Download presentation
Presentation is loading. Please wait.

1
Localizing Signs And Symptoms In Neurology Dr. Suhail Al-Shammri FRCP (C) Associate. Professor. Faculty of Medicine,Kuwait University

2
Language : Aphasia- language disturbance fluency, comprehension,repitition, naming,reading,writing and handedness. Dysarthria- abnormal speech articulation

3
NON-APHASIAAPHASIA

4
Fluent aphasia

5
Cranial Nerves : OLFACTORY Loss of smell: Anosmia Diminished : Hyposmia Distorted :dysosmia

6
Causes Of Anosmia Local nasal disease:cold.rhinitis,polyps Head injury: Fracture of frontal base Degenerative: Alzheimer’s disease Parkinson’s disease Endocrine: Addison’s disease, diabetes

7
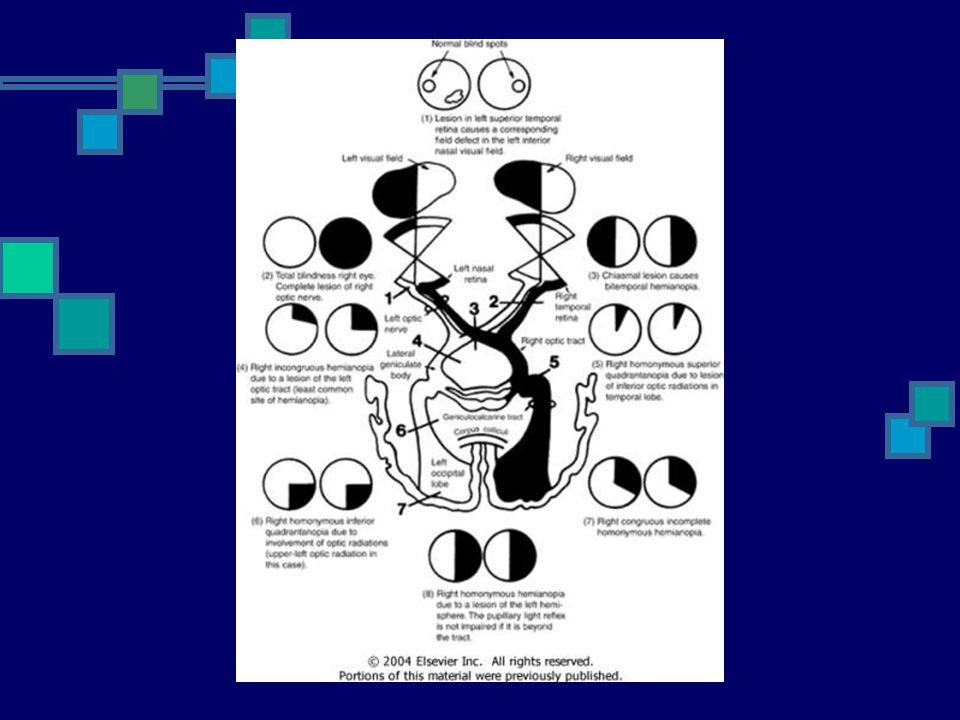
Cranial Nerve Function: optic nerve Visual acuity: reduced in : refraction error obstruction of light- catarct retinal or optic nerve disease Visual fields-confrontation hemianopia- loss of half of visual field quadrantanopia- loss of quarter

8
Visual Fields Homonymous hemianopia- loss of same half of visual field in each eye. Bitemporal hemianopia- loss of temporal fields in each eye. Perimetry- to detect small spots of visual loss(scotoma) or blind spot Extinction or neglect- perception of one stimulus on double stimulation
 or blind spot Extinction or neglect- perception of one stimulus on double stimulation.")
10
PAPILLEDEMA PATHOLOGICAL SWELLING WITH ELEVATION OF THE OPTIC DISC CAUSED BY RAISED INTRACRANIAL PRESSURE

11
Optic Nerve: Papilledema loss of venous pulsation blurring of optic disc margins venous engorgement elevation of optic disc retinal hemorrhage visual acuity usually spared Enlarged blind spot

12
PAPILLEDEMA

13
CAUSES OF PAPILLEDEMA:Increased ICP Mass lesions:tumors,abscess, hematoma Cerebral edema: trauma Infections: meningitis, encephalitis Venous sinus thrombosis Idiopathic intracranial hypertension

14
CAUSES OF PAPILLEDEMA:Medical disorders Severe anemia Accelerated hypertension Lead poisoning Polcythemia rubra vera Carbon dioxide retention Drugs: tetracyclines, steroids,excess vit A

15
OPTIC NEURITIS Acute inflammation of the optic nerve Papillitis Retrobulbar neuritis

16
Optic Nerve:Fundoscopy Papillitis- optic disc inflammation usually unilateral,painful visual acuity is impaired Causes: Demyelination: Multiple sclerosis Viral Post-infectious

17
OPTIC ATROPHY small pale sharply demarcated optic disc end-stage of various diseases visual acuity is usually impaired

