Download presentation
Presentation is loading. Please wait.

1
Neoplasms of the Testis
Ch. 31 Omar Alhunaidi

2
Introduction 95% of testicular neoplasms are germ cell tumors (GCTs)
GCTs are broadly categorized as seminoma and nonseminoma (NSGCT) GCTs are relatively rare malignancies, accounting for 1% to 2% of cancers among men in the US
 GCTs are relatively rare malignancies, accounting for 1% to 2% of cancers among men in the US.")
3
Approximately 90% of GCTs arise in the testis and 2% to 5% are extragonadal
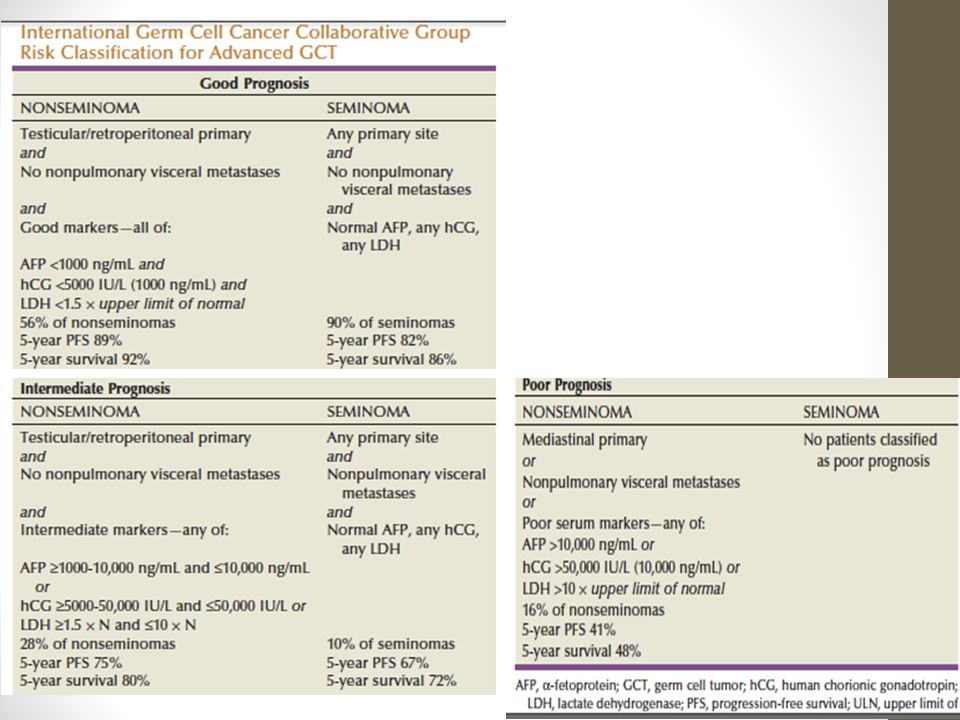
long-term survival for men with metastatic GCT is 80% to 90%

4
Non-GCTs of the testis are rare and include:
sex cord/stromal tumors lymphoid and hematopoietic tumor tumors of the collecting duct tumors of the testicular adnexa

5
Epidemiology In the US testicular cancer is the most common malignancy among men aged 20 to 40 years It is the second most common cancer after leukemia among males aged 15 to 19 years The incidence of bilateral GCT is approximately 2% Testicular lymphoma is less common than GCT but it is the most common testicular tumor in men > 50 years

6
Risk Factors Four well-established risk factors:
Cryptorchidism ( risk increase 4 to 6 times) Family history of testicular cancer Personal history of testicular cancer Intratubular germ cell neoplasia (ITGCN) * Infertile men also have a higher incidence of testicular cancer
 Family history of testicular cancer. Personal history of testicular cancer. Intratubular germ cell neoplasia (ITGCN) * Infertile men also have a higher incidence of testicular cancer.")
7
Most GCTs arise from a precursor lesion called intratubular germ cell neoplasia (ITGCN) (which is also referred to as carcinoma in situ). ITGCN is present in adjacent testicular parenchyma in 80% to 90% cases of invasive GCT Gene expression profile analysis indicates that ITGCN develops before birth from an arrested gonocyte

