Download presentation
Presentation is loading. Please wait.

1
Supraventricular Tachycardia and Atrial Fibrillation
Courtney Bunevich, D.O. August 15, 2007

2
SVT: Clinical Features
Regular, rapid rhythm Usually narrow complex rhythm Arises from atria or atrioventricular nodal tissue above the bundle of His that initiate and maintain the rhythm Either a reentry or an ectopic pacemaker above the bundle of His

3
SVT: Pathophysiology Reentry: SVT associated with reentry is PSVT
AV nodal reentry (AVNR) occurs in 60% of cases Orthodromic AVNR is antrograde conduction via AV node and retrograde conduction via accessory pathway AV reentry via an accessory pathway in 30% Intra-atrial reentry s/p cardiac surgery after large atrial incision with scar formation Sinus node reentry, inappropriate sinus tachycardia, ectopic junctional tachycardia, and nonparoxysmal junctional tachycardia are rare
 occurs in 60% of cases. Orthodromic AVNR is antrograde conduction via AV node and retrograde conduction via accessory pathway. AV reentry via an accessory pathway in 30% Intra-atrial reentry s/p cardiac surgery after large atrial incision with scar formation. Sinus node reentry, inappropriate sinus tachycardia, ectopic junctional tachycardia, and nonparoxysmal junctional tachycardia are rare.")
4
PSVT: Clinical Features
Can occur in a structurally normal heart Can be associated with rheumatic heart disease, acute pericarditis, MI, MVP, and preexcitation syndromes. Exacerbated by caffeine, alcohol, illicit drugs, hyperthyroidism, diet supplements, herbal supplements (ginseng). Can be induced by PACs and PVCs
. Can be induced by PACs and PVCs.")
5
PSVT: Signs and Symptoms
Sudden onset and termination Can occur in patients of all ages Regular, tachycardia Palpitations, anxiety, diaphoresis, lightheadedness, chest pain, dyspnea, pounding in chest and neck. Syncope is uncommon Polyuria if SVT prolonged secondary to release of atrial natriuretic peptide

6
Differential Diagnosis
Atrial fibrillation/ Atrial flutter/ MAT Onset usually in patients > 60 y/o Patients usually heave heart disease Irregularly Irregular rhythm Ventricular Tachycardia Patients usually > 50 y/o Patients usually have IHD Present with syncope and SCD Wide complex regular rhythm Abrupt onset

7
Physical Exam Patient can be diaphoretic, anxious, hypotensive, or even asymptomatic Prominent jugular venous A wave from atrial contraction against closed tricuspid valve “frog sign”

8
Emergency Care Get immediate set of vital signs including pulse oximetry, IV, O2, monitor. EKG CKMB and Trop I, TSH, FT4 BMP Connect patient to continuous 12 lead EKG Is patient stable? Do they need immediate cardioversion?

9
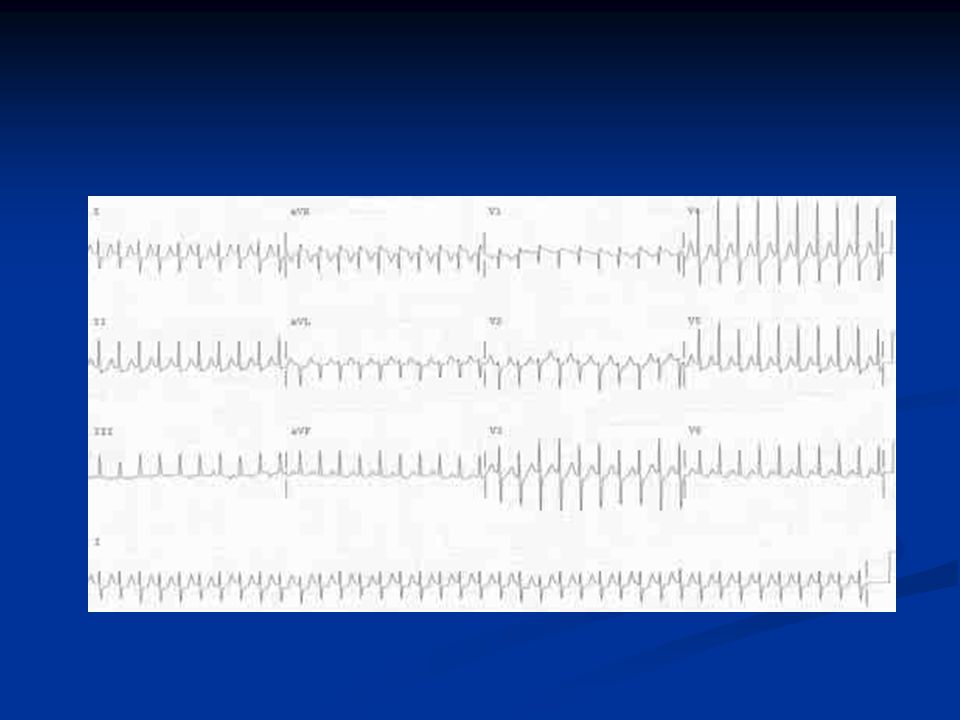
EKG The EKG in PSVT is usually a narrow, regular complex tachycardia.
Less than 10% of cases will have SVT with aberrancy To be discussed later

