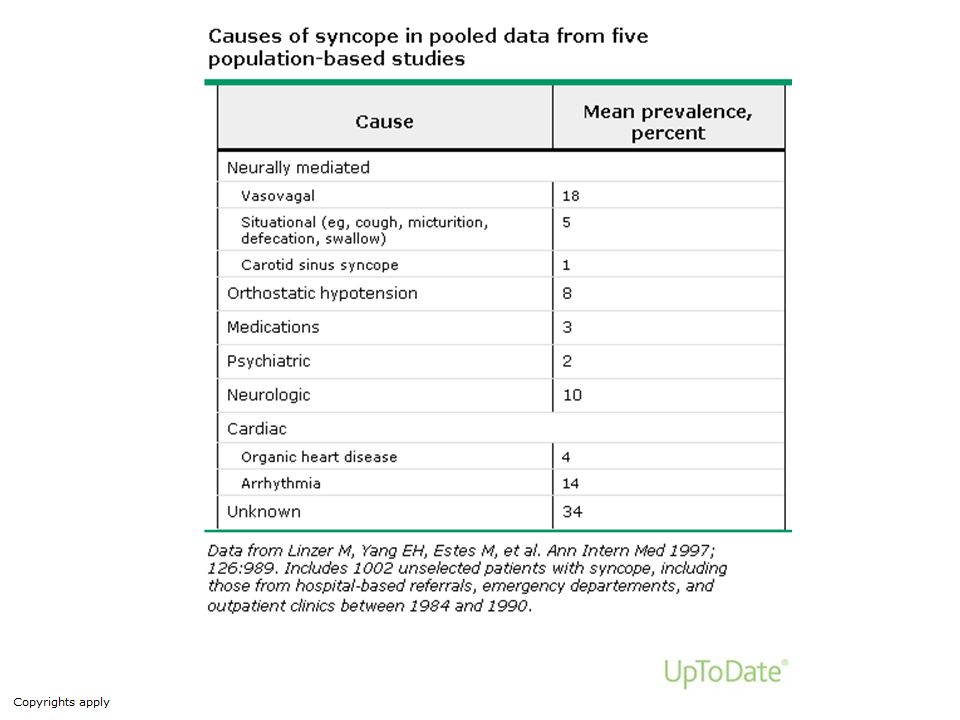
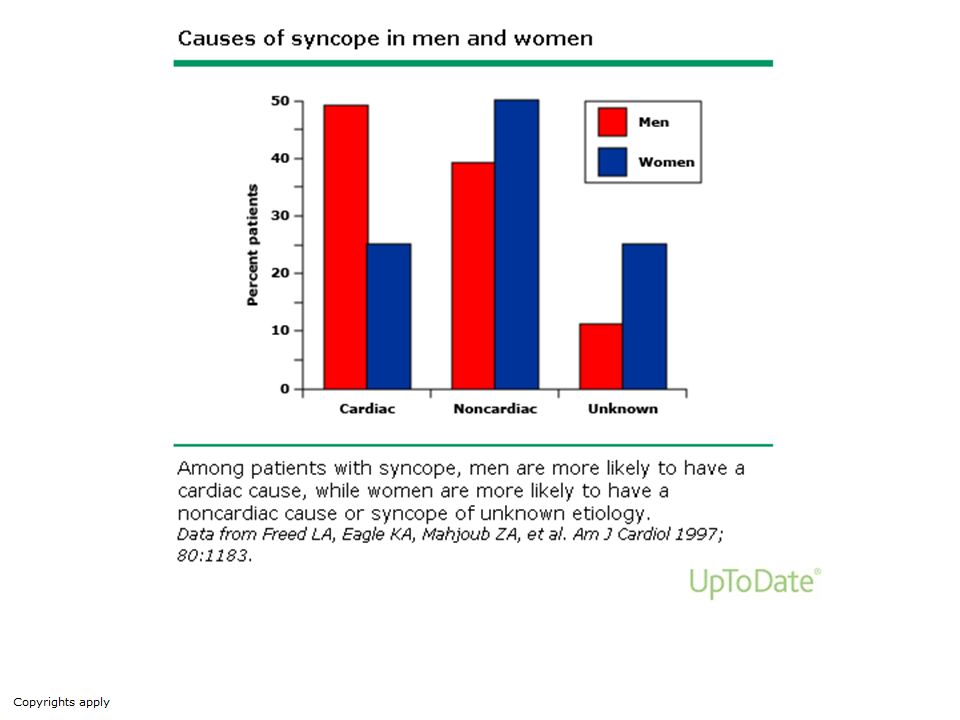
Causes of Syncope ■Reflex (neurally-mediated; this includes vasovagal, POTS) — 58 percent ■Cardiac disease, most often a bradyarrhythmia or tachyarrhythmia — 23 percent ■Neurologic or psychiatric disease — 1 percent ■Unexplained syncope — 18 percent; a higher value (41 percent) was noted in another large series
 — 58 percent ■Cardiac disease, most often a bradyarrhythmia or tachyarrhythmia — 23 percent ■Neurologic or psychiatric disease — 1 percent ■Unexplained syncope — 18 percent; a higher value (41 percent) was noted in another large series")
20
The underlying etiology for syncope can often be identified from the initial evaluation [1,4-7]. Information obtained from the initial evaluation can appropriately guide further analysis if the cause remains unknown [1,8]. Algorithms to diagnose the cause of syncope have been developed [1], but no protocol identifies a cause in all patients with syncope
![The underlying etiology for syncope can often be identified from the initial evaluation [1,4-7].](http://slideplayer.com/slide/6172688/18/images/20/The+underlying+etiology+for+syncope+can+often+be+identified+from+the+initial+evaluation+%5B1%2C4-7%5D..jpg "Information obtained from the initial evaluation can appropriately guide further analysis if the cause remains unknown [1,8]. Algorithms to diagnose the cause of syncope have been developed [1], but no protocol identifies a cause in all patients with syncope.")
21
The initial evaluation should answer three key questions
■Is it a syncopal episode or other type of event? ■Has the etiology been determined? ■Is there evidence suggestive of a high risk of cardiovascular events or death?

24
If Yes, Then Syncope ■Was loss of consciousness complete?
■Was loss of consciousness transient with rapid onset and short duration? ■Did the patient recover spontaneously, completely and without sequela? ■Did the patient lose postural tone?

25
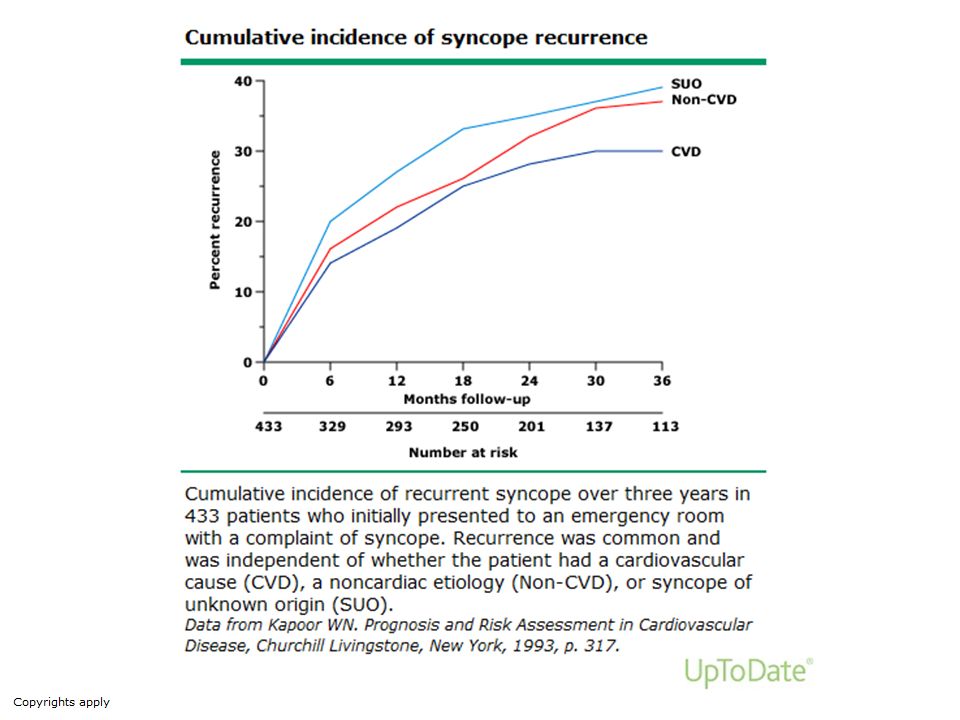
Recurrent Syncope The number of syncopal episodes can predict the risk of recurrence. This was illustrated in a series of 80 patients in which 90 percent of those with a single episode of syncope remained free of recurrence at 23 months without medical therapy and irrespective of the results of a tilt table test. In contrast, 54 percent of patients with two or more syncopal episodes suffered a recurrent episode.

