Download presentation
Presentation is loading. Please wait.

1
Screening Tests for Brest & Cervical Cancer
Dr. Yeşim YASİN Spring-2014

2
Outline Screening for breast cancer Screening for cervical cancer
Mammography Clinical breast exam Breast self-exam Screening for cervical cancer Pap-smear HPV DNA testing Screenings in Turkey

3
It is estimated that more than 1
It is estimated that more than 1.6 million new cases of cancer will be diagnosed in The most common cancers are prostate in men and breast in women; lung and colorectal cancers are the second and third most common cancers in both men and in women. Lung cancer is by far the most common cancer in men (28%), followed by prostate (10%), and colon & rectum (9%). In women, lung (26%), breast (14%), and colon & rectum (9%) are the leading sites of cancer death.
, followed by prostate (10%), and colon & rectum (9%). In women, lung (26%), breast (14%), and colon & rectum (9%) are the leading sites of cancer death.")
5
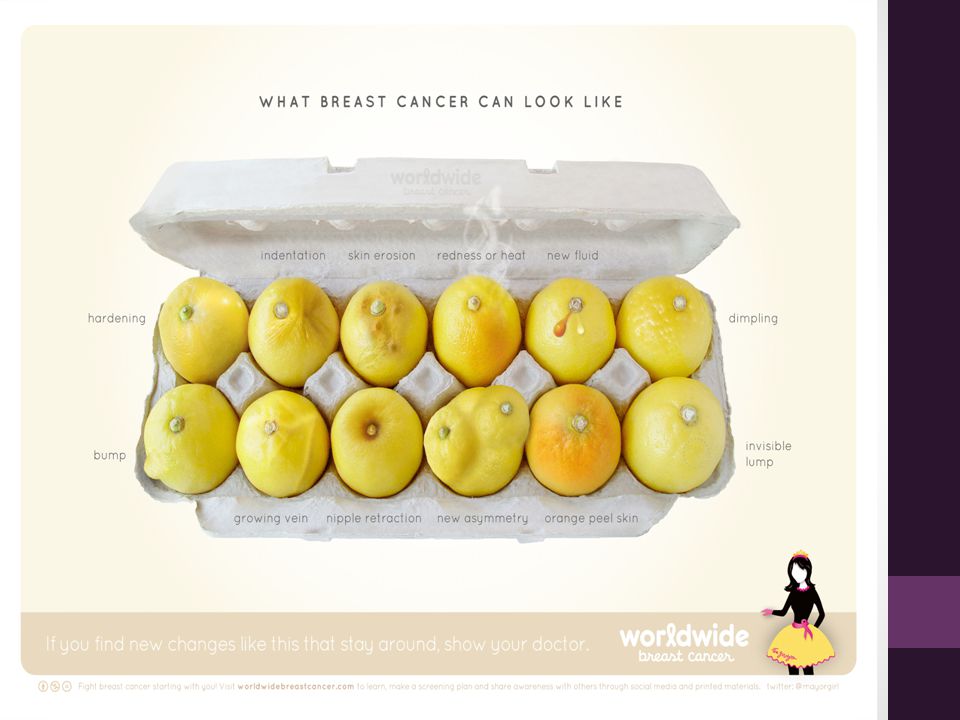
Breast cancer warning signs
Lump Skin changes Underarm swelling Veins Nipple inversion or discharge Depression of the breast Change of size of the breast A lump or thickening in or near the breast or under the arm A change in the way the skin of the breast, areola, or nipple looks or feels, for example: inversion or retraction of the nipple, swelling or distortion of the skin, a thickened area of skin on the breast, or scaling or erosion of the nipple. Strange pain in the breast with no lump Nipple discharge or nipple tenderness; the nipple may also be inverted, or pulled back into the breast Ridges or pitting of the breast; the skin may look like the skin of an orange

7
95% of Breast Cancer begins in the breast ducts

8
Most common screening tests
Mammography Clinical breast exam Breast self-exam

9
Mammography-1 Compression aided radiologic study
Screenings vs Diagnostic which should yield a final assessment and recommendation Obese women are more likely to have false positives and need additional views