11
Treatment Try a vagal maneuver to slow rhythm to see the underlying rhythm. Carotid sinus massage Do if no bruits auscultated and no known carotid disease Massage for 5 seconds and release Can also place an ice pack on the forehead

12
Treatment Adenosine Causes flushing, CP, dyspnea
Half life is 15 seconds First line treatment is Adenosine 6 mg IVP If unsuccessful, give Adenosine 12mg IVP x 2 Cause transient AV nodal block by hyperpolarization of the node Complications include bronchospams and VF Will not work if patient has heart transplant C/I if wide complex tachyarrhythmia Caution in patients with severe COPD Adensione 6mg terminate in 60-80% patients Adenosine 12mg will terminate in 90-95% of patients

14
Treatment Next line treatments:
Verapamil mg /kg IV can repeat in 30 min. Hypotension can occur but can prevent this by giving CaCl2 10% 4mL. Not commonly used. Diltiazem mg bolus then continuous infusion in at 5-15 mg/hour Esmolol protocol Metoprolol 5mg IV q5 x 3

15
Treatment Consider cardioversion or venous atrial or ventricular temporary pacing if unable to slow rhythm down with adenosine, CCB, and BB before giving antiarrhythmics. Can also give IV flecainide, IV procainamide, IV propafenone, IV ibutilide These drugs can cause hypotension, bradycardia, and are proarrhythmic.

16
Synchronized Cardioversion
Should be used immediately in any unstable patient with hypotension, pulmonary edema, chest pain, or other unstable signs. Required dose is usually small: 50 Joules

17
Long term Treatment Risk of developing long term PSVT after single episode not defined. One episode is not indication for long term treatment.

18
Long term Treatment SVT with No Preexcitation
Verapamil, Beta blockers, and Diltiazem Decrease symptoms in 30-60% Randomized clinical trials show no superiority Failure on a single drug therapy can try a combo of two or add one a class IC or class III antiarrhythmic Long term treatment with class IC not recommended, and patents should be referred for catheter ablation

