Download presentation
Presentation is loading. Please wait.

1
Ridge Splitting Techniques
By David R. Telles, DDS Diplomate of the American Board of Oral and Maxillofacial Surgeons

2
Introduction Not a well documented procedure
Technique useful for expansion of horizontal width deficiency Historically Indications Block Grafting vs. Ridge split Literature review

3
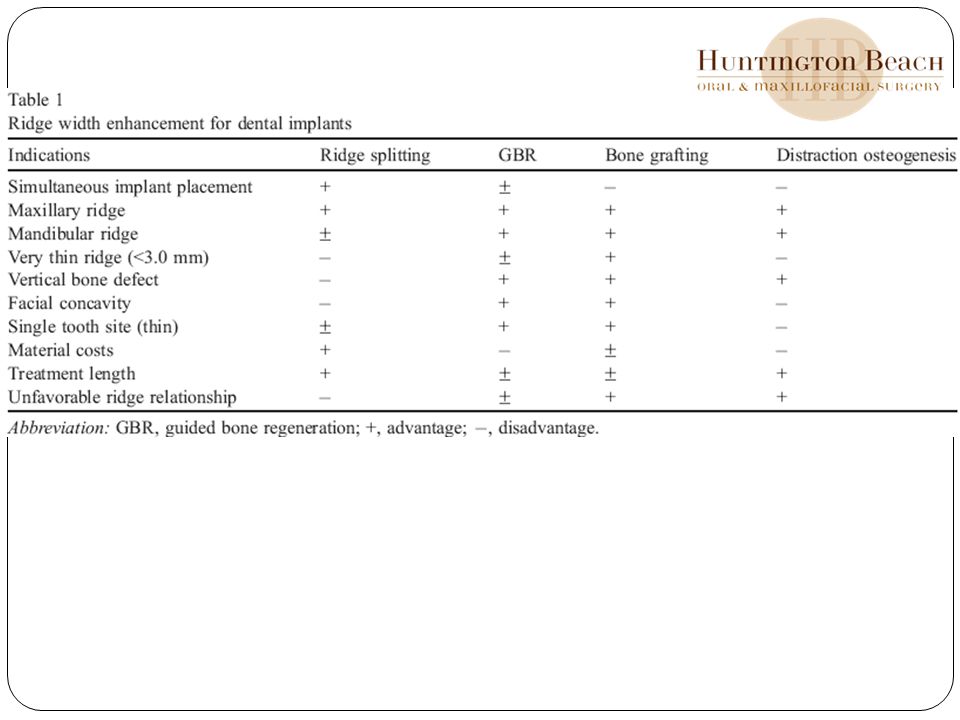
Available Techniques Bone grafting Guided bone regeneration
Distraction osteogenesis Expansion of the existing residual ridge AKA ridge splitting, bone spreading, ridge expansion, or the osteotome technique

4
Ridge Split Depends on numerous variables Clinical training
anatomic region degree of atrophy arch relationships Prosthetic goals esthetic demands Economics healing time requirements

5
Historically Ridge splitting for root-form implant placement was developed in the 1970s by Dr. Hilt Tatum Tatum developed specific instruments including tapered channel formers and D-shaped osteotomes to expand the resorbed residual ridge Designed an implant system (Omni R system, St. Petersburg, Florida) for this technique that was tapped into place with a mallet. Summers later revived the interest in this technique developed round implant osteotomes suitable for use with commercially available cylinder root-form implant systems reported that in 143 maxillary implants placed using the osteotome technique, only 5 failed Scipioni et al published their experience with the edentulous ridge expansion technique 329 implants in 170 patients with narrowed residual ridges Following a 4 to 5 month healing period and 3 to 5 months of provisional loading, the implants were restored 98.8% implant survival over 5 years.
 for this technique that was tapped into place with a mallet. Summers later revived the interest in this technique. developed round implant osteotomes suitable for use with commercially available cylinder root-form implant systems. reported that in 143 maxillary implants placed using the osteotome technique, only 5 failed. Scipioni et al published their experience with the edentulous ridge expansion technique. 329 implants in 170 patients with narrowed residual ridges. Following a 4 to 5 month healing period and 3 to 5 months of provisional loading, the implants were restored. 98.8% implant survival over 5 years.")
6
Historically Sethi and Kaus evaluated the ridge expansion technique in thin maxillary ridges with adequate height and two cortical plates separated by a cancellous layer of bone placed 449 implants at the time of expansion in 150 patients 97% implant survival rate after a 5-year observation period Clinical studies have shown that surgeons may achieve predictable results in managing the narrow edentulous ridge with ridge splitting techniques treatment has become an integral part of implant surgical therapy