8
In men with a history of GCT, the finding of testicular microlithiasis on ultrasound evaluation of the contralateral testis is associated with an increased risk of ITGCN (Karellas et al, 2007). However, the significance of microlithiasis in the general population is unclear

9
Pathogenesis and Biology
The carcinogenesis of GCTs is poorly understood Testicular GCTs develop from a precursor lesion, ITGCN, which, in turn, appears to develop from arrested primordial germ cells or gonocytes that failed to differentiate into prespermatogonia Hussain et al, 2008 Approximately 70% of GCTs have an extra copy of chromosome 12 in the form of an isochromosome 12p (i[12p]

10
Increased incidence of other male reproductive disorders, such as:
Hypospadias Cryptorchidism Subfertility These findings led to the hypothesis that testicular cancer and these other disorders all resulted from a TESTICULAR DYSGENESIS SYNDROME, which is due to environmental and/or lifestyle factors

11
Environmental and/or lifestyle factors:
Increased prenatal estrogen exposure reduction in androgen activity mothers of children with testicular cancer have more pollutant in their blood *ALL ARE HYPOTHESIS

12
GCTs is sensitive to cisplatin-based chemotherapy, which enables cure in the vast majority of patients with widely metastatic disease.

13
Up to 10% of GCTs are extragonadal 2 main hypothesis:
they originate from germ cells that mismigrated along the genital ridge and were able to survive in an extragonadal environment Reverse migration from the testis to extragonadal locations

14
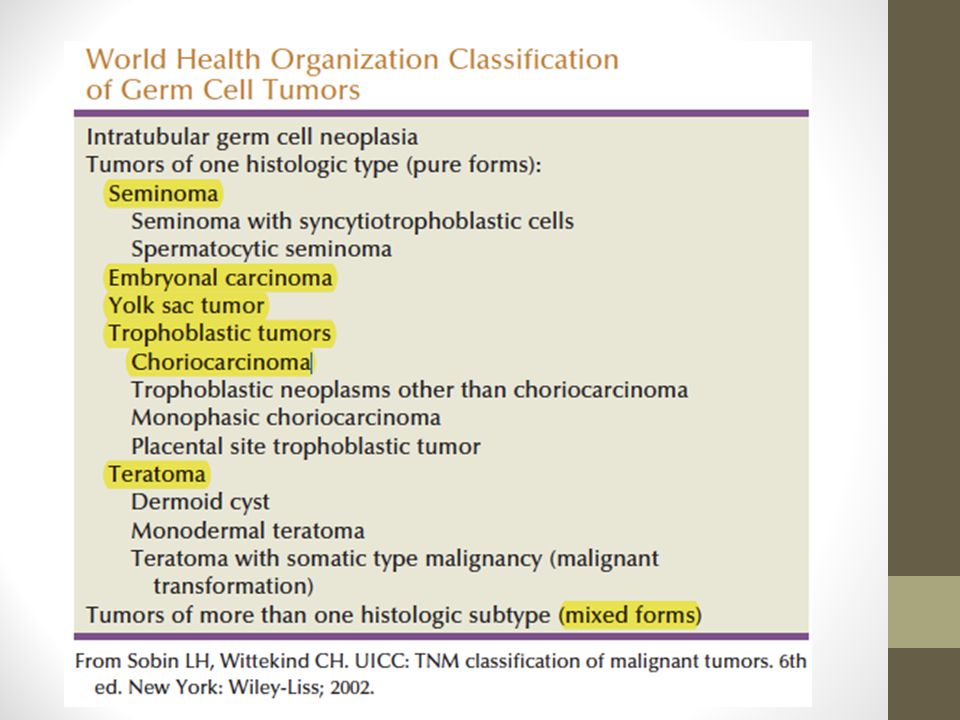
Histologic Classification
GCTs classified as: Seminoma (52% to 56%) NSGCT (44% to 48%) Embryonal carcinoma (EC) yolk sac tumor Teratoma choriocarcinoma
 NSGCT (44% to 48%) Embryonal carcinoma (EC) yolk sac tumor. Teratoma. choriocarcinoma.")
16
Intratubular Germ Cell Neoplasia
all adult invasive GCTs arise from ITGCN except for spermatocytic seminoma consists of undifferentiated germ cells that have the appearance of seminoma that are located basally within the seminiferous tubules tubule usually shows decreased or absent spermatogenesis presence of ITGCN in an orchiectomy specimen in men with testicular cancer does not carry any prognostic implications

