Download presentation
Presentation is loading. Please wait.

1
Testis Dr. Raid Jastania

2
Objectives By the end of this session the student should be able to:
List common causes of scrotal swelling Classify testicular tumors List the gross and microscopic features of germ cell tumors

3
Scrotum Scrotal enlargement Squamous cell carcinoma and chimney sweeps
Hydrocele: accumulation of serous fluid in the tunica vaginalis Hematocele Chylocele Squamous cell carcinoma and chimney sweeps

4
Cryptorchidism Undescended testis 0.7-0.8% of males
Descent occurs in the last 2 months of intrauterine life Risk factors: Hormonal abnormalities Prematurity Testicular abnormalities Mechanical problems Congenital syndormes

5
Cryptorchidism Right > left Can result in infertility
Risk of malignancy : x4 May result in atrophy Tubular atrophy, hyalinization Hyperplasia of leydig cells Intratubular germ cell neoplasia

6
Epididymitis, Orchitis
Infections (acute, chronic, granulomatous) Follow UTI Associated with mumps in 20% of adults, rare in children
 Follow UTI. Associated with mumps in 20% of adults, rare in children.")
7
Granulomatous orchitis

8
Testicular torsion and infarction

9
Testicular Neoplasm Most common cause of painless, firm enlargement of the testis 2/100,000 male 15-35 year Classification Germ cell tumors Sex cord tumors

11
Germ cell tumors Seminoma Non-Seminoma 1. Teratoma 2. Embryonal carcinoma 3. Yolk sac tumor 4. Choriocarcinoma Mixed Germ cell tumors (60%)
")
12
Genetic finding: Isochromosome 12
Risk factors: Testicular abnormalities: undesceded testis, testicular dysgenesis Chromosomal syndromes: Klinefelter Family history White > Black Intratubular germ cell neoplasia Genetic finding: Isochromosome 12

13
Case Presentation

14
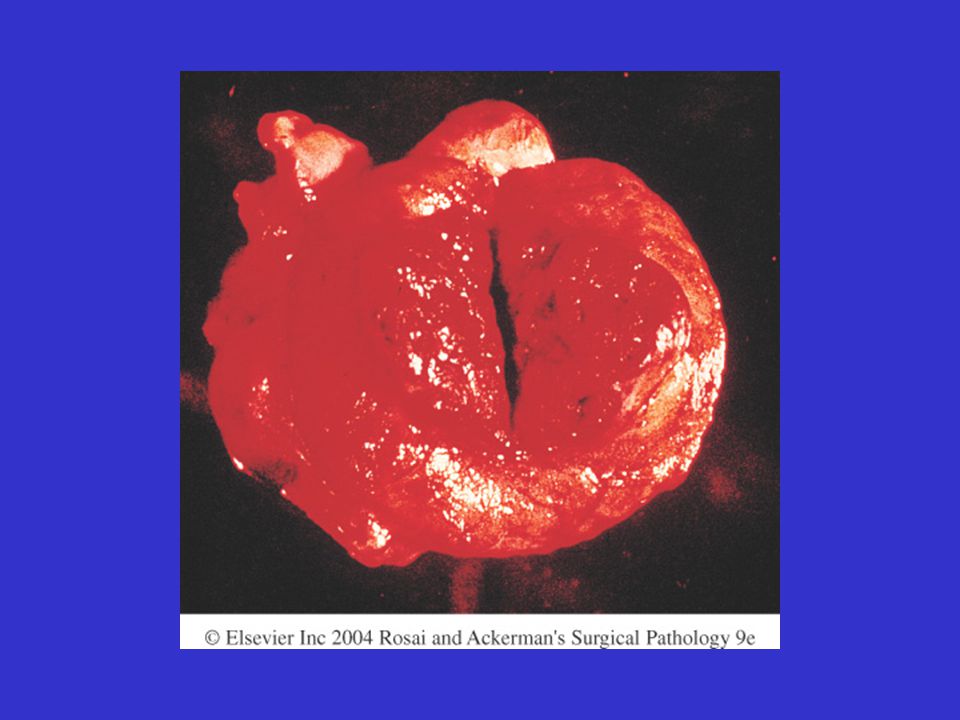
A 35-year-old healthy male with a past history of cryptorchidism repaired at age 5 presented with painless enlargement of the left testis. The mass was opaque on transillumination. A testicular ultrasound examination revealed the enlargement to be composed of soft tissue without a cystic component. Laboratory data included serum HCG of 90 mU/mL (ref. range < 5 mU/mL) and AFP of 7 ng/mL (ref. range 0-44 ng/mL). A radical left orchiectomy was performed.
 and AFP of 7 ng/mL (ref. range 0-44 ng/mL). A radical left orchiectomy was performed.")
15
The left testicle was dominated by a 4. 0-cm, pink-tan nodular mass
The left testicle was dominated by a 4.0-cm, pink-tan nodular mass. An abdominal CT scan revealed para-aortic lymphadenopathy; a chest x-ray was normal. Radiotherapy was given to the abdominal retroperitoneal region.

17
Seminoma Age years Large, soft, well-demarcated, homogenous mass, gray-white (may show hemorrhage, necrosis) Large cells, round nuclei with porminent nucleoli Inflammatory cells Malignant

21
Teratoma All ages Firm mass, may contain cartilage Types
Mature Immature Teratoma with malignant transformation All are considered malignant except mature teratoma in children.

24
Embryonal carcinoma Age 20-30 years
Ill-defined mass with hemorrhage and necrosis Large cells, large nuclei with glandular structures Malignant

26
Yolk Sac tumor Children: 3 years Large tumor, well demarcated
Cuboidal cells forming microcysts Eosinophilic hyaline globules Schiller-Duvall bodies Alpha feto protien (AFP) Malignant
 Malignant.")
29
Choriocarcinoma Age 20-30 years Small, hemorrhagic
Cytotrophoblasts, Syncytiotrophobalsts hCG Malignant

32
Mixed Germ cell tumor 60% Teratoma + Embryonal carcinoma
Teratoma + Yolk sac tumor

34
Clinical Issues Stage I: tumor limited to testis
Stage II: Retroperitoneal lymph nodes Stage III: beyond retroperitoneal lymph nodes Tumor markers hCG AFP Seminoma is radiosensitive

35
70 year old man with testicular mass

Similar presentations



















; FRCS (Ireland); MMed (Wits); FCS (SA) Urology 38 th BMA CONGRESS.>")