11
Mammography-2 7 statistical models
Mammography reduces the rate of death from breast cancer by 7%-23% with a median of 15%1. 1. Berry DA, et al. N Eng J Med. 2005:353: Mammography is the primary screening tool for cancer. Findings from seven independent statistical models of breast cancer incidence and mortality showed that mammography screening as practiced in the United States reduced the rate of death from breast cancer by 7% to 23%, with a median of 15%.1 1. Berry DA, et al. N Eng J Med. 2005:353:

12
Age and interval for mammography
Regular screening lowers breast cancer mortality by 15%-20% in women aged 40-49 25%-30% in women aged 50-69 Limited evidence for effectiveness in women aged 70+ Interval Optimal interval unknown Reductions in mortality have occurred at intervals ranging from months Many organizations recommend annual screening for women aged 40-49 Health organizations sometimes differ in their recommendations for the age to begin screening and for how often the screenings should be done. The effectiveness of mammographic screening among women aged 40 to 49 is less than in older women, although it is still significant.1 Evidence for the effectiveness of mammography screening in women older than 70 is limited, but recent research has led the American Cancer Society to recommend that all women aged 40 and older receive annual mammograms for as long as they are in good health and would be a candidate for treatment should a cancer be found.2,3 The optimal interval for mammography screening is unknown. Reductions in breast cancer mortality have occurred in screening programs with intervals ranging from 12 to 33 months.1 Because breast cancers tend to grow more rapidly in premenopausal women and because the sensitivity of breast cancer screening is lower in this age group, many major North American health organizations recommend annual screening for women aged 40 to 49. All organizations, however, recommend yearly screening from age 50 to 70. 1. Humphrey LL, et al. Ann Intern Med. 2002;137: 2. Randolph WM, et al. Ann Intern Med. 2002;137: 3. Smith RA, Cokkinides V, Eyre HJ. CA Cancer J Clin. 2007;57:

13
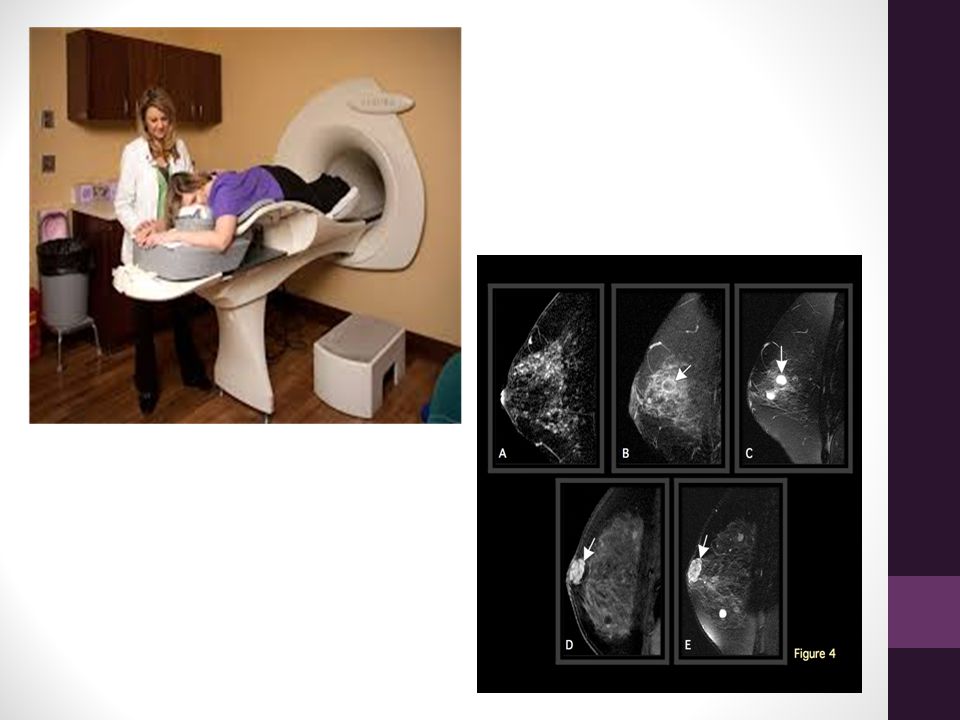
MRI Annual MRI screening recommended for women with genetic mutations for breast cancer or with other factors that put them at very high risk MRI improved staging and treatment planning, enhanced evaluation of augmented breasts and better detection of recurrences Requires contrast injection 10 cancers per 1000 women with >15% life time risk 18-38 per 1000 women suspected of BRCA mutation carriers The American Cancer Society now recommends annual screening magnetic resonance imaging (MRI) for women at very high risk for breast cancer, such as those with genetic mutations for the disease.1 There is little evidence to support the use of ultrasound for screening asymptomatic women.2 1. American Cancer Society. CA Cancer J Clin. 2007;57:75-89. 2. Irwig L, Houssami N, van Vliet C. Brit J Cancer. 2004;90:
 for women at very high risk for breast cancer, such as those with genetic mutations for the disease.1. There is little evidence to support the use of ultrasound for screening asymptomatic women American Cancer Society. CA Cancer J Clin. 2007;57: Irwig L, Houssami N, van Vliet C. Brit J Cancer. 2004;90:")
15
Breast Ultrasound (US)
Effectiveness not yet demonstrated High risk women are 2 to 3 times more likely to have a cancer seen only on US Used primarily to Evaluate breast abnormalities identified through clinical breast examination or mammography Guide breast biopsies and Fine Needle Aspiration (FNA) Currently, ultrasound’s role in breast cancer detection is primarily to evaluate breast abnormalities identified through clinical breast exam or mammography, and to guide breast biopsies and fine-needle aspiration.
 Currently, ultrasound’s role in breast cancer detection is primarily to evaluate breast abnormalities identified through clinical breast exam or mammography, and to guide breast biopsies and fine-needle aspiration.")
17
Is US a good stand-alone option?
3 Studies of women with hereditary risk1: 2 of 83 cancers detected solely by annual ultrasonography 2 additional cancers detected through screenings at 6-month intervals 1. Berry DA, et al. N Eng J Med. 2005:353: If a woman cannot have a successful mammogram, ultrasound may be considered. However, ultrasound has yet to be proven as a good stand-alone option. In three studies of women with a hereditary risk of breast cancer, only 2 of 83 cancers were detected solely by annual ultrasonography. Two additional nonpalpable cancers were detected by ultrasounds performed at 6-month intervals.1 Accessible mammography remains the best screening option for all women. Robson M, Offit K. N Engl J Med. 2007;357:

18
Clinical Breast Examination
May identify 4.5%-10.7% of breast cancers that mammography misses1 Clinical proficiency impacts effectiveness Recommendations vary: American Cancer Society2 Every 3 years for average-risk women in 20s and 30s Annually for women aged 40 and above U.S Preventive Services Task Force3 No recommendation/Not enough evidence When compared with current mammography technology, the clinical breast exam has been found to identify 4.5% to 10.7% of cancers that mammography misses.1 Given that more than 180,000 women are diagnosed in the United States each year, that means that the clinical breast exam may annually help identify as many as 18,000 otherwise undetected cancers. The ability to detect breast cancer by clinical breast exam appears to be related to the experience and training of the clinician performing the test. The factor most strongly associated with the clinical breast exam’s sensitivity is time spent on the exam.1 Recommendations for how often women should undergo a clinical breast evaluation vary widely. For example, the American Cancer Society recommends the exam every 3 years for average-risk women in their 20s and 30s and every year for women aged 40 and older2 whereas the U.S. Preventive Services Task Force (USPSTF) says the evidence for or against routine clinical breast exams is too insufficient to make any recommendation.3 1. McDonald S, Saslow D, Alciati MH. CA Cancer J Clin. 2004;54: 2. Smith, RA, Cokkinides V, Eyre HJ. CA Cancer J Clin. 2005;55:31-44. 3. U.S. Preventive Services Task Force. Screening for Breast Cancer: Recommendations and Rationale
 says the evidence for or against routine clinical breast exams is too insufficient to make any recommendation McDonald S, Saslow D, Alciati MH. CA Cancer J Clin. 2004;54: Smith, RA, Cokkinides V, Eyre HJ. CA Cancer J Clin. 2005;55: U.S. Preventive Services Task Force. Screening for Breast Cancer: Recommendations and Rationale")
19
Breast Self-Exam Not shown to have an affect on breast cancer mortality rate1. US Preventive Services Task Force: Not enough evidence to recommend for or against it2. ACS and others: Teach women the procedure and give them the option of using it3. As a “stand-alone” procedure, the breast self-exam has not been shown to be an effective screening tool. A Cochrane review of two large population-based trials conducted in Russia and Shanghai found that breast self-exam did not reduce breast cancer mortality, but did increase the number of diagnosed benign breast lesions.1 The Cochrane reviewers concluded that breast self-examination does not appear to reduce breast cancer deaths.1 The U.S. Preventive Services Task Force has also concluded that there is not enough evidence to recommend for or against breast self-exam.2 The American Cancer Society and other health organizations, however, continue to recommend that women be taught the procedure and offered the option of using it.3 Kosters JP, Gotzsche PC. Cochrane Database of Systematic Reviews. 2003;2: CD 2. U.S. Preventive Services Task Force. Screening for Breast Cancer: Recommendations and Rationale 3. Smith, RA, Cokkinides V, Eyre HJ. CA Cancer J Clin. 2005;55:31-44.