17
Seminoma Seminoma is the most common type of GCT
Most cases diagnosed in the fourth or fifth decade Grossly, seminoma is a soft tan to white diffuse or multinodular mass

18
Spermatocytic Seminoma
Rare and accounts for less than 1% of GCTs Unlike other GCTs: does not arise from ITGCN not associated with a history of cryptorchidism does not express PLAP or i(12p) does not occur as part of mixed GCTs It is a benign tumor (only one documented case having metastasized) and is almost always cured with orchiectomy (Chung et al, 2004a).
 does not occur as part of mixed GCTs. It is a benign tumor (only one documented case having metastasized) and is almost always cured with orchiectomy (Chung et al, 2004a).")
19
Embryonal Carcinoma. most undifferentiated cell type of NSGCT, with totipotential capacity to differentiate to other NSGCT cell types Grossly, it is a tan to yellow neoplasm that often exhibits large areas of hemorrhage and necrosis aggressive tumor associated with a high rate of metastasis, often in the context of normal serum tumor markers

20
Choriocarcinoma rare and aggressive tumor
typically presents as elevated serum hCG levels and disseminated disease commonly spreads by hematogenous routes common sites of metastases: Lungs Brain ( DON’T FRGET TO IMAGE THE BRAIN) Eye and skin metastases are also been reported
 Eye and skin metastases are also been reported.")
21
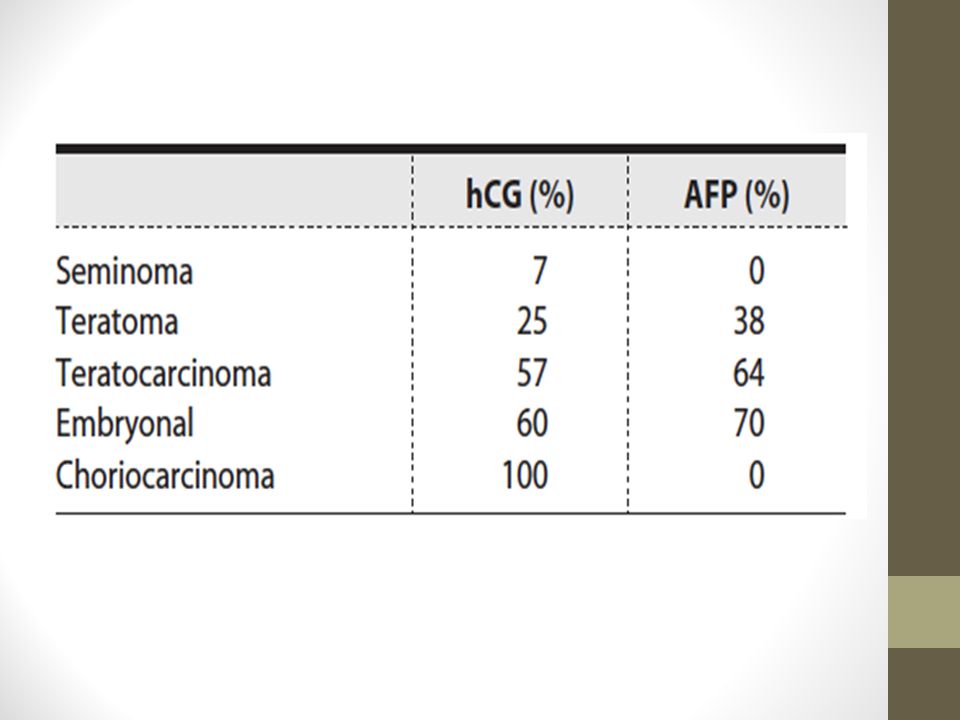
Yolk Sac Tumors Pure yolk sac tumors represent a very small fraction of adult-type GCTs but are more common in mediastinal and pediatric GCTs Schiller-Duval body is a characteristicfeature almost always produce AFP but not hCG