7
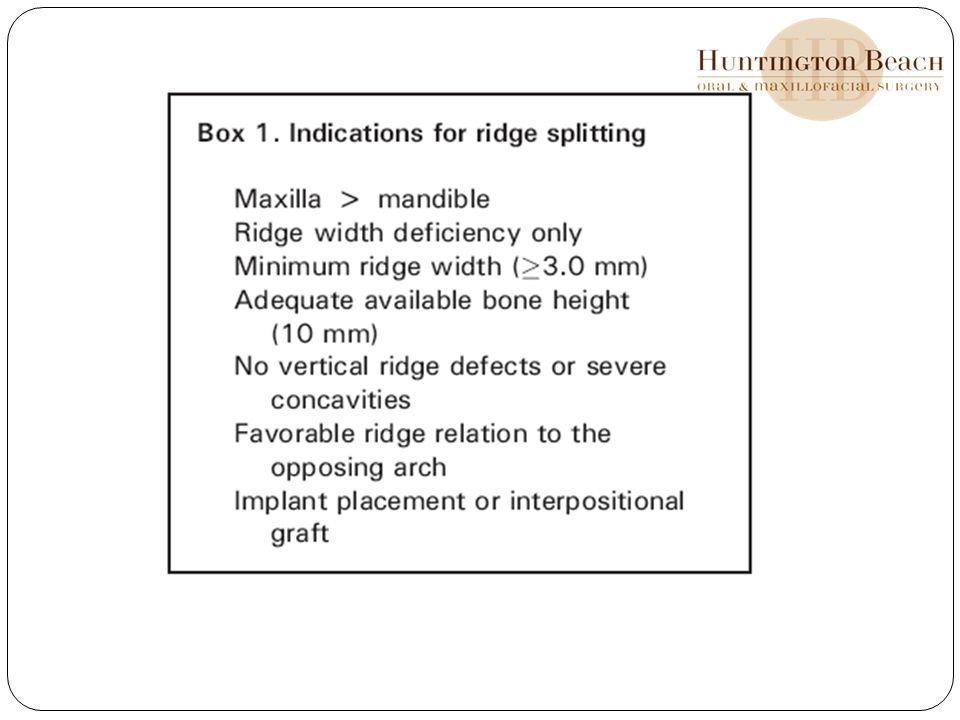
Indications used to expand the edentulous ridge for implant placement or insertion of an interpositional bone graft only suitable for enhancing ridge width – must be adequate done height – no vertical bony defect can be present minimum ridge width of 3.0 mm is preferred Splitting ridges narrower than this is technique sensitive and can result in bone fractures and resorption Very Difficult to expand narrow ridges in single tooth sites – these cases better augmented with graft Avoid ridge splitting when facial bone concavities are present

8
Indications More applicable to the maxilla than the mandible
Thinner cortical plates and softer medullary bone make maxillary ridge splits more predictable In some cases narrow posterior mandible may be split E.g. long edentulous span Abundant bone height superior to the mandibular canal (> 12 mm) Presence of some cancellous bone between the dense outer cortical plates If these conditions are not met may be best to consider onlay augmentation Bone quality dictates outcome
 Presence of some cancellous bone between the dense outer cortical plates. If these conditions are not met may be best to consider onlay augmentation. Bone quality dictates outcome.")
11
Following tooth loss…. thin buccal cortex of the maxillary alveolus resorbs to a greater degree than the thicker palatal socket wall resorption results in a decrease in bone width and more medial position of the residual ridge narrower ridge in the anterior maxilla and premolar areas is often inadequate for placement of standard-diameter dental implants (4.0 mm) When Ridge splitting considered– do not compromise on the desired implant diameter simply for implant placement Goal = expand the ridge to allow placement of the appropriate size implant for proper prosthetic / biomechanical support
 When Ridge splitting considered– do not compromise on the desired implant diameter simply for implant placement. Goal = expand the ridge to allow placement of the appropriate size implant for proper prosthetic / biomechanical support.")
12
Considerations Interocclusal space
r/o unfavorable crown-to-implant ratios Ridge splitting doesn’t correct ridge discrepancies If significant medial resorption has occurred – causing an unfavorable ridge relationship – consider only grafting When implants are placed following ridge splitting – angulation is typically more facial compared to the axis of natural teeth Due to greater remodeling and resoprtion of the facial cortical plate following extraction Restoring these may require angle abutments – communicate to GP