21
Cervical Screening

22
Why cervical screening?
Regular screening reduces the risk of developing cervical cancer Cervical screening can prevent about 80 – 90% of cervical cancers developing Due to cervical screening, incidence of cervical cancer dropped drastically in many parts of the world.

23
Cervical carcinogenesis
What are the possibilities once a woman is infected with a high risk HPV type? It has been shown that between 60-75% of young women are infected with HPV. We know that the majority of women have only transient infection and do not go on to develop persistent infection. However, during the time of transient infection women may develop mild cytological abnormalities. It is felt to be only those with persistent infection that go on to develop precancerous lesions such as CIN 2 and 3 or invasive cervical cancer. Wright et al. NEJM 2003

24
Epidemiology of cervical cancer
Over 99% of cervical cancers have HPV DNA detected within the tumor 70% of cervical cancer is caused by one of two types of HPV, 16 or 18 The quadrivalent HPV vaccine protects against Types 6, 11, 16 and 18 It is generally accepted that HPV infection may be detectable only transiently. However, it is still not clear whether genital HPV infections are entirely eliminated by the host or merely become suppressed at a level below detection, through an immune response. Progression from HPV infection to invasive cervical cancer is estimated to take years or longer. Cervical cancer is an uncommon consequence of HPV infection. Nevertheless, regular screening for cancer with pap smears can detect cervical abnormalities that can be treated before they become cancerous. Screening helps detect pre-cancerous abnormalities/cancer at a stage where it can be “cured” in over 90% of people.

25
What is cervical screening?
It is NOT a test for cancer It aims to detect possible abnormalities in cells on the cervix which may develop into cancer in years to come if not treated The test is either HPV (HPV DNA) test or “pap-smear” test
 test or pap-smear test.")
26
Special conditions Following conditions should be reported:
Bleeding between periods Offensive vaginal discharge Pelvic pain

27
Performing Pap-smear A vaginal speculum is used to view the cervix
One method involves brushing the cervix with a spatula and broom, and then smearing what is collected on a slide The second involves collecting a specimen with the spatula and broom, and then putting it into a container of fluid that can be plated onto a slide.

28
Not routinely needed group:
Women aged under 20 years Women aged 65 years or over Women who have had a total hysterectomy Women who are pregnant Women who have had radiotherapy to the cervix

29
Test results-1 Most results are normal this means that no abnormal cells were found at that time If the sample is not good enough the result is insufficient, and the smear must be repeated The smear should not be repeated within 6 weeks of the last test If abnormal cells are found it is very unlikely that it is cancer