22
Teratomas are tumors that contain well-differentiated or incompletely differentiated elements of at least two of the three germ cell layers of: endoderm mesoderm Ectoderm Teratomas are generally associated with normal serum tumor markers, but they may cause mildly elevated serum AFP levels In adults, teratomas are histologically benign but are frequently found at metastatic sites in patients with advanced NSGCT Teratoma is resistant to chemotherapy

23
Growing Teratoma Syndrome:
Is when teratoma grows uncontrollably, invade surrounding structures, and become unresectable Rarely, it may transform into a somatic malignancy such as rhabdomyosarcoma, adenocarcinoma, or primitive neuroectodermal tumor Malignant transformation is highly aggressive, resistant to conventional chemotherapy, and associated with a poor prognosis

24
Initial Presentation The most common presentation of testicular cancer is a painless testicular mass Acute testicular pain is less common and is caused by rapid expansion of the testis due to intratumor hemorrhage or infarction Pain is more commonly associated with NSGCT, because these tumors tend to be more vascular and exhibit more rapid growth Symptoms related to metastatic disease are the presenting complaint in 10% to 20% of patients

25
Retroperitoneal metastasis may cause:
palpable mass abdominal pain flank pain due to ureteral obstruction back pain due to involvement of the psoas muscle or nerve roots lower extremity swelling due to compression of the inferior vena cava gastrointestinal symptoms.

26
Pulmonary metastasis may present as
dyspnea chest pain cough hemoptysis Metastasis to supraclavicular lymph nodes may present as neck mass

27
Approximately 2% of men have GYNECOMASTIA, resulting from either:
elevated serum hCG levels decreased androgen production increased estrogen levels (most commonly seen in men withLeydig cell tumors) Although approximately two thirds of men with GCT have diminished fertility, it is an uncommon initial presentation
 Although approximately two thirds of men with GCT have diminished fertility, it is an uncommon initial presentation.")
28
Physical Examination physician should carefully examine both testis
Atrophy of the affected or contralateral testis is common, more with h/o cryptorchidism Any firm area within the testis is suggestive of malignancy hydrocele may accompany a testicular cancer and impair the examination

29
Patient should also be examined for any evidence of:
palpable abdominal mass or tenderness inguinal lymphadenopathy (mainly if he had prior inguinal or scrotal surgery) gynecomastia supraclavicular lymphadenopathy Auscultation of the chest
 gynecomastia. supraclavicular lymphadenopathy. Auscultation of the chest.")
30
A firm intratesticular mass should be considered cancer until proven otherwise and should be evaluated further with scrotal U/S

31
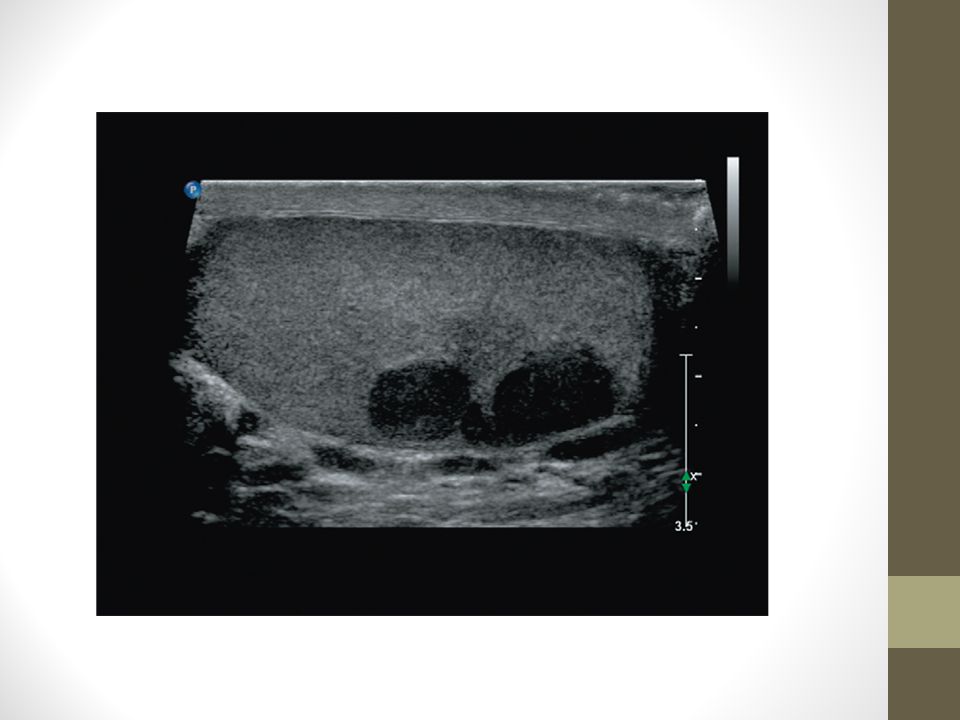
Diagnostic Testing Scrotal U/S should be considered after examination because it is inexpensive and noninvasive On ultrasonography the typical GCT is hypoechoic and two or more discrete lesions may be identified Heterogeneous echotexture within a lesion is more commonly associated with NSGCT, because seminomas usually have a homogeneous echotexture