27
Clinical features that suggest a diagnosis on initial evaluation
Neurally mediated syncope: Absence of heart disease Long history of recurrent syncope After sudden unexpected unpleasant sight, sound, smell or pain Prolonged standing or crowded, hot places Nausea, vomiting associated with syncope During a meal or post-prandial With head rotation or pressure on carotid sinus (as in tumors, shaving, tight collars) After exertion
 After exertion.")
28
Clinical features that suggest a diagnosis on initial evaluation
Syncope due to Orthostatic Hypotension(OH): After standing up Temporal relationship with start or changes of dosage of vasodepressive drugs leading to hypotension Prolonged standing especially in crowded, hot places Presence of autonomic neuropathy or Parkinsonism Standing after exertion
: After standing up. Temporal relationship with start or changes of dosage of vasodepressive drugs leading to hypotension. Prolonged standing especially in crowded, hot places. Presence of autonomic neuropathy or Parkinsonism. Standing after exertion.")
29
Clinical features that suggest a diagnosis on initial evaluation
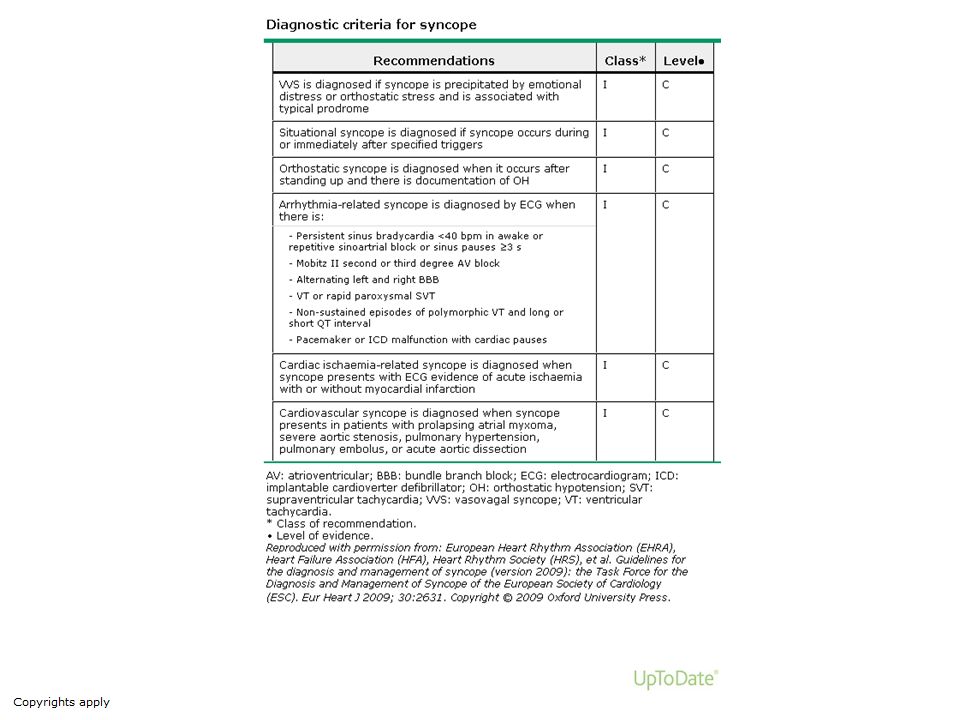
Cardiovascular syncope: Presence of definite structural heart disease Family history of unexplained sudden death or channelopathy During exertion, or supine Abnormal ECG Sudden onset palpitation immediately followed by syncope

30
Cardiovascular syncope:
ECG findings suggesting arrhythmic syncope: - Bifascicular block (defined as either LBBB or RBBB combined with left anterior or left posterior fascicular block) - Other intraventriclar conduction abnormalities (QRS duration ≥0.12 s) - Mobitz I second degree AV block - Asymptomatic inappropriate sinus bradycardia (<50 bpm), sinoatrial block or sinus pause ≥3 s in the absence of negatively chronotropic medications
 - Other intraventriclar conduction abnormalities (QRS duration ≥0.12 s) - Mobitz I second degree AV block. - Asymptomatic inappropriate sinus bradycardia (<50 bpm), sinoatrial block or sinus pause ≥3 s in the absence of negatively chronotropic medications.")
31
Cardiovascular syncope:
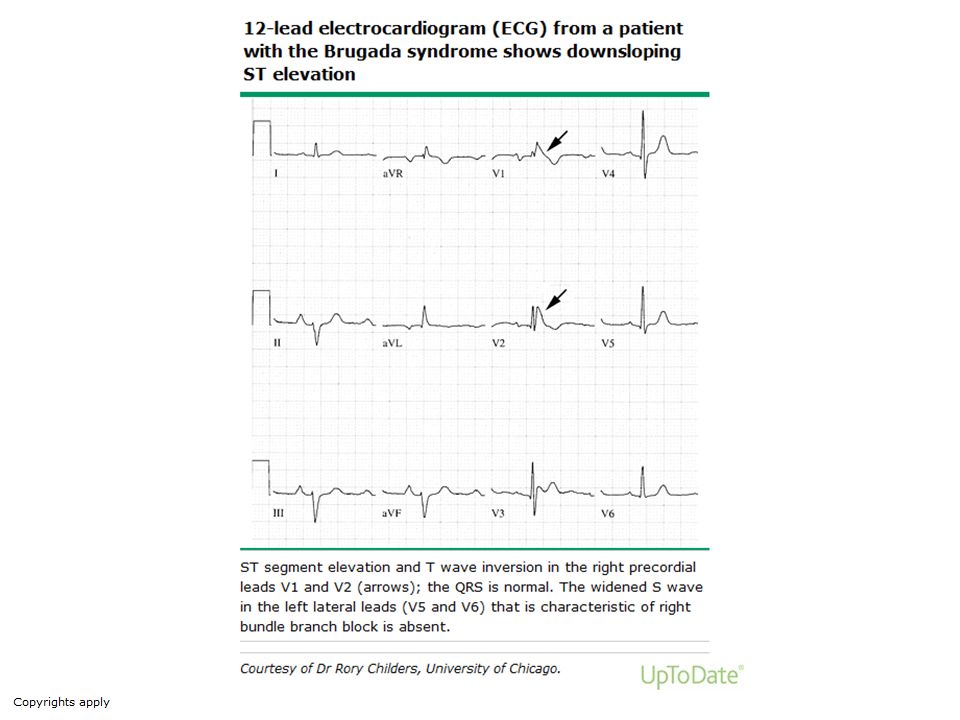
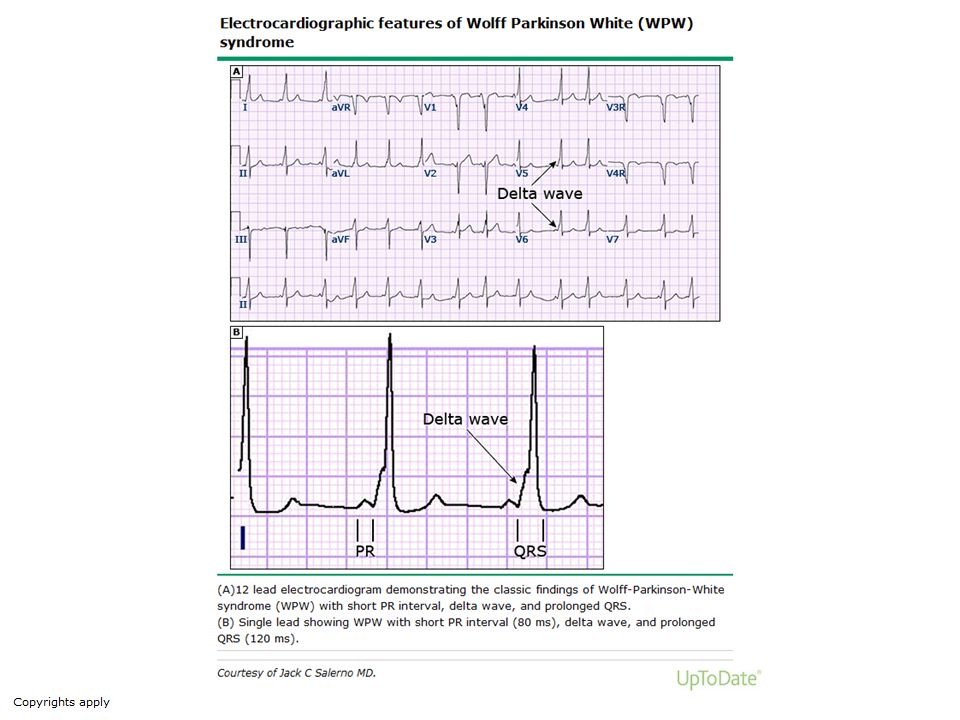
- Non-sustained VT - Pre-excited QRS complexes - Long or short QT intervals - Early repolarization - RBBB pattern with ST-elevation in leads V1-V3 (Brugada syndrome) - Negative T waves in right precordial leads, epsilon waves and ventricular late potentials suggestive of ARVC - Q waves suggesting myocardial infarction
 - Negative T waves in right precordial leads, epsilon waves and ventricular late potentials suggestive of ARVC. - Q waves suggesting myocardial infarction.")
34
Figure 2. Different patterns of QT prolongation in LQTS
Figure 2. Different patterns of QT prolongation in LQTS. Morphology of the QT segment and T wave may be different in different genetic subsets of the LQTS, although there is significant individual variation. Figure 2. Different patterns of QT prolongation in LQTS. Morphology of the QT segment and T wave may be different in different genetic subsets of the LQTS, although there is significant individual variation. Reproduced with permission from Moss et al.64 Strickberger S et al. Circulation 2006;113: Copyright © American Heart Association, Inc. All rights reserved.