30
Test results-2 Mild abnormalities often go back to normal on their own – the smear needs to be repeated in six months time More significant changes such as moderate or severe abnormalities will need further investigation (colposcopy) and sometimes treatment Almost all abnormalities detected should be treated
 and sometimes treatment. Almost all abnormalities detected should be treated.")
31
Pap-smear terms Cervical Dysplasia Abnormal cell changes
Precancerous cell changes CIN (Cervical Intraepithelial Neoplasia) SIL (Squamous Intraepithelial Lesions) “Warts” on the cervix All of these terms mean similar things-simply that abnormalities were found. Most of the time, these cell changes are due to HPV. Many of these types of HPV can cause cervical dysplasia, or abnormal cell changes. Just because a female has cervical dysplasia, it does not mean she will get cervical cancer, it means she has precancerous changes to the cells of the cervix. Dysplasia is generally referred to as mild, moderate and severe. Mild dysplasia is the most common and probably is not a true precancerous disease. Mild dysplasia generally represents a tissue response to the virus. Up to 70% of women with mild dysplasia will have the cells return to normal without any treatment. Moderate and severe dysplasia are usually treated because of their higher rates of developing into cancer. Usually the health care provider will want to monitor the cervix closely. Some health care providers will take a more aggressive stance and will want to treat any type of dysplasia. Others may be open to discussing options and/or closely monitoring the cervix with more frequent pap smears before making decisions about when to treat and what treatment option(s) should be considered.
 SIL (Squamous Intraepithelial Lesions) Warts on the cervix. All of these terms mean similar things-simply that abnormalities were found. Most of the time, these cell changes are due to HPV. Many of these types of HPV can cause cervical dysplasia, or abnormal cell changes. Just because a female has cervical dysplasia, it does not mean she will get cervical cancer, it means she has precancerous changes to the cells of the cervix. Dysplasia is generally referred to as mild, moderate and severe. Mild dysplasia is the most common and probably is not a true precancerous disease. Mild dysplasia generally represents a tissue response to the virus. Up to 70% of women with mild dysplasia will have the cells return to normal without any treatment. Moderate and severe dysplasia are usually treated because of their higher rates of developing into cancer. Usually the health care provider will want to monitor the cervix closely. Some health care providers will take a more aggressive stance and will want to treat any type of dysplasia. Others may be open to discussing options and/or closely monitoring the cervix with more frequent pap smears before making decisions about when to treat and what treatment option(s) should be considered.")
32
How accurate is pap-smear?
Cervical screening is not 100% accurate Having a smear test every three years reduces the risk of developing cervical cancer by % It is important to report any abnormal symptoms, such as bleeding or discharge

33
Abnormal pap tests What is usually recommended? Re-testing
Treat with antibiotics HPV-DNA testing Colposcopy Biopsy If your Pap test is” borderline abnormal”, or considered to be of “undetermined significance” (ASCUS), Women with abnormal Pap smear results are usually examined further for cervical problems. You may be advised to take some medication to help clear up a possible infection. The health care provider may just want you to re-test in 1-3 months. You may be advised to have a colposcopy and biopsy. A colposcopy is a procedure in which the vagina and the surface of the uterine cervix is examined through a lighted microscope (colposcope) for signs of cervical abnormalities or cancer. It requires special training to be able to perform the test. It is recommended for women with high-grade lesions (HSIL) and carcinoma results in a Pap smear, and may also be offered to women who have atypical glandular or squamous cell results; it is recommended to be offered to those with ASC-US pap smears AND positive HPV DNA tests. Often they remove any abnormal cells at the same time with cryotherapy, laser surgery or electrocautery (LEEP). If the pap smear result comes back ASC-US or border-line “normal-abnormal” then an HPV-DNA test may be done in the lab to see if HPV is causing this borderline result.
, Women with abnormal Pap smear results are usually examined further for cervical problems. You may be advised to take some medication to help clear up a possible infection. The health care provider may just want you to re-test in 1-3 months. You may be advised to have a colposcopy and biopsy. A colposcopy is a procedure in which the vagina and the surface of the uterine cervix is examined through a lighted microscope (colposcope) for signs of cervical abnormalities or cancer. It requires special training to be able to perform the test. It is recommended for women with high-grade lesions (HSIL) and carcinoma results in a Pap smear, and may also be offered to women who have atypical glandular or squamous cell results; it is recommended to be offered to those with ASC-US pap smears AND positive HPV DNA tests. Often they remove any abnormal cells at the same time with cryotherapy, laser surgery or electrocautery (LEEP). If the pap smear result comes back ASC-US or border-line normal-abnormal then an HPV-DNA test may be done in the lab to see if HPV is causing this borderline result.")
34
Risk factors for cervical cancer:
Being/having been sexually active Sex at an early age Multiple sex partners Partners’ sexual history Not using condoms Smoking Weakened immune system All Related to the Human Papilloma Virus (HPV)
")
35
HPV DNA classification
Low Risk HPV Types: 6,11,40,42,43,44, 54, 61, 72, 73, 81 types 6 and 11 responsible for 95% of visible warts High-Risk HPV Types: 31,33,35,39,45, 51, 52, 56, 58, 59, 68,82 High cancer risk: 16 Most common-50% of cervical cancer High cancer risk: 18 10-12% of cervical cancer *Risk not well established yet: 26, 53, 66, 73

36
HPV DNA testing The remaining liquid from the Pap test can be tested for a number of additional things, including HPV.