33
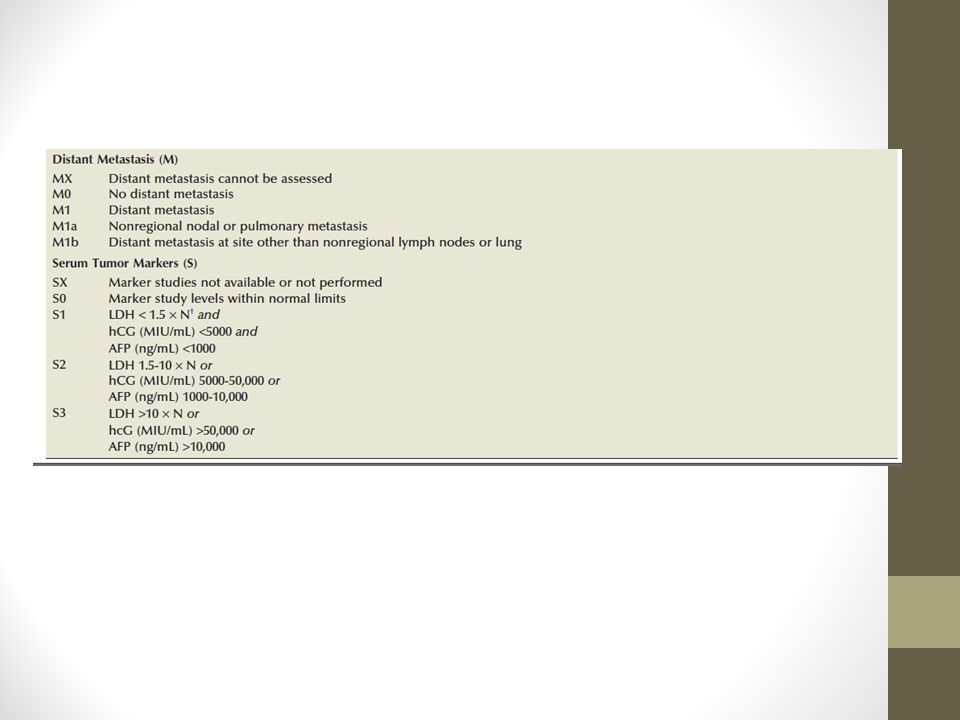
Serum Tumor Markers LDH AFP hCG
They are essential in its diagnosis, prognosis, treatment, and monitoring AFP is elevated in: 50% to 70% of low-stage (CS I, IIA, IIB) NSGCT 60% to 80% of advanced (CS IIC, III) NSGCT
 NSGCT. 60% to 80% of advanced (CS IIC, III) NSGCT.")
34
EC and yolk sac tumors secrete AFP
Choriocarcinomas and seminomas do not produce AFP The half-life of AFP is 5 to 7 days AFP levels may also be raised in patients with hepatocellular carcinoma Stomach ca Pancreas ca biliary tract ca Lung ca

35
hCG levels are elevated in
20% to 40% of low-stage NSGCT 40% to 60% of advanced NSGCT 15% of seminomas secrete hCG hCG is also secreted by choriocarcinoma and EC The half life of hCG is 24 to 36 hours