35
Figure 3. ECG changes in the Brugada syndrome.
Figure 3. ECG changes in the Brugada syndrome. ST elevation occurs in the anterior precordial leads, leads V1 and V2. Type 1 (coved) ECGs with ≥1 mV of ST elevation have the most prognostic significance. ECG recordings may change over time, as in this example, and serial ECGs may be important. Reproduced with permission from Wilde et al.65 Strickberger S et al. Circulation 2006;113: Copyright © American Heart Association, Inc. All rights reserved.
 ECGs with ≥1 mV of ST elevation have the most prognostic significance. ECG recordings may change over time, as in this example, and serial ECGs may be important. Reproduced with permission from Wilde et al.65. Strickberger S et al. Circulation 2006;113: Copyright © American Heart Association, Inc. All rights reserved.")
38
History "Auras" are associated with seizures. In comparison, vasovagal (neurocardiogenic/reflex) syncope is usually, but not always, associated with a prodrome of nausea, warmth, pallor, lightheadedness, and/or diaphoresis. Sudden onset of syncope without a prodrome is more common among patients with cardiac syncope (arrhythmic or mechanical cardiac etiology).
 syncope is usually, but not always, associated with a prodrome of nausea, warmth, pallor, lightheadedness, and/or diaphoresis. Sudden onset of syncope without a prodrome is more common among patients with cardiac syncope (arrhythmic or mechanical cardiac etiology).")
39
History Neurocardiogenic syncope commonly occurs when the patient is erect, not usually when supine. Syncope resulting from orthostatic hypotension is frequently associated with the change from a supine to erect posture. In comparison, syncope that occurs when the patient is supine suggests an arrhythmia.

40
History An evaluation to rule out potentially life-threatening causes for syncope is required if syncope occurs during exertion

41
History A prolonged loss of consciousness may indicate a seizure. By comparison, arrhythmias and neurocardiogenic syncope are often associated with a brief period of syncope, since the supine position reestablishes some blood flow to the brain and can therefore result in the restoration of consciousness. Recovery of consciousness may occur even if the arrhythmia is maintained.

42
History Persistence of nausea, pallor, and diaphoresis in addition to a prolonged recovery from the episode suggest a vagal event. These findings are helpful in distinguishing neurocardiogenic syncope from syncope due to an arrhythmia. Significant neurologic changes or confusion during the recovery period may be due to a stroke or seizure.

43
History A witness to the syncopal event may verify the loss of consciousness, any associated limb movements, and the presence or absence of pallor, diaphoresis, or a pulse. Neurocardiogenic syncope is more likely to occur among young, otherwise healthy patients.

44
History Important elements of the family history include history of sudden death, pacemakers in young people, syncope, seizures, single car accidents, drowning, cardiomyopathy.

45
History Seizures are the probable cause of 5 to 15 percent of apparent syncopal episodes. They can mimic syncope when the seizure is atypical and not associated with tonic-clonic movements, the seizure is not observed, or a complete history cannot be obtained. In addition, some patients with syncope present with myoclonic or other involuntary movements that are suggestive of a seizure but are actually due to cerebral hypoxia.

46
History One distinguishing feature is that patients with seizures rarely have a rapid and complete recovery. Instead, the postictal state is characterized by a slow and complete recovery. Another feature is usually those with syncope are pale and those with seizures are usually flushed.

47
Physical Exam Blood pressure obtained in the supine, sitting, and erect position may detect orthostatic hypotension.

48
Orthostatic Measurement
Orthostatic blood pressure measurement is performed with the patient standing after at least three minutes of lying supine. Blood pressure should be measured each minute (or more often) in the standing position for three minutes or more (or as long as the patient tolerates) until the blood pressure nadir is reached. A sphygmomanometer (manual blood pressure cuff) may allow greater flexibility than an automatic arm-cuff device in measuring blood pressure prior to and during active standing
 in the standing position for three minutes or more (or as long as the patient tolerates) until the blood pressure nadir is reached. A sphygmomanometer (manual blood pressure cuff) may allow greater flexibility than an automatic arm-cuff device in measuring blood pressure prior to and during active standing.")
49
Orthostatic syndromes
■Classic orthostatic hypotension (OH) is defined as a decrease in systolic blood pressure (BP) of ≥20 mmHg and in diastolic BP ≥10 mmHg within three minutes of standing. This syndrome is diagnosed by active standing or tilt testing. ■Initial OH is defined by a BP decrease immediately on standing of >40 mmHg with BP spontaneously and rapidly returning to normal, so the period of hypotension and symptoms is <30 s. This is diagnosed by active standing.
 is defined as a decrease in systolic blood pressure (BP) of ≥20 mmHg and in diastolic BP ≥10 mmHg within three minutes of standing. This syndrome is diagnosed by active standing or tilt testing. ■Initial OH is defined by a BP decrease immediately on standing of >40 mmHg with BP spontaneously and rapidly returning to normal, so the period of hypotension and symptoms is <30 s. This is diagnosed by active standing.")
50
Orthostatic syndromes
■Reflex syncope (vasovagal syncope) triggered by standing is characterized by an initial normal adaption reflex followed by rapid fall in venous return and vasovagal reaction (reflex bradycardia and vasodilatation). This is diagnosed by tilt table. ■Delayed (progressive) OH is defined by a slow progressive decrease in systolic BP on standing with no bradycardic reflex (in contrast to reflex syncope). This is diagnosed by tilt table.
 triggered by standing is characterized by an initial normal adaption reflex followed by rapid fall in venous return and vasovagal reaction (reflex bradycardia and vasodilatation). This is diagnosed by tilt table. ■Delayed (progressive) OH is defined by a slow progressive decrease in systolic BP on standing with no bradycardic reflex (in contrast to reflex syncope). This is diagnosed by tilt table.")
51
Orthostatic syndromes
■Delayed (progressive) OH plus reflex syncope occurs when a vasovagal reaction (reflex bradycardia and vasodilation) follows delayed OH. This is diagnosed by tilt table.
 OH plus reflex syncope occurs when a vasovagal reaction (reflex bradycardia and vasodilation) follows delayed OH. This is diagnosed by tilt table.")
52
Orthostatic syndromes
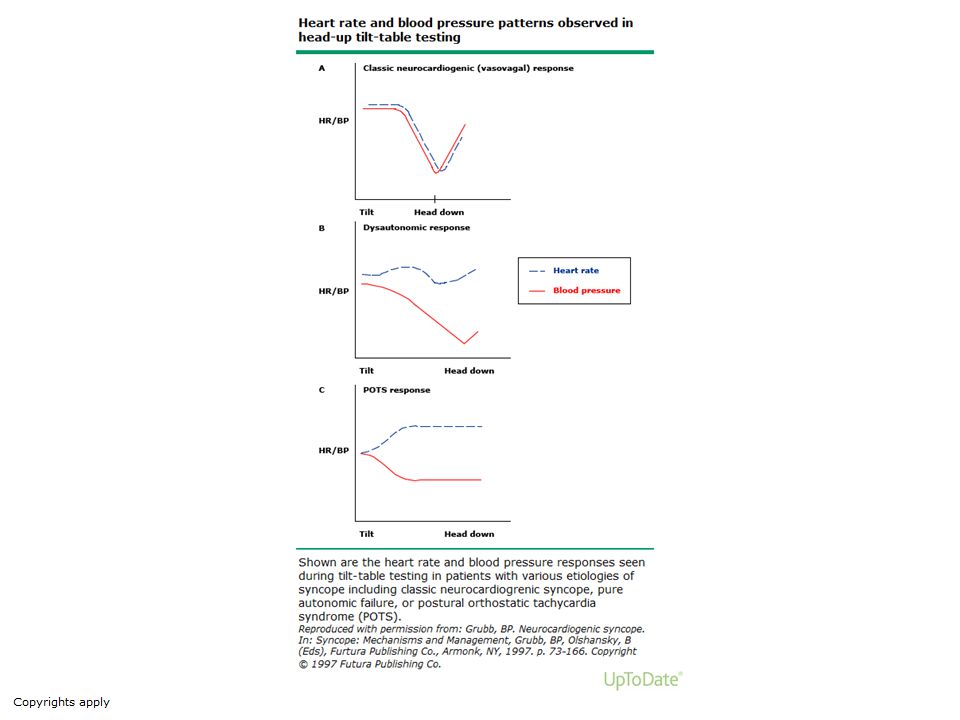
■Postural orthostatic tachycardia syndrome (POTS) presents with severe orthostatic intolerance (not syncope) with marked increase in heart rate (by >30 beats per minute or to >120 beats per minute)within ten minutes of standing. This is diagnosed by tilt table or passive standing. POTS can be diagnosed with bedside measurements of heart rate and blood pressure taken in the supine (laying down) and standing up position at 2, 5 and 10 minute intervals. In children and adolescents, a revised standard of a 40 bpm or more increase has recently been adopted.
 presents with severe orthostatic intolerance (not syncope) with marked increase in heart rate (by >30 beats per minute or to >120 beats per minute)within ten minutes of standing. This is diagnosed by tilt table or passive standing. POTS can be diagnosed with bedside measurements of heart rate and blood pressure taken in the supine (laying down) and standing up position at 2, 5 and 10 minute intervals. In children and adolescents, a revised standard of a 40 bpm or more increase has recently been adopted.")
54
Physical Exam The heart rate may be rapid or slow due to a number of possible rhythm disturbances, or irregular due to atrial fibrillation. The pulse and blood pressure should be obtained with the patient supine, seated, and erect. Hyperventilation can be seen with pulmonary embolism or psychiatric causes of syncope.