37
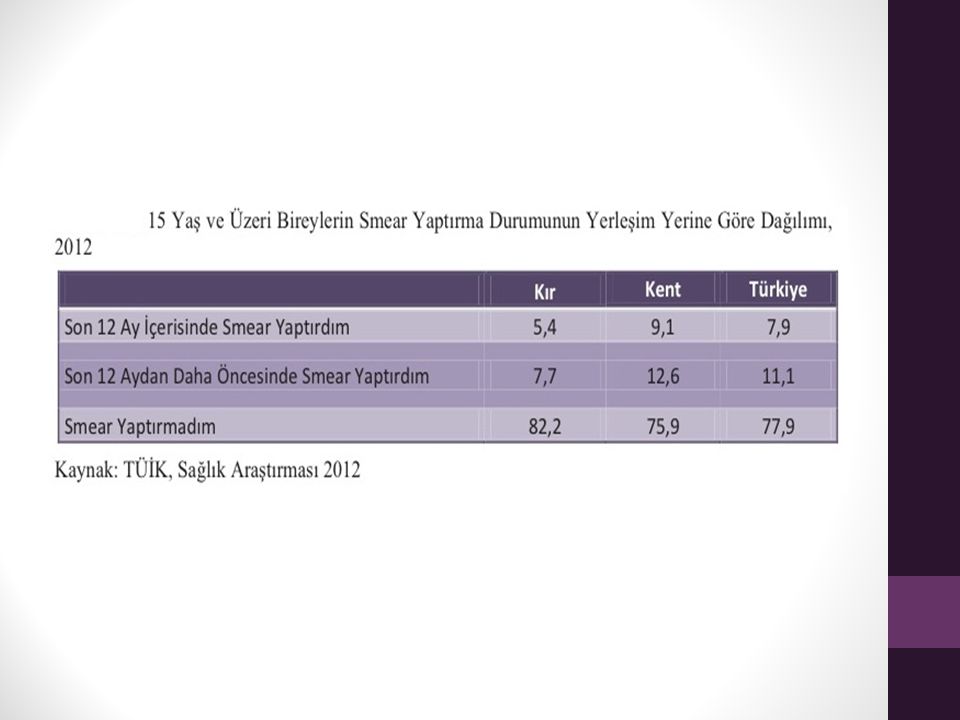
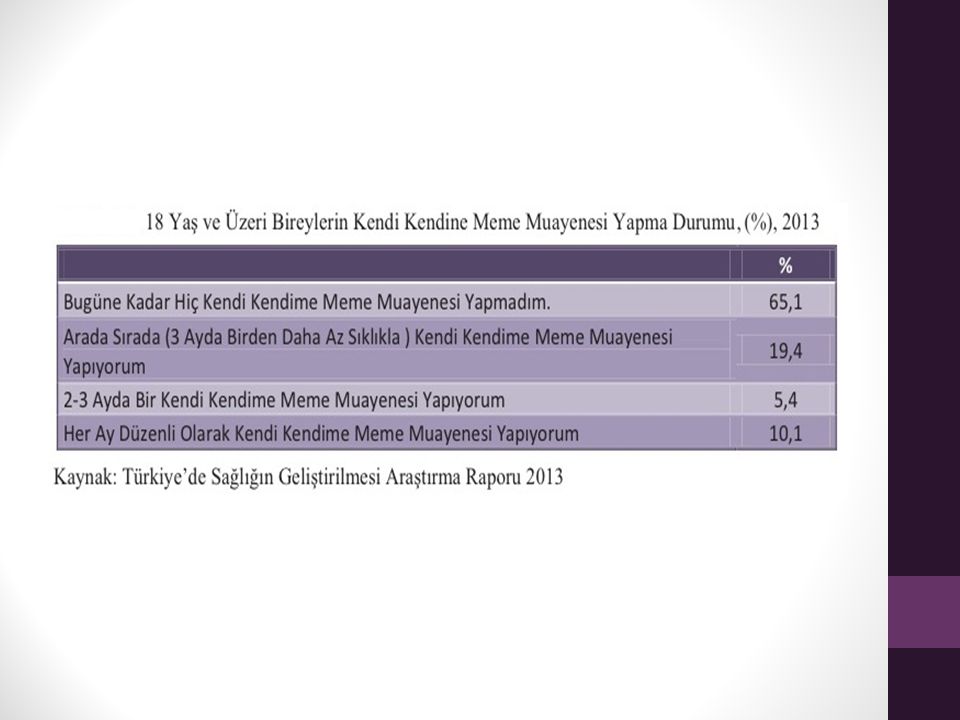
Screenings in Turkey