36
hCG levels may be elevated in cancers of the:
liver biliary tract pancreas stomach lung Breast kidney bladder

38
LDH levels are elevated in:
20% of lowstage GCTs 20% to 60% of advanced GCTs LDH is expressed in smooth, cardiac, and skeletal muscle Lymphoma may also cause elevated LDH levels

39
Patients suspected of having a GCT should do serum AFP, hCG, and LDH evaluation
before orchiectomy to aid in the diagnosis and to help interpret postorchiectomy tumor marker levels

40
Initial Management Radical inguinal orchiectomy when testicular neoplasm is suspected, with removal of the tumor-bearing testis and spermatic cord to the level of the internal inguinal ring A transscrotal orchiectomy or biopsy is contraindicated because: it leaves the inguinal portion of the spermatic cord intact and may alter the lymphatic drainage of the testis increasing the risk of local recurrence Pelvic or inguinal lymph node metastasis

41
Because of the rapid growth of GCT, orchiectomy should performed in a timely manner and delays greater than 1 to 2 weeks should be avoided

42
Testis-sparing surgery (or partial orchiectomy)
is highly controversial and has no role in the patient suspected of having a testicular neoplasm with a normal contralateral testis It MAY be considered for organ confined tumors of less than 2 cm in patients with bilateral tumors or tumor in a solitary testis Also it may be considered for suspected benign tumor or indeterminate lesion when serum AFP, hCG, and LDH values are normal.

43
When testis-sparing surgery is performed, biopsies of the adjacent testicular parenchyma should be done to R/O ITGCN Adjuvant radiotherapy to the residual testis is usually sufficient to prevent the development of a GCT

44
Biopsy of the Contralateral Testis
Open inguinal biopsy of the contralateral testis may be considered in patients with risk factors for ITGCN or those with suspicious lesions on preoperative ultrasonography