19
Catheter Ablation Radiofrequency and Cyrothermal
95% success rate initially <5% recurrence rate in the 1st few months Complications occur in 2-3% Damage to arteries, bleeding, AVF, venous thrombosis, PE, myocardial perforation, valvular damage, systemic embolism, and death (rare) Blocking near the AV node can cause total block of the AV node and patient will need a pacemaker
 Blocking near the AV node can cause total block of the AV node and patient will need a pacemaker.")
20
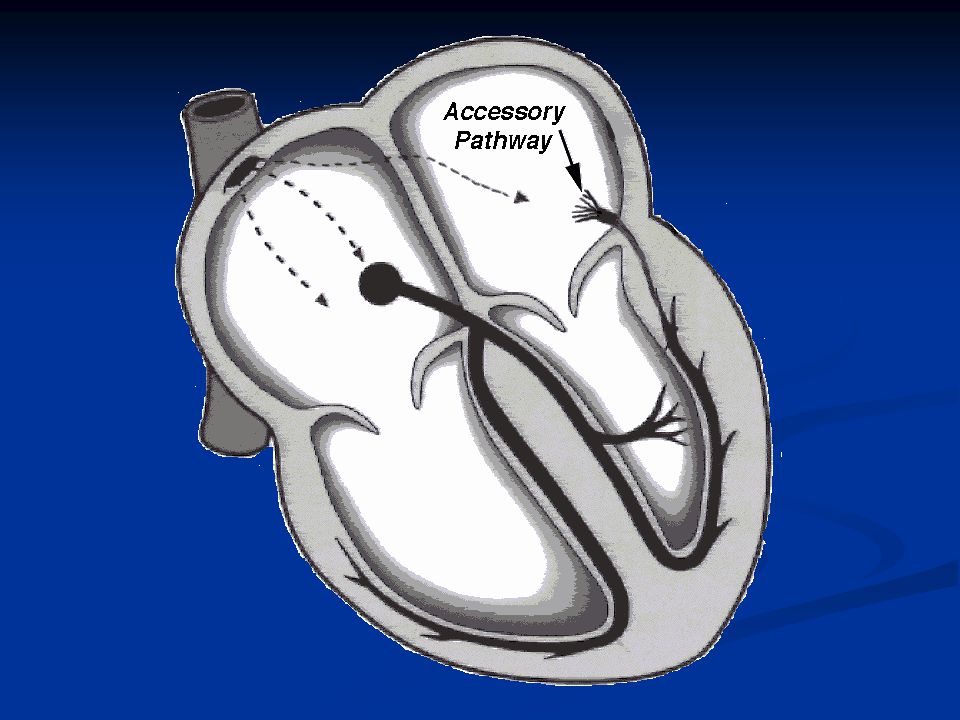
Wolf Parkinson White Associated Ebstein’s anomaly
EKG will show a short PR interval, a delta wave, and a QRS interval up to 0.12 msec Accessory pathway is the Bundle of Kent

23
Wolf Parkinson White Has 2 mechanisms for PSVT
Orthodromic, narrow complex (95%) Antrograde conduction via AV node and retrograde conduction via accessory pathway Can treat like PSVT Antidromic, wide complex (5%) Antrograde conduction via accessory pathway and retrograde conduction via AV node DO NOT give Digoxin, BB, Verapamil Try procainamide and cardioversion
 Antrograde conduction via AV node and retrograde conduction via accessory pathway. Can treat like PSVT. Antidromic, wide complex (5%) Antrograde conduction via accessory pathway and retrograde conduction via AV node. DO NOT give Digoxin, BB, Verapamil. Try procainamide and cardioversion.")
25
SVT with WPW Catheter ablation is the treatment of choice once stable
Risk of sudden death is 0.15 – 0.45 % / year

26
Wolf Parkinson White Can degenerate into Atrial Fibrillation
If life threatening: do immediate cardioversion. If not unstable, you can try procainamine, amiodarone, or lidocaine Caution verapamil, BB, and digoxin will cause degeneration into ventricular fibrillation!!