18
Afferant Pupillary Defect

19
Oculomotor Nerves Eye movements controlled by six extraocular muscles: superior rectus, medial rectus,inferior rectus and inferior oblique(oculomotor) lateral rectus (abducens nerve) superior oblique (trochlear nerve) eyelid elevation,pupillary size,shape and reactivity to light and accommodation(oculomotor nerve)
 lateral rectus (abducens nerve) superior oblique (trochlear nerve) eyelid elevation,pupillary size,shape and reactivity to light and accommodation(oculomotor nerve)")
20
Nystagmus Abnormal involuntary rhythmic eye movement- at rest or induced slow deviation of one eye in one direction and quick corrective movement in opposite direction “End- point” nystagmus: occurs normally with gaze too far laterally Asymmetric horizontal nystagmus: indicate central or vestibular lesion

21
Nystagmus Up-beating or downbeating nystagmus indicates brain-stem disease. Congenital nystagmus: present at birth horizontal beating reduced or disappears on convergence usually associated with rduced visual acuity

22
NYSTAGMUS

23
Oculomotor nerve palsy Eye is down and out upper eyelid droops(ptosis) pupil is dilated, unreactive to light the concept of pupillary sparing differentiates between diabetic and compressive neuropathy.
 pupil is dilated, unreactive to light the concept of pupillary sparing differentiates between diabetic and compressive neuropathy.")
24
Oculomotor nerve palsy Nuclear: result in contralateral superior rectus palsy Fascicular: Long tract signs Weber’s syndrome: contralateral hemiplegia Benedikit’s syndrome: contralateral ataxia and intention tremor Peripheral: Partial or complete

25
Oculomotor nerve palsy: CAUSES Diabetes Compressive: Aneurysm Cavernous sinus lesions: Affect oculomotor nerves First and second divisions of trigeminal Oculosympathetic fibers

26
Cavernous sinus lesions: Causes Aneurysm Caroticocavernous fistula or thrombosis Expanding pituitary tumor Granuloma: Sarcoidosis

27
Oculomotor nerve palsy

28
Abducens nerve palsy: eye is adducted and doesn’t cross midline Nuclear lesions cause Gaze palsy CAUSES: Diabetes Atherosclerosis Multiple sclerosis Raised intracranial pressure

29
Abducens nerve palsy

30
Internuclear ophthalmoplegia Adducting eye does not move past midline and the abducting eye develops nystagmus Adduction is spared during convergence Result from lesion of the medial longitudinal fasciculus(MLF)
")
31
Internuclear ophthalmoplegia

32
Trochlear nerve palsy Vertical diplopia(double vision) especially on looking downword Head tilt toward side opposite paretic superior oblique muscle Isolated trochlear nerve palsy is often due to HEAD TRAUMA Argyll Robertson pupil-small irregular pupil costricts to light not to accommodation - neurosyphilis
 especially on looking downword Head tilt toward side opposite paretic superior oblique muscle Isolated trochlear nerve palsy is often due to HEAD TRAUMA Argyll Robertson pupil-small irregular pupil costricts to light not to accommodation - neurosyphilis")
33
Trochlear nerve palsy

34
Trigeminal Nerve Corneal Reflex: lightly touching cornea normally causes brisk bilateral eye closure. Blink will not occur on side of facial nerve paralysis. Touching cornea on the side of ophthalmic division dysfunction will not result in eye blink

35
Trigeminal Nerve Facial sensation - loss of sensation can occur independantly in each trigeminal nerve division. Muscles of mastication : atrophy of temporalis or masseter muscles. Jaw deviation toward weak side in unilateral lesions.

36
Facial Nerve Lower motor neuron palsy : produces weakness of all facial muscles including forehead on same side as lesion. Upper motor neuron palsy : Unilateral lower facial weakness sparing the ability to wrinkle forehead and partially close eyelids.

37
Horner’s Syndrome Damage to the sympathetic nerve supply to eye Characterized by : small pupil (miosis) slight drooping of eyelid (ptosis) impaired sweating (anhydrosis) on that side of the face
 slight drooping of eyelid (ptosis) impaired sweating (anhydrosis) on that side of the face")
38
Vestiulocochlear nerve Weber’s test: In sensorineural deafness sound is heard better in the normal ear. In conductive deafness sound is heard better in diseased ear. Rinne test : Air conduction is louder than bone conduction in normal individuals and in those with sensorineural deafness

39
Vestibulocochlear nerve Caloric test : unilateral vestibular stimulation is accomplished by instillation of cold or warm water into one external auditory meatus. It induces nystagmus Warm water- towards stimulated ear Cold water- away from stimulated ear

40
Glosopharyngeal and Vagus nerve Unilateral vagal nerve lesion result in palatal asymmetry with uvula deviating towards normal side. Palatal weakness results in nasal quality to voice Vocal cord weakness result in Horseness.

41
Hypoglossal Nerve Unilateral lesion : tongue deviates toward weak side. In long-standing lesion : atrophy of affected side of tongue

43
Case 3 A patient is found to have : Reduced joint position sense in the left foot. Reduced pin prick sensation on the palmar surface of the little finger of the right hand

44
Case 4 A patient is found to have : reduced joint position sense in the left foot reduced pin prick sensation on the palmar surface of the little finger of the right hand. Weakness of left ankle dorsiflexion Hperreflexia at left knee

45
Case 5 A patient found to have: reduced joint position sense in the left foot. Reduced joint position sense in the right foot. Reduced joint position sense in the left hand reduced joint position sense in the right hand

46
Case 6 A patient is found to have: reduced joint position sense in the left foot. Reduced pin prick sensation on the palmar surface of little finger of the right hand reduced visual acuity in the left eye

Similar presentations






 examination By Don Hudson, D.O., FACEP/ACOEP.>")