45
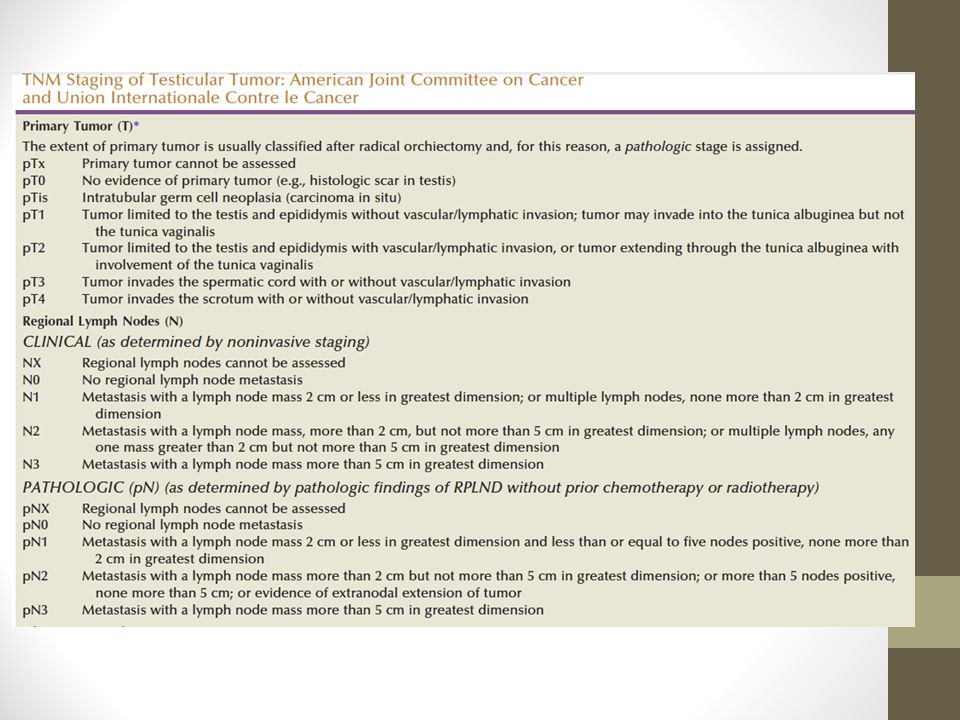
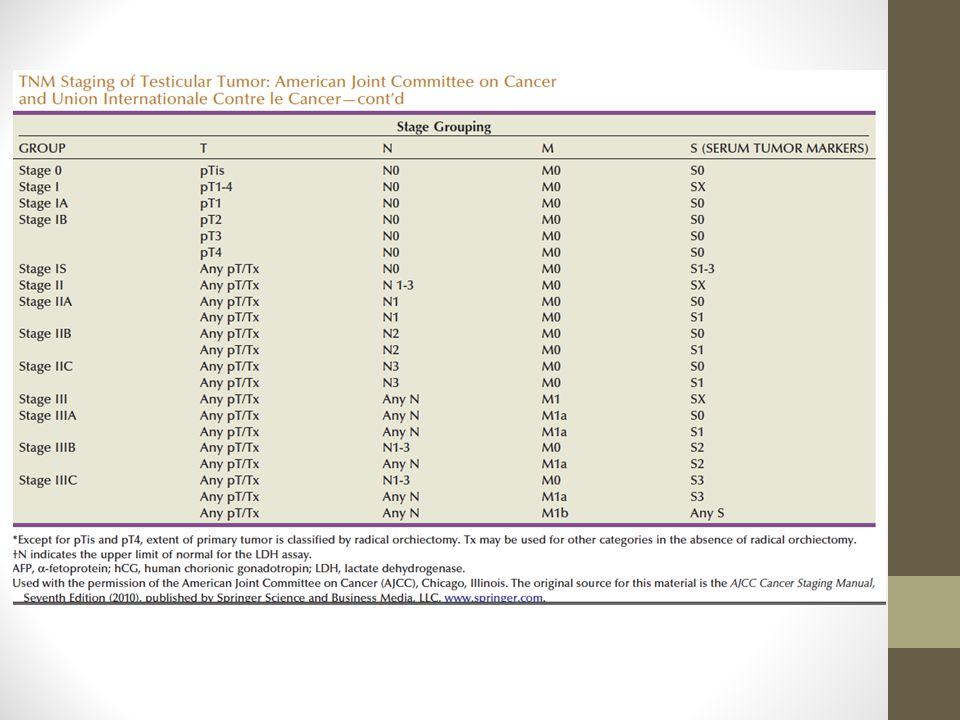
Clinical Staging The prognosis of GCT and initial management decisions are dictated by the clinical stage of the disease by histological and radilogical findings Lymphatic spread is the most common route of disease dissemination, except for Choriocarcinoma. Retroperitoneum is the initial site of metastatic spread in 70% to 80% of patients with GCT

46
Clinical Staging CS I : disease clinically confined to the testis CS II : indicates the presence of regional (retroperitoneal) lymph node metastasis CS III : represents nonregional lymph node and/or visceral metastasis.
 lymph node metastasis. CS III : represents nonregional lymph node and/or visceral metastasis.")
47
For RIGHT testicular tumors the primary drainage site is the interaortocaval lymph nodes inferior to the renal vessels, followed by the paracaval and para-aortic nodes. For LEFT testicular tumors is the para-aortic lymph nodes, followed by the interaortocaval nodes Distal iliac and inguinal lymph nodes secondary to large volume disease or aberrant testicular lymphatic drainage

48
All patients with GCT should do CT Abd+Pelvis with oral & IV contrast for staging
(MRI) is an alternative to CT
 is an alternative to CT.")
49
All patients with GCT should undergo chest imaging
Thoracic metastasis in the absence of retroperitoneal disease and/or elevated serum tumor markers is uncommon Routine chest CT may be associated with a high rate of false-positive findings

50
Serum Tumor Markers Postorchiectomy AFP, hCG, and LDH levels are important for staging, prognosis, and treatment selection presence of newly elevated and / or rising serum tumor marker levels after orchiectomy indicates metastatic disease

55
Therapeutic Principles
After orchiectomy, staging imaging studies, serum tumor marker status, and treatment plans should be performed as soon as possible Cisplatin which is a nephrotoxic chemotherapy is often administered even in the presence of moderate-to-severe renal insufficiency Seminoma is associated with increased sensitivity to radiation therapy and platin-based chemotherapy compared with NSGCT. Aggressive surgical approach is taken to resect all sites of residual disease after chemotherapy for NSGCT

56
Sperm cryopreservation should be offered to all patients before RPLND, chemotherapy, or radiation therapy owing to the potential effects of these treatments on fertility.