55
Physical Exam The cardiac examination may reveal the murmur of aortic stenosis, pulmonic stenosis, or atrial myxoma (mitral stenosis). Pulmonary hypertension may be suggested by a loud, palpable P2. Increase in an outflow murmur with the Valsalva maneuver may help diagnose hypertrophic cardiomyopathy.

56
Physical Exam Unilateral abnormalities found upon neurologic examination may reflect a cerebral vascular accident.

57
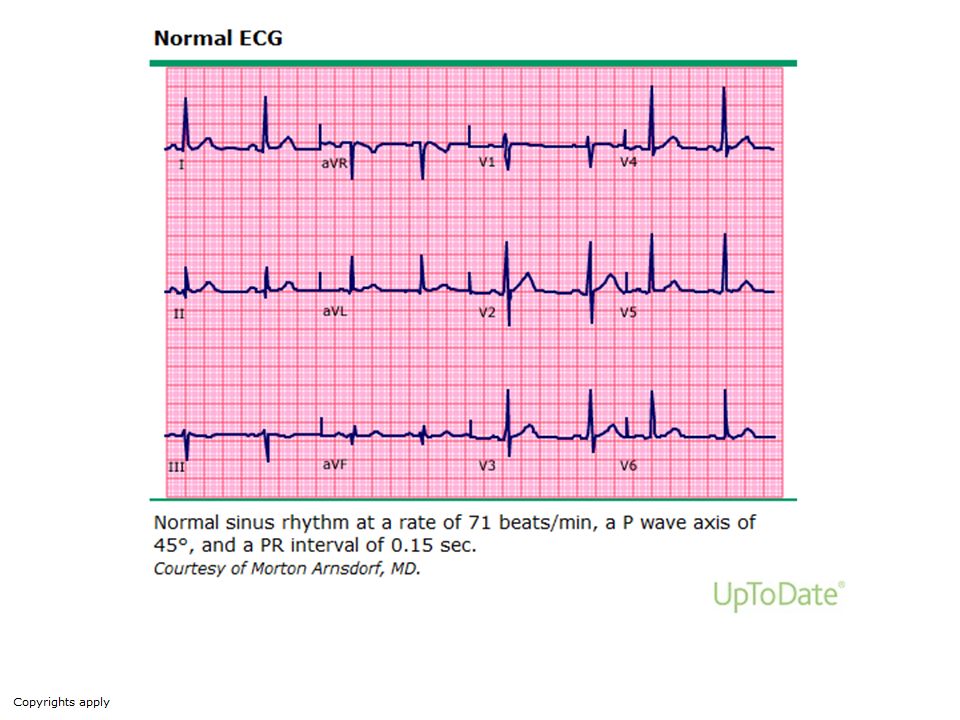
ECG An electrocardiogram (ECG) should be obtained in all patients with syncope. The ECG is suggestive of an arrhythmic cause of syncope if any of the following abnormalities is present: ■Bifascicular block (defined as left bundle branch block or right bundle branch block combined with left anterior or left posterior fascicular block) ■Other intraventricular conduction abnormalities (QRS duration ≥0.12 sec) ■Mobitz II second degree atrioventricular block
 should be obtained in all patients with syncope. The ECG is suggestive of an arrhythmic cause of syncope if any of the following abnormalities is present: ■Bifascicular block (defined as left bundle branch block or right bundle branch block combined with left anterior or left posterior fascicular block) ■Other intraventricular conduction abnormalities (QRS duration ≥0.12 sec) ■Mobitz II second degree atrioventricular block.")
58
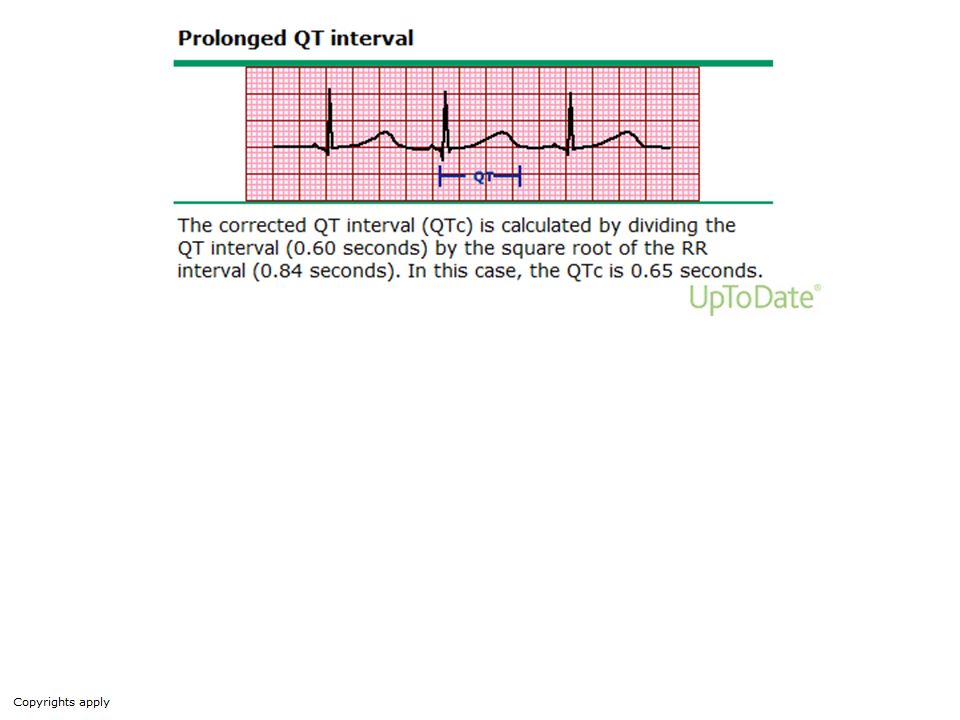
ECG ■Asymptomatic sinus bradycardia (<50 beats/min), sinoatrial block or sinus pause ≥3 seconds in the absence of negatively chronotropic medications ■Preexcited QRS complexes, suggesting Wolff-Parkinson-White syndrome ■Long or short QT intervals ■Right bundle branch block pattern with ST-elevation in leads V1-V3 (Brugada syndrome) ■Negative T waves in right precordial leads, epsilon waves and ventricular late potentials suggestive of arrhythmogenic right ventricular cardiomyopathy ■Q waves suggesting myocardial infarction
 ■Negative T waves in right precordial leads, epsilon waves and ventricular late potentials suggestive of arrhythmogenic right ventricular cardiomyopathy. ■Q waves suggesting myocardial infarction.")
59
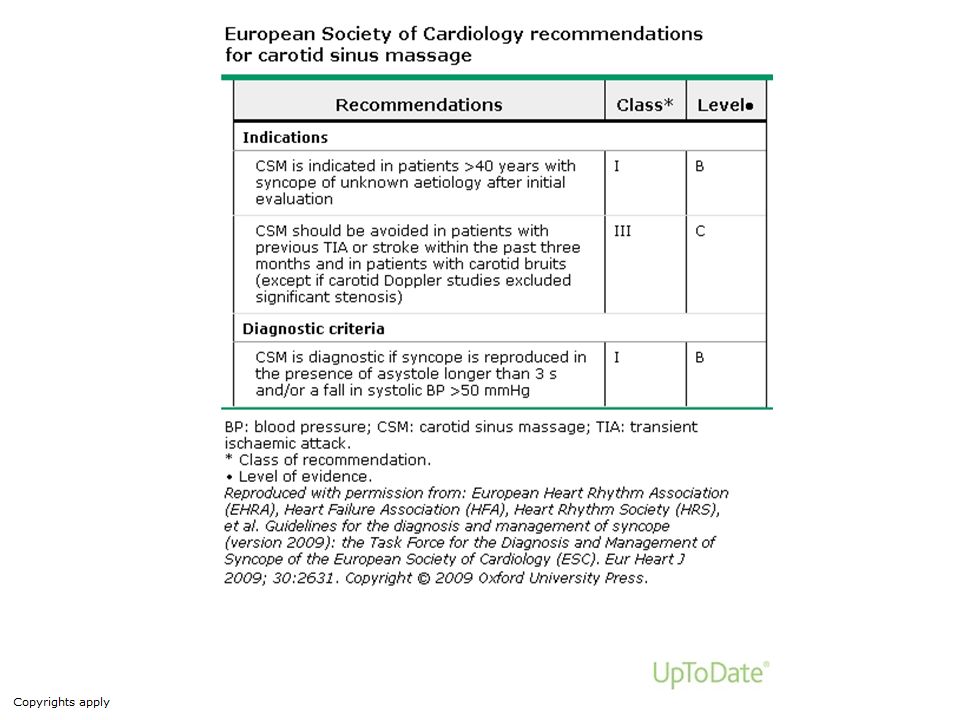
Testing Additional testing is based on the results of the initial evaluation. A variety of tests, mostly cardiologic, can be used in the evaluation of the patient with syncope. Neurologic testing is generally of low yield and overused, unless specifically suggested by history or physical examination. ■Carotid sinus massage in patients >40 years old. ■Echocardiogram when there is previous known heart disease or data suggestive of structural heart disease or syncope secondary to cardiovascular cause.