27
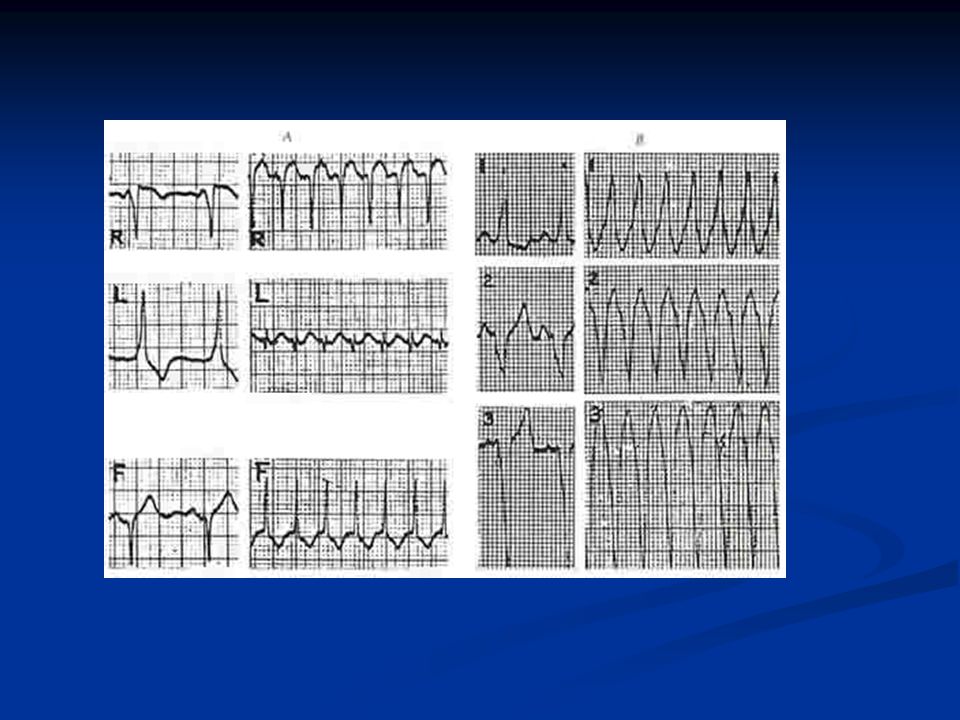
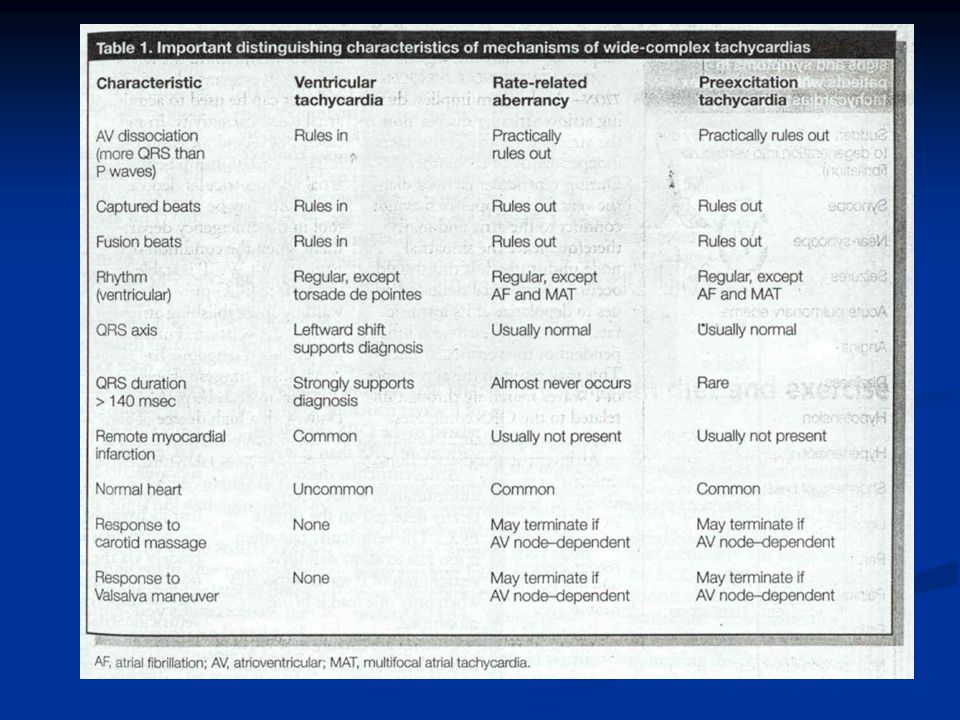
SVT with aberrancy Occur in less than 10% of cases
Regular, wide complex tachycardia Causes: SVT with a preexcitation syndrome Antidromic reentry seen in <5% cases of patients who have WPW Patient with a preexisting BBB Bundle branch fatigue in PSVT

30
Atrial Fibrillation Uncoordinated atrial activation with deterioration of atrial mechanical dysfunction Ventricular response to atrial fibrillation depends on the integrity and electrophysical properties of the AV node Most common arrhythmia encountered in clinical practice