57
MANAGEMENT NSGCT The optimal management of CS I NSGCT is controversial. Surveillance, primary RPLND, and primary chemotherapy with BEPAx2 (+ adjuvant bleomycin-etoposide-cisplatin) are accepted treatment options, with long-term survival rates approaching 100% for each. Surveillance is not recommended to patients who are anticipated to be poorly compliant with follow-up imaging and clinical evaluation. BEPx2 is the standard regimen used for patients with CS I NSGCT who choose to receive chemotherapy
 are accepted treatment options, with long-term survival rates approaching 100% for each. Surveillance is not recommended to patients who are anticipated to be poorly compliant with follow-up imaging and clinical evaluation. BEPx2 is the standard regimen used for patients with CS I NSGCT who choose to receive chemotherapy.")
58
Adjuvant chemotherapy after primary RPLND for pathologic stage II disease is associated with a reduced risk of relapse Adjuvant chemotherapy is usually recommended to patients with extensive retroperitoneal metastasis (pN2-3) and those anticipated to be noncompliant with postoperative cancer surveillance imaging and testing
 and those anticipated to be noncompliant with postoperative cancer surveillance imaging and testing.")
59
Induction chemotherapy and primary RPLND are accepted treatment options for patients with CS IIA-B NSGCT, with long-term cure in 95%

60
management of patients with CS IS, IIC, and III NSGCT is induction cisplatin-based chemotherapy
Patients with good-risk disease should receive BEPx3 or BEPx4 Those with intermediate- and poor-risk disease should receive BEPx4 Postchemotherapy resection of all residual masses is based on the incidence of residual cancer

61
MANAGEMENT OF SEMINOMA
The optimal management of CS I seminoma is controversial Surveillance, primary radiotherapy, and primary chemotherapy with carboplatin (one to two cycles) are accepted treatment with long-term survival rates approaching 100% for each Surveillance is not recommended to patients who are anticipated to be poorly compliant
 are accepted treatment with long-term survival rates approaching 100% for each. Surveillance is not recommended to patients who are anticipated to be poorly compliant.")
62
For CS IIA-B seminoma, radiotherapy and first-line chemotherapy (BEPx3 or BEPx4) are accepted treatment with nonbulky (<3 cm) retroperitoneal lymph node metastasis. For bulky (>3 cm) and/or multifocal retroperitoneal metastases, first-line chemotherapy (BEPÅ~3 or EPÅ~4) is recommended The treatment of patients with CS IIC and III seminoma is first-line cisplatin-based chemotherapy
 and/or multifocal retroperitoneal metastases, first-line chemotherapy (BEPÅ~3 or EPÅ~4) is recommended. The treatment of patients with CS IIC and III seminoma is first-line cisplatin-based chemotherapy.")
63
NON–GERM CELL TUMORS

64
term refers to neoplasms containing
Sex cord/stromal tumors are rare, comprising approximately 4% of testicular neoplasms term refers to neoplasms containing Leydig cells Sertoli cells Granulosa cells Thecal cells

65
Leydig cell tumors are the most common of the sex cord/stromal tumors
no association with cryptorchidism occur in adult males between age 20 and 60 years Common presentation is a painless testicular mass Frequently p/w feminizing characteristics including: gynecomastia impotence, decreased libido

66
Radical inguinal orchiectomy is the initial treatment of choice
90% of these tumors are benign, and 10% are malignant The most frequent metastatic sites are the retroperitoneum and lung. Metastatic Leydig cell tumors are resistant to chemotherapy and radiation therapy

67
Sertoli Cell Tumor less than 1% of testicular neoplasms. occur in any age group, including infants no association with cryptorchidism Treatment is radical inguinal orchiectomy Ninety percent of tumors are benign, and 10% are malignant

68
Thank u

Similar presentations






>")







; FRCS (Ireland); MMed (Wits); FCS (SA) Urology 38 th BMA CONGRESS.>")