60
Testing Immediate ECG monitoring when there is a suspicion of arrhythmic syncope. ■Orthostatic challenge (lying to standing orthostatic test or head-up tilt testing) when syncope is related to the standing position or there is suspicion of a reflex mechanism ■Other less specific tests such as neurological evaluation or blood tests are indicated only when there is suspicion of non-syncopal transient loss of consciousness.
 when syncope is related to the standing position or there is suspicion of a reflex mechanism. ■Other less specific tests such as neurological evaluation or blood tests are indicated only when there is suspicion of non-syncopal transient loss of consciousness.")
64
Testing Echocardiography is recommended in patients with syncope when structural cardiac disease is suspected. Electrocardiographic (ECG) monitoring is indicated if there is a high probability of identifying an arrhythmia associated with syncope. Electrophysiology study (EPS) is indicated in selected patients with unexplained syncope.
 monitoring is indicated if there is a high probability of identifying an arrhythmia associated with syncope. Electrophysiology study (EPS) is indicated in selected patients with unexplained syncope.")
65
Implantable Loop Recorders (ILR)
Automatically detects bradycardia tachycardia asystole ILR Records rhythm at time of trigger Patient Assist Device Syncopal events are often too infrequent and unpredictable for detection by conventional ambulatroy monitoring. Therefore, we use an implantable loop recorder or monitor. This is a wireless device that is implanted under the skin similar to pacemaker. Continuous loop monitoring for about 3 years. Events may be automatically triggered or patient triggered.

66
ILRs Leads to more implants of PPM and ICDs

67
Example tracing from ILR

68
ILR in unexplained syncope with normal conventional work-up
Tachycardia Asystole / bradycardia 11% No arrhythmia 33% 56% Pool data from 9 studies to a total of 506 patients. Correlation between syncope and underlying rhythm was found in 35% of patients for a diagnostic yield of 35%. Of these 56% had asystole of bradycardia 11% had tachycardia and 33% had no-arrhythmia. Diagnostic yield was hampered in 5-9% of patients due to failure of syncope relapse. Diagnostic yield: 35% (175/506 patients) Brignole et al. Europace 2009;11,
 Brignole et al. Europace 2009;11,")
69
Testing Neurologic tests, including electroencephalogram (EEG), brain CT scan, brain magnetic resonance imaging, and carotid Doppler ultrasound, are frequently obtained in patients with syncope. In one review of 649 patients, 53 percent had at least one neurologic test. However, such testing was rarely useful.
, brain CT scan, brain magnetic resonance imaging, and carotid Doppler ultrasound, are frequently obtained in patients with syncope. In one review of 649 patients, 53 percent had at least one neurologic test. However, such testing was rarely useful.")
71
Postural Orthostatic Tachycardia Syndrome (POTS)
A form of orthostatic intolerance occurs in patients, particularly younger adults and children, who consistently or frequently experience symptoms of orthostatic intolerance in response to postural stressors. Autonomic reflexes are relatively preserved in these patients, and orthostatic hypotension and syncope rarely occur. Some patients may have slightly elevated blood pressure. The hallmark of this disorder is an exaggerated heart rate increase in response to postural change.

72
Names of POTS ■Chronic orthostatic intolerance
■Mild orthostatic intolerance ■Orthostatic tachycardia ■Sympathotonic orthostatic hypotension ■Hyperdynamic beta adrenergic state ■Idiopathic hypovolemia ■Mitral valve prolapse syndrome ■Neurocirculatory asthenia ■Irritable heart ■Soldier's heart ■Effort syndrome

73
Facts POTS It is the most prevalent form of orthostatic intolerance. It is estimated that 500,000 Americans suffer from this disorder. It is the most common syndrome of young people seen in autonomic dysfunction clinics. Patients present at a relatively young age (14 to 45 years).
.")
74
Facts POTS Women predominate among patients with POTS with a female to male ratio of 4-5:1. The reason for this is not known, however, observed gender differences in muscle sympathetic nerve discharge characteristics in healthy patients may explain why women are more likely to develop POTS.

75
Etiology POTS The etiology of postural tachycardia syndrome (POTS) is heterogeneous. Investigators have reported a number of different abnormalities in patients with POTS. It remains uncertain as to which of these abnormalities are primary and causative and which are secondary.
 is heterogeneous. Investigators have reported a number of different abnormalities in patients with POTS. It remains uncertain as to which of these abnormalities are primary and causative and which are secondary.")
76
Etiology POTS Distal denervation — Several clinical and empiric observations suggest the presence of distal, predominantly lower extremity, denervation with preserved cardiac innervation in this disorder.

77
Etiology POTS Hypovolemia — Patients with POTS frequently experience symptomatic improvement with saline infusion. Additional evidence of a decrease and/or redistribution of blood volume is observed in several studies of patients with POTS, which have noted: ■Hypovolemia ■Trend toward hypovolemia ■Reduced erythrocyte volume ■Excessive venous pooling with redistributive hypovolemia

78
Etiology POTS Changes in venous function — Abnormal venous function with decreased venous return on assumption of the upright posture could stimulate a compensatory tachycardia in order to maintain cardiac output. Baroreflex abnormalities — The increase in heart rate without blood pressure change upon standing in POTS suggests a primary abnormality in baroreflex control.

79
Etiology POTS Increased sympathetic activity — Increased sympathetic activity is the final common pathway of most proposed mechanisms in POTS. Genetic abnormalities — In one large series, 12.5 percent of 152 patients with POTS reported a family history of orthostatic intolerance

80
Clinical POTS Patients with postural tachycardia syndrome (POTS) report dizziness, lightheadedness, weakness, blurred vision, and fatigue upon standing. Other predominantly orthostatic symptoms include palpitations, tremulousness, and anxiety.
 report dizziness, lightheadedness, weakness, blurred vision, and fatigue upon standing. Other predominantly orthostatic symptoms include palpitations, tremulousness, and anxiety.")
81
Clinical POTS Gastrointestinal symptoms such as nausea, abdominal cramps, early satiety, bloating, constipation, and diarrhea may be particularly problematic in some. There may also be evidence of venous pooling, as manifested by acrocyanosis and edema when upright. Syncope is relatively unusual, but does occur in about 40 percent of patients.

83
Clinical POTS The onset often follows a flulike illness.
Illness may occasionally represent a self-limited autoimmune disease. The role of immune and epigenetic factors remains ill defined. Some patients have an insidious onset over years, sometimes with a past history of VVS.

84
Clinical POTS ? Some patients have joint hypermobility syndromes.
Causality is unclear. While supine or seated, some patients appear well, others pasty pale.