13
Advantage over Grafting
Ridge splitting may allow for immediate implant placement Unlike guided bone regeneration, which relies on bone forming over the exposed implant surface, ridge splitting repositions the cortical plates around the implant. Bone then regenerates within the space between the expanded cortical plates Diminished treatment length Cost for implant treatment is decreased No bone grafting or barrier membranes required DisAdv: If complications arise and bone loss occurs – pt may be left with an even more greater bone defect

14
Evaluation / Technique
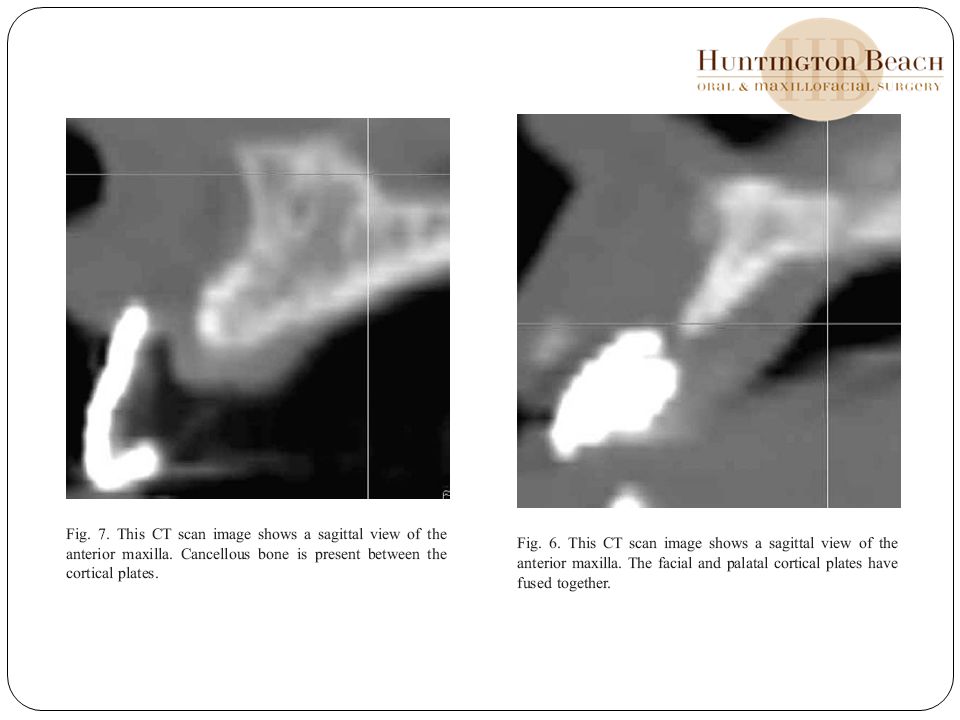
Periapical Eval Panorex --- help to determine bone height CT scan – Use of a radiographic stent can guide placement and give information regarding ridge deficiency Helps to determine actual ridge width and deficiencies Determine if cortices have fused Palpation / Ridge mapping – to determine the depth/thickness of soft tissue Soft tissue considerations – adequate attached gingiva Study models – interocclusal distance