31
Atrial Fibrillation Most common sustained tachyarrhythmia patients seek treatment for Affects 0.4-1% of the general population and 8% of patients greater than 80 years old AF occurring in patient without structural heat disease and less than 65 y/o is termed lone AF Types: First episode Paroxysmal (self-terminating) Persistent (requiring electrical or pharmacological treatment) Permanent
 Persistent (requiring electrical or pharmacological treatment) Permanent.")
32
Atrial Fibrillation Irregularly, irregular rhythm
Can be associated with rapid ventricular conduction/response or AF with RVR No atrial kick in atrial fibrillation. The firing of the atria and ventricles is not synchronized. In patients with systolic dysfunction, the atria makes an important contribution Biopsies have shown patchy fibrosis of fibers in atria Foci can be found in atria, pulmonary arteries, coronary sinus Atrial rate is beats/min Multiple small areas of the atria are firing and contracting (quivering) Ventricular conduction rate is variable bpm
 Ventricular conduction rate is variable bpm.")
33
Causes for Atrial Fibrillation
Rheumatic heart disease Nonrheumatic mitral valve disease disease Hypertension Chronic lung disease ASD Thyrotoxicosis * Lone AF Ischemic heart disease Acute MI * Dilated cardiomyopathy Holiday heart- Alcohol ingestion * Theophylline toxicity Pheochromocytoma

34
Causes for Atrial Fibrillation
Pericarditis * Electrocution * Post cardiothoracic surgery * Myocarditis * Pulmonary embolism * Obesity Intracardiac tumors or thrombi Amyloidosis SAH or CVA Familial AF

35
Signs and Symptoms Can be severe:
Pulmonary edema, palpitations, angina, and syncope Relatively asymptomatic Nonspecific symptoms such as fatigue

36
Treatment of AF with RVR
Get an immediate set of vitals, pulse oximetry. Place a patient on a monitor and O2. Get IV access. Get EKG. Check BMP. Check CKMB and Trop I. Get CXR. Check TSH and FT4. How long has AF been present? <48hrs or >48hrs or unknown Is patient unstable? Do they need immediate cardioversion?

38
Treatment of AF with RVR Rate Control
Medications: IF preserved EF > 40% Diltiazem mg IV bolus and run a drip in at 5-15 mg/hour. Can repeat the bolus if needed. Esmolol protocol Metoprolol 5mg IV q5 min x 3

39
Treatment of AF with RVR Rate Control
Medications: If EF < 40% Recommend: Diltiazem mg IV bolus and run a drip in at 5-15 mg/hour. Can repeat the bolus if needed. Amiodarone 150mg IV over 1 minute then 1 mg/minute for 6 hours then 0.5 mg/min for 18 hours Caution if patient on digoxin Watch for hypotension Low efficacy for acute conversion

40
Treatment of AF with RVR Rhythm Control
If duration is < 48 hours and EF > 40% DC Cardioversion at 100 Joules (60%) , 200 Joules (80%) ONLY ONE of the following: Amiodarone, ibutilide, flecainide, propafenone, and procainamide
 , 200 Joules (80%) ONLY ONE of the following: Amiodarone, ibutilide, flecainide, propafenone, and procainamide.")
41
Treatment of AF with RVR Rhythm Control
If duration < 48 hours and EF< 40% DC cardioversion or Amiodarone

42
Treatment of AF with RVR Rhythm Control
If duration > 48 hours or unknown Do rate control. Start anticoagulation for 4 weeks with therapeutic INR. Exclude clot. Do cardioversion. Continue anticoagulation for 4 more weeks. Begin IV heparin. TEE exclude clot. Cardioversion. Anticoagulation for 4 weeks.