85
Clinical POTS Patients are unable to remain upright for long periods of time. Symptoms are similar to the prodrome of VVS. BP is typically well maintained and may increase when upright in hyperadrenergic individuals. Prolonged laboratory tilt may provoke VVS.

86
Clinical POTS Cognitive deficits and exercise intolerance are prominent complaints. Gastrointestinal symptoms include dysmotility issues. Young women may be underweight, and POTS must be differentiated from eating disorders, which can produce POTS-like Orthostatic Intolerance in early stages.

87
Clinical POTS Environmental heat reroutes blood to the skin and makes patients worse. Air-conditioning may be required and standing hot showers untenable. Schoolwork may be impaired. Home schooling is common in adolescents. Colleges are often accommodating because of adaptive scheduling and improved logistics.

88
Clinical POTS The symptoms may appear abruptly, often after a viral illness; others experience a more insidious onset. The severity of symptoms is also quite variable. Some patients experience only mild symptoms and often only in the setting of additional orthostatic stress (e.g., menstrual cycle, relative dehydration). Others are profoundly incapacitated. The course of the disorder may be self limited or may follow a relapsing remitting course over several years.
. Others are profoundly incapacitated. The course of the disorder may be self limited or may follow a relapsing remitting course over several years.")
89
Diagnosis POTS The characteristic autonomic abnormality in patients with postural tachycardia syndrome (POTS) is an exaggerated increase in heart rate on tilt table testing or standing. Diagnostic criteria from several laboratories have in common a sustained heart rate increase of greater than 30 beats per minute or an increase to 120 beats per minute or greater within the first 10 minutes of tilt. There is usually no orthostatic hypotension.
 is an exaggerated increase in heart rate on tilt table testing or standing. Diagnostic criteria from several laboratories have in common a sustained heart rate increase of greater than 30 beats per minute or an increase to 120 beats per minute or greater within the first 10 minutes of tilt. There is usually no orthostatic hypotension.")
90
Diagnosis POTS Autonomic neuropathies, central dysautonomias, bedrest deconditioning, side effects of medications, and dehydration can produce similar symptoms to POTS. Ruling out these conditions is essential to making a diagnosis of POTS. In most cases, historical information and a neurologic examination specifically looking for other evidence of autonomic failure, neuropathy, and extrapyramidal signs, will provide evidence of the underlying disorder.

91
Diagnosis POTS Patients with POTS may be thought to have panic, anxiety, somatization disorder, or chronic fatigue syndrome in part because of the vague nature of the symptoms. In fact, patients with POTS report subjective cognitive dysfunction and have objectively increased scores on inattention scales, but do not have an increased prevalence of depression or anxiety. The prominent postural nature of the symptoms should prompt the clinician to look for the diagnostic heart rate response.

92
Diagnosis POTS The syndrome of inappropriate sinus tachycardia is characterized by an elevated heart rate that is not influenced by postural changes.

93
Treatment POTS The optimal therapy of postural tachycardia syndrome (POTS) is uncertain. No intervention has been systematically studied. The placebo effect may be substantial in POTS, highlighting the need for controlled studies. Exacerbating factors, medications, dehydration, and inactivity should be avoided.

94
Treatment POTS Because many patients with POTS have a low plasma volume, correction with oral volume expansion, a high salt diet (3,000 mg to 10,000 mg per day), and fludrocortisone, a mineralocorticoid agonist may improve symptoms. This regimen is similar to that used in orthostatic hypotension in general.
, and fludrocortisone, a mineralocorticoid agonist may improve symptoms. This regimen is similar to that used in orthostatic hypotension in general.")
95
Treatment POTS Some patients report symptomatic benefit with acute ingestion of 16 oz of water and from a saline infusion of 500 to 2000 cc, corresponding to objective improvement in tilt testing response. However, it is not clear that this translates to a therapeutic response to chronic treatment. Fludrocortisone (0.1 to 0.4 mg per day) is most effective when combined with increased salt and water intake. Treatment may be complicated by supine hypertension, fluid retention, and hypokalemia and should be monitored closely.
 is most effective when combined with increased salt and water intake. Treatment may be complicated by supine hypertension, fluid retention, and hypokalemia and should be monitored closely.")
96
Treatment POTS Adrenoreceptor agonists may be helpful in some patients (e.g., midodrine 2.5 to 10 mg three times daily). Both intravenous phenylephrine and oral midodrine have been associated with improved symptoms and heart rate response in some patients during tilt testing. However, benefit from chronic therapy is not established.

97
Treatment POTS Preliminary evidence suggests that the acetylcholinesterase inhibitor pyridostigmine (30 mg daily) may attenuate the tachycardia and improve symptoms. Further confirmation from larger trials is needed to establish the benefit of acetylcholinesterase inhibition for POTS.
 may attenuate the tachycardia and improve symptoms. Further confirmation from larger trials is needed to establish the benefit of acetylcholinesterase inhibition for POTS.")
98
Treatment POTS Some patients, particularly those troubled by prominent adrenergic symptoms, may benefit from beta blocking agents. These should be started in low doses and increased gradually (e.g., propranolol 10 to 20 mg three or four times daily). In one placebo-controlled, randomized crossover study, a single low-dose of oral propranolol (20 mg) was associated with improved tachycardia and reduced symptoms, while higher dose propranolol (80 mg) was associated with unchanged or worsened symptoms.
. In one placebo-controlled, randomized crossover study, a single low-dose of oral propranolol (20 mg) was associated with improved tachycardia and reduced symptoms, while higher dose propranolol (80 mg) was associated with unchanged or worsened symptoms.")
99
POTS Treatment Water ingestion is a useful, short lived palliation.
Effects are through TRPV4 receptors in the splanchnic vasculature. Sixteen ounces of water and waiting 20 to 30 minutes yields benefit for hours. Salt and water loading can help but often require Spartan efforts.

100
POTS Treatment Even when the cause is known pharmacologic treatment is rarely curative. Most young people improve over time. In some, POTS persists.

101
Volume Expansion Fludrocortisone mg daily – Many patients with POTS are hypovolemic 4, so fludrocortisone (an aldosterone analogue) is often used. Through enhanced renal sodium retention, it should expand the plasma volume (although the data are poor). Potassium wasting can result in hypokalemia, so serum K+ should be monitored periodically.
 is often used. Through enhanced renal sodium retention, it should expand the plasma volume (although the data are poor). Potassium wasting can result in hypokalemia, so serum K+ should be monitored periodically.")
102
Sympatholysis Propranolol mg PO QID – Many patients report intolerance to beta blockers when first seen at the Vanderbilt Autonomic Dysfunction Center. The vast majority of POTS patients, however, respond well hemodynamically and symptomatically to low doses of propranolol. Of note, more complete beta blockade with higher doses of propranolol cause symptoms to worsen. Long acting propranolol was not found to be helpful.

103
Sympatholysis Methyldopa 125mg QHS-BID – Methyldopa is a false neurotransmitter that can lower central sympathetic tone. It is particularly useful in hyperadrenergic patients. Clonidine mg PO BID (or a long acting patch) - Alpha 2 adrenergic agonist that acts centrally to decrease sympathetic nervous system tone. It can stabilize HR and BP, but it can also cause drowsiness, fatigue and worsen the mental clouding of some patients.
 - Alpha 2 adrenergic agonist that acts centrally to decrease sympathetic nervous system tone. It can stabilize HR and BP, but it can also cause drowsiness, fatigue and worsen the mental clouding of some patients.")
104
Vasoconstrictor Therapy
Midodrine 5-10mg PO q4H x3/day - Since a failure of vascular resistance may be an integral part of neuropathic POTS, vasoconstrictors such as midodrine (alpha-1 agonist) can be employed.
 can be employed.")
105
Increasing Vagal Tone Pyridostigmine mg PO TID – Pyridostigmine is a peripheral acetylcholinesterase inhibitor. By increasing synaptic acetylcholine at both the autonomic ganglia and the peripheral muscarinic parasympathetic receptors, pyridostigmine significantly restrains the heart rate in response to standing in patients with POTS. Pyridostigmine is most effective in combination with low dose propranolol. Since pyridostigmine enhances bowel motility, it is often not well tolerated in patients with diarrhea-predominant irritable bowel syndrome symptoms.