16
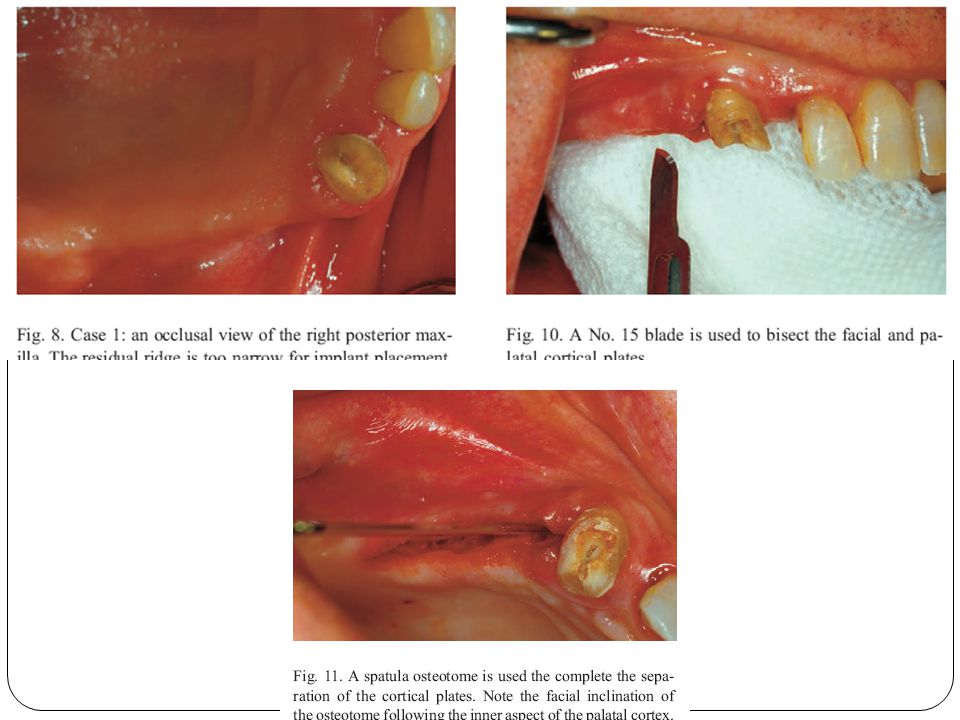
Technique Minimal mucoperiosteal flap reflection is performed to expose only the ridge crest periosteum along the lateral cortices should remain intact to ensure blood supply to the underlying bone Evaluate the ridge width and determine whether the bone dimensions and anatomy are suitable for ridge splitting If necessary, the peak of the thin ridge may be slightly reduced with a ronguer or osteoplasty bur round-handled scalpel with a No. 15 or round-tip Beaver blade is used to begin the osteotomy osteotomy should bisect the ridge and separate the cortical plates A mallet is used to advance the scalpel blade through the bone Hold blade parallel to the palatal or lingual cortex – will often result in a more facial angulation Remove blade with a back and forth motion parallel to the cut This crestal bone cut can be within 1 mm of the adjacent tooth The ridge split should be performed well beyond the planned implant sites in an edentulous span

17
Technique After the crestal osteotomy is completed, thin chisels, osteotomes, tapered fissure burs, or saws are used to further separate the cortices and begin the ridge expansion In dense bone, a thin, tapered fissure bur or a saw blade is often preferred to complete the bony cut Gradually, wider chisels or osteotomes are used to gently expand the ridge If bone expansion is difficult, then vertical osteotomies may be made through the facial cortex at each end of the crestal osteotomy Implant site preparation can be accomplished using round, tapered implant osteotomes or implant drills Slowly place implant to allow for expansion Some ppl perfer to place particulate bone graft around the implants and between separated cortices – usually unnecessary Follwing implant placement – split thickness facial flap developed leaving the periosteum in tact – will allow for advancement of the flap for primary closure Wait 3-6 months to allow for adequate implant / bony healing