41
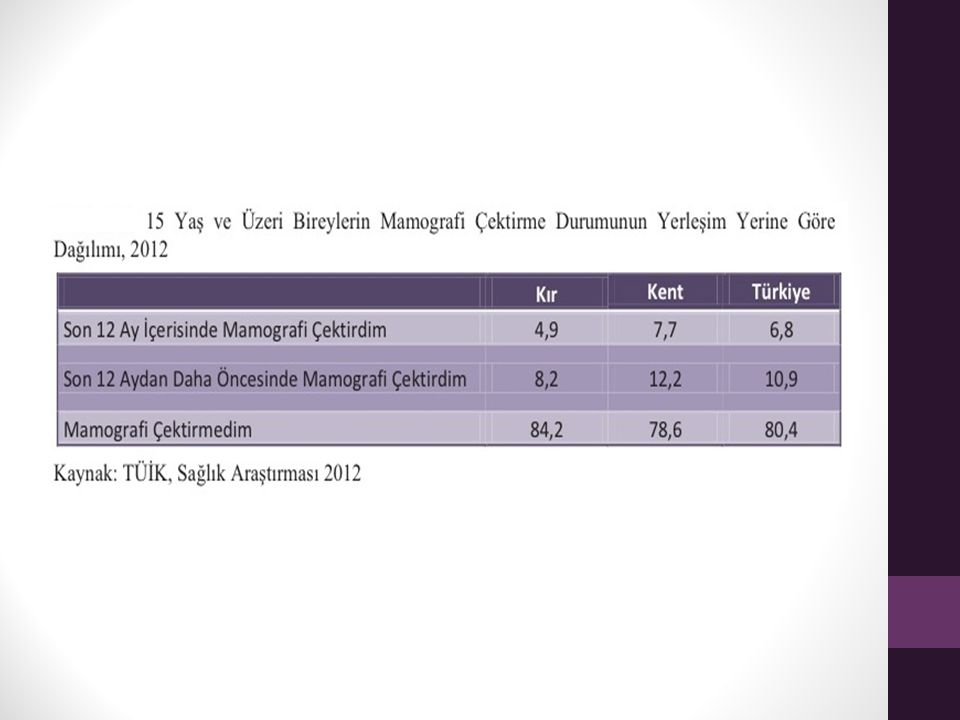
Mammography screening program in Turkey-1
Aim: To promote diagnosis at an early stage before the onset of clinical manifestations and reduce mortality due to breast cancer. Method: every 2 years; mammography (bilateral/two poses of each) + clinical breast exam + counseling on self breast exam
 + clinical breast exam + counseling on self breast exam.")
42
Mammography screening program in Turkey-2
Target population: Women at ages Organization by Family Health Centers, Community Health Centers, KETEM In case of abnormalities: Re-evaluation is needed; detailed examination and biopsy if needed.

43
Cervical screening program in Turkey-1
Aim: To promote diagnosis at an early, premalignant stage before the onset of clinical manifestations and reduce mortality due to cervical cancer. Method: every 5 years; HPV Test or Pap smear

44
Cervical screening program in Turkey-2
Target population: Women at ages (not needed in women who had hysterectomy) Organization by Family Health Centers, Community Health Centers, KETEM In case of abnormalities: Pap-smear: Re-evaluation is needed; detailed cervical examination and colposcopy if needed. HPV: Reflex cytology.
 Organization by Family Health Centers, Community Health Centers, KETEM. In case of abnormalities: Pap-smear: Re-evaluation is needed; detailed cervical examination and colposcopy if needed. HPV: Reflex cytology.")
45
THANK YOU!

Similar presentations








 Consultant Obstetrician & Gynaecologist Infertility Specialist.>")