106
? Treatment of POTS Cardiovasc Ther Feb 4. doi: / [Epub ahead of print] Melatonin reduces tachycardia in Postural Tachycardia Syndrome (POTS): A Randomized, Crossover Trial. Green EA1, Black BK, Biaggioni I, Paranjape SY, Bagai K, Shibao C, Okoye MC, Dupont WD, Robertson D, Raj SR. Autonomic Dysfunction Center, Division of Clinical Pharmacology, Departments of Medicine, Vanderbilt University, Nashville, Tennessee, USA.
![Treatment of POTS Cardiovasc Ther Feb 4. doi: / [Epub ahead of print]](http://slideplayer.com/slide/6172688/18/images/106/Treatment+of+POTS+Cardiovasc+Ther+Feb+4.+doi%3A+%2F+%5BEpub+ahead+of+print%5D.jpg "Melatonin reduces tachycardia in Postural Tachycardia Syndrome (POTS): A Randomized, Crossover Trial. Green EA1, Black BK, Biaggioni I, Paranjape SY, Bagai K, Shibao C, Okoye MC, Dupont WD, Robertson D, Raj SR. Autonomic Dysfunction Center, Division of Clinical Pharmacology, Departments of Medicine, Vanderbilt University, Nashville, Tennessee, USA.")
107
Figure. Treatment strategies for POTS.
Grubb B P , and Karabin B Circulation. 2008;118:e61-e62 Copyright © American Heart Association, Inc. All rights reserved.

108
POTS Treatment One confounding and alarming issue is the tendency for POTS patients to bed rest. Prolonged bed rest emulates microgravity and has deleterious effects including Orthostatic Instability (OI) profound reductions in blood volume and cardiac size, redistribution of blood, osteoporosis, skeletal muscle pump atrophy, and more. Vasoconstriction is impaired. Bed rest causes a self-perpetuating state of OI, which can emulate or intensify POTS.
 profound reductions in blood volume and cardiac size, redistribution of blood, osteoporosis, skeletal muscle pump atrophy, and more. Vasoconstriction is impaired. Bed rest causes a self-perpetuating state of OI, which can emulate or intensify POTS.")
109
POTS Treatment It is paramount for POTS patient to leave bed and recondition. Well-structured exercise protocols are essential and must accommodate patients who start off bed rested. Reconditioning invariably improves patient well-being. Recent work supports the idea that POTS patients are also exercise deconditioned compared with matched volunteers. Although exercise deconditioning may or may not be causal in POTS, it is clear that exercise reconditioning is beneficial and should be advocated for all POTS patients.

110
Diagnostic Criteria for Postural Tachycardia Syndrome
HR increase ≥30 bpm from lying to standing Absence of significant drop in BP with standing Positional symptoms ○ Many symptoms are worse with upright posture and improve on lying down ○ Some symptoms can be non-positional (e.g. fatigue, headache) Chronic symptoms ○ Duration ≥6 months Absence of other overt cause for tachycardia ○ E.g., acute blood loss, prolonged bedrest, hyperthyroidism, tachycardia promoting medications
 Chronic symptoms. ○ Duration ≥6 months. Absence of other overt cause for tachycardia. ○ E.g., acute blood loss, prolonged bedrest, hyperthyroidism, tachycardia promoting medications.")
112
Reflex (Neurally Mediated) Syncope
Reflex (neurally mediated) syncope is a transient loss of consciousness due to a reflex response that encompasses vasodilatation and/or bradycardia (rarely tachycardia), leading to systemic hypotension and cerebral hypoperfusion. Types of reflex syncope include vasovagal syncope, situational syncope, carotid sinus syncope, and atypical forms (without apparent triggers and/or atypical presentation).
 syncope is a transient loss of consciousness due to a reflex response that encompasses vasodilatation and/or bradycardia (rarely tachycardia), leading to systemic hypotension and cerebral hypoperfusion. Types of reflex syncope include vasovagal syncope, situational syncope, carotid sinus syncope, and atypical forms (without apparent triggers and/or atypical presentation).")
113
Reflex Syncope Vasovagal:
Mediated by emotional distress: fear, pain, instrumentation, blood phobia Mediated by orthostatic stress

114
Reflex Syncope Situational: Cough, sneeze
Gastrointestinal stimulation (swallow, defecation, visceral pain) Micturition (postmicturition) Post-exercise Postprandial Others (e.g., laughter, brass instrument playing, weightlifting) Hair grooming Stretching
 Micturition (postmicturition) Post-exercise. Postprandial. Others (e.g., laughter, brass instrument playing, weightlifting) Hair grooming. Stretching.")
115
Reflex Syncope Carotid sinus syncope
Atypical forms (without apparent triggers and/or atypical presentation)
")
116
Reflex Syncope Vasovagal syncope (also known as neurocardiogenic syncope) is the most common cause of syncope. The diagnosis may be suggested or diagnosed by a specific history with well-known triggers, but a classic history is not required. The diagnosis can also be made by exclusion of other causes of syncope and by a characteristic response to upright tilt table testing during which the patient may pass out from bradycardia and/or hypotension.

118
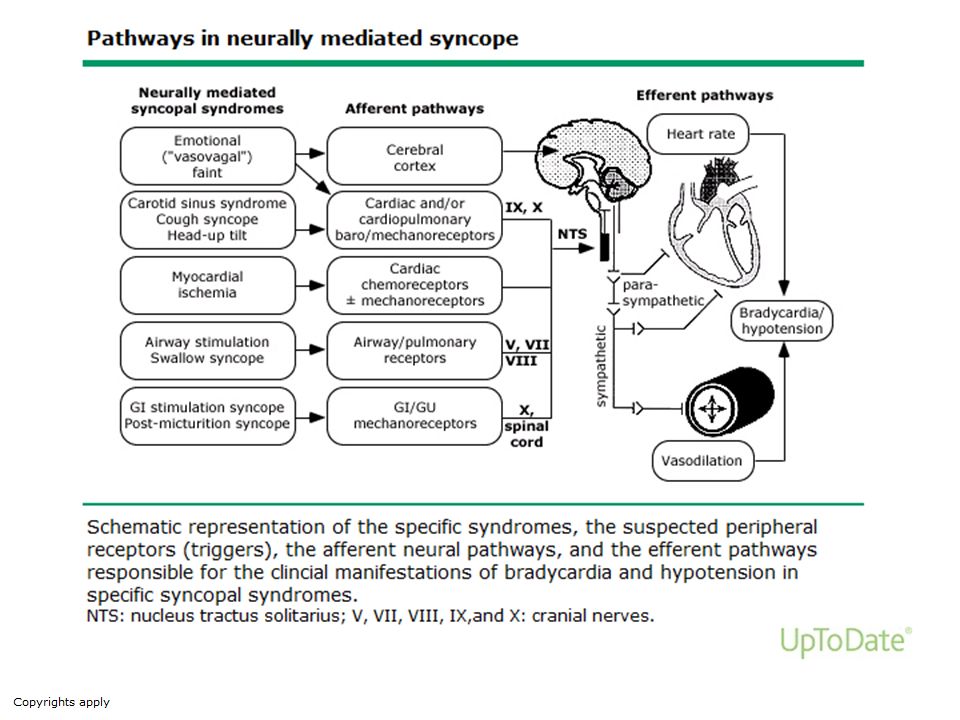
Reflex Mechanism - Bezold Jarisch
Inotropy Contractility Venous return Trigger BP Sympathetic tone Arterial HR Vasodilation BP Syncope Vagal efferent Small ventricle afferent Sympathetic withdrawal Wall stretch Reflex C-fibers The reflex mechanism is fairly well elucidated. A trigger such as prolonged upright posture results decreased venous return and reduced intracardiac volume. The resultant arterial hypotension is sensed in the carotid sinus baroreceptors and efferent fibers from these receptors trigger autonomic signals that increase cardiac rate and contractility by increasing sympathetic tone and decreasing vagal tone. Arterial tension is also increased. The combined effect is a rise in blood pressure. This is a physiologic and normal response. However, in some patients a hypersensitive reflex mechanism mediated by C-fibers results in syncope. Pressure receptors (C-fibers) in the inferoposterior wall of the underfilled left ventricle may then sense increased wall stress leading increase vagal afferent stimuli and consequently a sudden withdrawl of sympathetic tone. This leads to a paradoxical bradycardia, decreased contractility and vaso-dilitation. The result is sudden hypotension and syncope. Chang-Sing P. Cardiol Clinics. 1991;9(4):
 in the inferoposterior wall of the underfilled left ventricle may then sense increased wall stress leading increase vagal afferent stimuli and consequently a sudden withdrawl of sympathetic tone. This leads to a paradoxical bradycardia, decreased contractility and vaso-dilitation. The result is sudden hypotension and syncope. Chang-Sing P. Cardiol Clinics. 1991;9(4):")
119
Reflex Syncope Upright posture causes pooling of blood in lower extremities Decrease in venous return causes transient hyperdynamic ventricle Cardiac C fibers (mechanoreceptors) activate causing parasympathetic response resulting in bradycardia, peripheral vasodilation and hypotension Abrupt decrease in BP and HR ± asystole
 activate causing parasympathetic response resulting in bradycardia, peripheral vasodilation and hypotension. Abrupt decrease in BP and HR ± asystole.")
120
Reflex Syncope Alterations in autonomic activation are responsible for reflex syncope. Three types of responses are seen: a cardioinhibitory response, a vasodepressor response, and a mixed response with features of both.