43
TEE TEE will show thrombus in 5-15% in atrial fibrillation preparing for cardioversion Thromboembolic events have been reported after “normal” TEE and cardioversion Contrast enhanced MRI is evolving diagnostic modality for evaluation intracardiac thrombi Statins have been shown to decreases risk of recurrent AF after cardioversion possible due to anti-inflammatory affects

44
Atrial Fibrillation AFFIRM trial 2002 showed no mortality differences between rate and rhythm control groups. Rhythm control should be reserved for patients who are symptomatic even when rate controlled. Patients need either rate or rhythm control and anticoagulation

45
New Onset AF Minimal Evaluation:
H and P for symptoms, type of AF, date of onset and duration, treatment given, co-morbid or predisposing conditions ECG- evaluate rhythm, LVH, preexcitation syndromes, BBB, and old MI TTE- evaluate LV function, clots (inferior), valvular disease Labs: TSH, Renal and Hepatic function
, valvular disease. Labs: TSH, Renal and Hepatic function.")
46
New Onset AF Additional Testing:
6 minute walk test to assess for adequate rate control Exercise stress test Holter monitor TEE Electrophysical studies

47
Atrial Fibrillation AFFIRM trial showed that patients despite being in sinus rhythm are still at high risk of stroke. Patients with paroxsymal AF still must be anticoagulated. CHADS2: criteria recommended that scores 0-2 can use aspirin safely and scores greater than 3 need warfarin in those with nonvalvular AF CHF – 1 point HTN – 1 point Age > 75 years – 1 point DM – 1 point Prior Stroke or TIA – 2 points

48
CHADS2 Score: Stroke rate per year (%): 1 2 3 4 5 6 1.9 2.8 4.0 5.9
1 2 3 4 5 6 Stroke rate per year (%): 1.9 2.8 4.0 5.9 8.5 12.5 18.2
:")
49
Risk of Stroke Atrial fibrillation is associated with increased risk of stroke, heart failure, and all cause mortality 5% per year risk of CVA in patients with nonvalvular atrial fibrillation Framingham study showed 17 times increased risk of CVA in patients with valvular AF and 5 times increased risk in those with nonvalvular AF 1.5% risk of CVA in patients age 50-59 23.5% risk of CVA in patients age 80-89

50
Risk of Stoke NYHA classification: Risk of stroke/year (%): I II-III
IV Risk of stroke/year (%): 4% 12-26% 27-50%
: 4% 12-26% 27-50%")
51
Risk of Stroke Risk Factors: Relative Increased Risk: CVA/TIA DM HTN
HF Age per decade Relative Increased Risk: 2.5 1.7 1.6 1.4

52
ASA Treatment Treat of AF with ASA is a Class I recommendation by the 2006 ACC guidelines in the following subsets of patients: Age < 60 and no heart disease Age with heart disease and no risk factors Age and no heart disease Risk factors: Heart failure, EF<35%, HTN

53
Pharmacologic Cardioversion
Ibutilide is the only drug FDA approved for pharmacologic cardioversion 45% conversion rate for AF 60% conversion rate for Atrial Flutter Class III agent with a 4-8% risk of TdP Higher if patient has CHF or cardiomyopathy 0.01mg/kg (max 1 mg) over 10 minutes Have external defibrillator ready Monitor of telemetry for at least 4 hours
 over 10 minutes. Have external defibrillator ready. Monitor of telemetry for at least 4 hours.")
54
Pharmacologic Cardioversion
Digoxin and sotalol are NOT recommended for pharmacologic cardioversion These drugs gave Class I and IIa recommendations for pharmacologic cardioversion: Dofetilde Flecanide Propafenone Ibutilide Amiodarone (IIa)
")
55
Electrical Cardioversion
Recommended if symptoms are known to be less than 48 hours Unstable in patients without accessory pathway Unstable or in tachycardic patients with an accessory pathway Patients unable to tolerate symptoms Contraindicated in hypokalemia and digitalis toxicity

56
Other Treatments Maze procedure
Can do as an adjunct procedure during open heart surgeries Catheter ablation after EP studies to determine irritable foci AVN ablation can be useful in patients with tachycardia-mediated cardiomyopathy Small study showed increase in EF from 26% to 34% after AVN and pacemaker implantation

58
References Harrison’s Internal Medicine 16th Edition
2006 ACC Guideline for Atrial Fibrillation New England Journal of Medicine Supraventicular Tachycardia 9 March pp volume 354 American Journal of Emergency Medicine Wide Complex Tachycardias: Beyond Traditional Differential Diagnosis of Ventricular Tachycardia versus SVT with Aberrant Conduction November pp 876 volume 23 AFFRIM Trial pp volume 347

Similar presentations