121
Reflex Syncope An individual patient may have separate syncopal events characterized by a primary vasodepressor, cardioinhibitory or mixed responses, but the episodes can vary in their presentation for any individual such that asystole may occur at one time and hypotension at another. Furthermore, the response observed during tilt table testing is not necessarily the same as that recorded during clinical episodes. Asystolic pauses are more common during spontaneous episodes, but hypotension is more common during tilt table testing.

122
Reflex Syncope Vasovagal (neurocardiogenic) syncope (also known as the “common faint”) refers to a variety of clinical scenarios in which a neural reflex results in usually self-limited systemic hypotension characterized by bradycardia and/or peripheral vasodilation. It is the most common cause of syncope (approximately 20 to 35 percent of cases), particularly in patients without apparent cardiac or neurologic disease. However, reflex syncope is the most common cause of syncope even among patients with heart disease and should be considered as a potential cause in such patients.
 syncope (also known as the common faint ) refers to a variety of clinical scenarios in which a neural reflex results in usually self-limited systemic hypotension characterized by bradycardia and/or peripheral vasodilation. It is the most common cause of syncope (approximately 20 to 35 percent of cases), particularly in patients without apparent cardiac or neurologic disease. However, reflex syncope is the most common cause of syncope even among patients with heart disease and should be considered as a potential cause in such patients.")
123
Reflex Syncope Vasovagal syncope is a common cause of syncope in athletes. However, other potential causes of syncope should be considered and evaluated before identifying the etiology of syncope, particularly if the syncope occurs during exertion. Athletes with syncope during physical activity should be evaluated for potential risk of sudden death.

124
History Reflex Syncope
Clinical presentation — Patients with vasovagal syncope are most commonly young and otherwise healthy. Typical triggers and premonitory symptoms are strongly suggestive of vasovagal syncope, although these may be absent or difficult to correlate to the syncopal episode. Women and patients younger than 40 are more likely to have typical symptoms. However, older patients are also frequently diagnosed with vasovagal syncope. Older individuals have specific triggers that may be absent in younger individuals (i.e., micturition, cough, defecation, deglutition).
.")
125
History Reflex Syncope
Vasovagal syncope (“classical”) refers to syncope triggered by emotional or orthostatic stress such as venipuncture (experienced or witnessed), painful or noxious stimuli, fear of bodily injury, prolonged standing, heat exposure, or exertion (post exertion).
 refers to syncope triggered by emotional or orthostatic stress such as venipuncture (experienced or witnessed), painful or noxious stimuli, fear of bodily injury, prolonged standing, heat exposure, or exertion (post exertion).")
126
History Reflex Syncope
Vasovagal syncope is often associated with a prodrome and persistence of nausea, pallor, and diaphoresis, consistent with increased vagal tone. Syncope is typically of short duration and occurs in the sitting or standing position. The supine position restores adequate blood flow to the brain.

127
History Reflex Syncope
However, full recovery may be delayed as the patient may feel depressed or fatigued. This course may help distinguish vasovagal syncope from syncope associated with arrhythmia, which is typically of abrupt onset and of short duration. Loss of consciousness may be prolonged with some other causes of syncope, such as seizures and aortic stenosis, but rarely with vasovagal syncope

128
Tilt Table Testing The tilt table test has limited specificity, sensitivity, and reproducibility.

130
Treatment Reflex Syncope
No therapy has been proven effective for recurrent vasovagal syncope. Some intuitively appealing therapies have not proven effective. Therapy is particularly important in patients who have recurrent syncope in high-risk settings (e.g., commercial vehicle driver, pilot) and who wish to continue these activities. Patients with recurrent episodes may require restriction of activities until therapy is shown to be effective.
 and who wish to continue these activities. Patients with recurrent episodes may require restriction of activities until therapy is shown to be effective.")
131
Treatment Reflex Syncope
Explanation — Patients with vasovagal syncope should be provided with reassurance and education regarding the nature, risks, and prognosis of the condition. The patient should be advised to assume the supine position with legs raised at the onset of symptoms. The patient should be advised to avoid trigger events when feasible, and medications that may induce hypotension should be modified or discontinued. A study of self-reported symptom burden in 418 patients diagnosed with vasovagal syncope indicated that 35 percent were symptom free at median five-year follow-up, regardless of presenting symptom or treatment received.

132
Treatment Reflex Syncope
Physical counterpressure — Studies have found that isometric activity, such as crossing the legs and the arms, may be helpful to offset a syncopal response, but release of this position may be associated with precipitous decline in heart rate and blood pressure. Counter-pressure maneuvers, such as tensing the arms with clenched fists, leg pumping, and leg-crossing may abort a syncopal episode or at least delay it long enough that patients can assume the supine position. Physical counterpressure maneuvers are intended to reduce lower-extremity venous pooling and therefore improve cardiac output and prevent vasovagal syncope.

133
Treatment Reflex Syncope
Maneuvers include: ■Leg-crossing with simultaneous tensing of leg, abdominal, and buttock muscles. ■Handgrip, which consists of maximum grip on a rubber ball or similar object. ■Arm tensing, which involves gripping one hand with the other while simultaneously abducting both arms

134
Treatment Reflex Syncope
Evidence from clinical trials suggests a limited role for pacemaker therapy in patients with vasovagal syncope.

135
Treatment Reflex Syncope
Some have recommended support stockings (in some cases, Jobst stockings), volume expansion by liberalizing salt intake, and occasionally administration of the mineralocorticoid fludrocortisone (similar to the regimen used in the treatment of orthostatic hypotension). Data are lacking to support this approach in treating reflex syncope.
, volume expansion by liberalizing salt intake, and occasionally administration of the mineralocorticoid fludrocortisone (similar to the regimen used in the treatment of orthostatic hypotension). Data are lacking to support this approach in treating reflex syncope.")
136
Treatment of Reflex Syncope
Beta blockers Although beta blockers have been the most commonly used drug therapy for vasovagal syncope, available evidence does not support their efficacy. They have been postulated to act upon the ill-defined afferent limb of the reflex arc involved in the Bezold-Jarisch reflex and to potentially also inhibit the discharge frequency of the C fibers originating from the cardiac mechanoreceptors and chemoreceptors.

137
Treatment Reflex Syncope
■Midodrine, an alpha-1-adrenergic agonist, had a beneficial effect in a small randomized trial and a number of observational studies. The benefits have ranged from prevention of syncopal episodes in 95 percent of previously untreated patients to efficacy for up to 22 months in as many as 78 percent of patients who failed to respond to a beta blocker or other conventional therapy. However, the efficacy of midodrine is uncertain, and another alpha agonist, etilefrine, was ineffective in a placebo-controlled study of 126 patients

138
Treatment Reflex Syncope
Some patients with vasovagal syncope respond poorly to general measures. Orthostatic or tilt training may be an effective approach, although study results have been mixed.

139
Treatment Reflex Syncope
The efficacy of orthostatic training started in hospital and continued at home was suggested by a controlled but non-randomized study. Forty-seven patients with recurrent syncope and a positive upright tilt table test who were refractory to traditional therapies were assigned to a tilt-training program or to continued medical therapy, depending upon their consent. The training program included five daily in-hospital upright tilt table studies increasing in duration from 10 to 50 minutes. The training program was continued at home with the patient instructed to stand against a wall for up to 40 minutes twice a day, under supervision of a family member.

140
Treatment Reflex Syncope
Wall stands with progressive increase in time over 6 to 8 weeks can improve symptoms, possibly by retraining baroreceptor reflexes. While the individual is standing, the upper back is positioned against a wall without arm and leg movement, beginning with 5-minute intervals twice daily and increasing gradually to 30-minute to 40-minute intervals over 6 to 8 weeks.

141
Treatment Reflex Syncope
Moderate exercise training — Limited uncontrolled data suggest that moderate exercise training may increase orthostatic tolerance in patients with syncope.

142
Driving Restrictions The 2009 ESC guidelines recommend no restriction with a single mild episode of vasovagal syncope in a private driver. If there are recurrent and severe episodes, private drivers are allowed to return to driving after symptoms are controlled. For a professional driver, no restriction is recommended for a single mild episode, unless it occurs during high-risk activity. For recurrent and severe episodes, permanent restriction is recommended unless effective treatment has been established.

143
References Vanderbilt Autonomic Dysfunction site ( DOI: /peds Pediatrics 2013;131;968; originally published online April 8, 2013; Julian M. Stewart Common Syndromes of Orthostatic Intolerance Postural Tachycardia Syndrome: A Heterogeneous and Multifactorial Disorder Eduardo E. Benarroch, MD, DScMayo Clin Proc. 2012;87(12):
:")
Similar presentations















>")

 58% Cardiac Disease (arrhythmias) 23% Neurologic or.>")