19
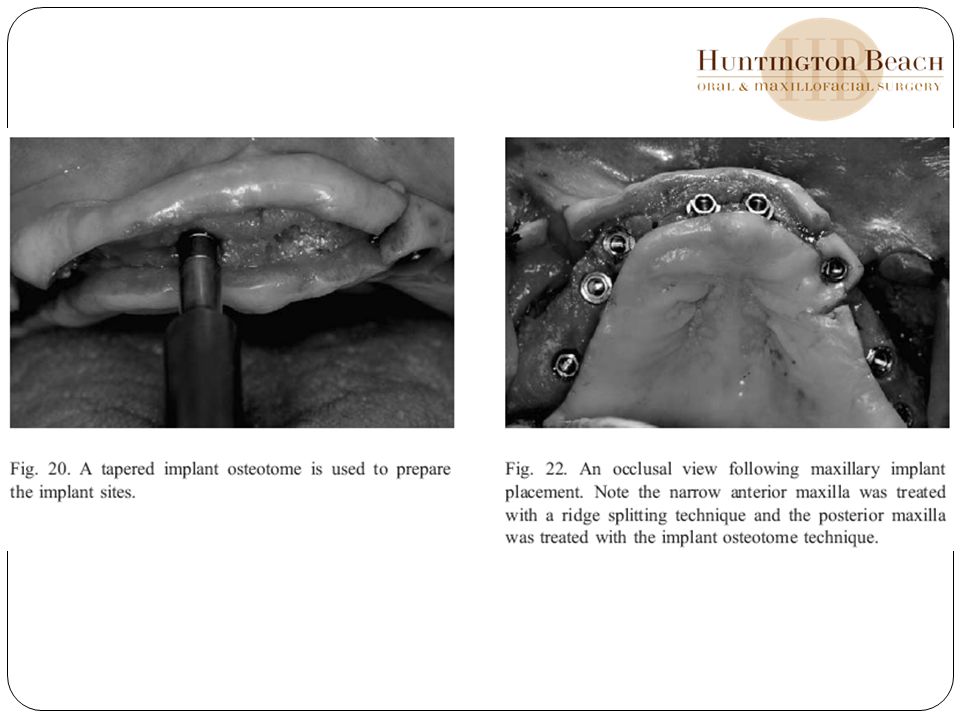
Technique - osteotome When greater ridge width is present and minimal gains required – implant osteotome technique may be considered Useful in anterior and posterior maxilla OR indicated when ridge width is adequate but clinician wants to place wider diameter implant (>4.5 mm) for improved emergence profile or biomechanical
 for improved emergence profile or biomechanical.")
20
Technique -- osteotome
A small, round bur is used to penetrate the crestal bone slightly palatal to the center of the ridge. implant osteotomy is started with a small-diameter drill (1.5–2.0 mm) shank of the drill is angulated slightly facially to follow the palatal cortical bone palatal cortex is more difficult to expand help prevent apical perforation of the tip through the facial cortex A Linderman bur is also useful for the initial preparation because it is side cutting, and palatal pressure during drilling can prepare the denser palatal bone Tapered implant osteotomes in gradually greater diameters are then used to prepare the implant site Gently malleted to compress and expand the bone as opposed to removing it with a drill. force should be directed over the long axis of the osteotome w/ periodic pauses allow the viscoelastic bone to adapt to the expansion The osteotome should be rotated with a gentle pulling force to allow atraumatic removal Digital pressure on the facial plate can help support the bone during preparation and detect apical perforation of the osteotome or drill.
 shank of the drill is angulated slightly facially to follow the palatal cortical bone. palatal cortex is more difficult to expand. help prevent apical perforation of the tip through the facial cortex. A Linderman bur is also useful for the initial preparation because it is side cutting, and palatal pressure during drilling can prepare the denser palatal bone. Tapered implant osteotomes in gradually greater diameters are then used to prepare the implant site. Gently malleted to compress and expand the bone as opposed to removing it with a drill. force should be directed over the long axis of the osteotome w/ periodic pauses allow the viscoelastic bone to adapt to the expansion. The osteotome should be rotated with a gentle pulling force to allow atraumatic removal. Digital pressure on the facial plate can help support the bone during preparation and detect apical perforation of the osteotome or drill.")
21
Technique -- osteotome
A screw tap may be needed in denser bone (type II) and to prepare the thicker palatal cortex Before implant insertion, a depth gauge or periodontal probe is used to detect any perforation of the facial cortex If a fenestration or dehiscence is noted, then an incision can be made through the mucosa over the site and the tissues can be reflected to expose and repair the defect.
 and to prepare the thicker palatal cortex. Before implant insertion, a depth gauge or periodontal probe is used to detect any perforation of the facial cortex. If a fenestration or dehiscence is noted, then an incision can be made through the mucosa over the site and the tissues can be reflected to expose and repair the defect.")
23
Review Clinical experience has shown that the ridge splitting technique can be a useful method for managing the narrow residual ridge Careful preparation of the bone and maintenance of an attached periosteum are critical to the formation of new bone around the interproximal surfaces of the implants. Wound healing in these cases is similar to the fracture repair of bone

24
Review The risk of complications with ridge splitting increases when treating very thin ridges or denser inflexible cortices. Failure with this technique can result in significant bone loss If significant cortical bone fractures occur or the facial plate separates at the base, then the implant should not be placed. bone graft materials such as particulate bone or cortical struts may be inserted within the osteotomy for a staged reconstruction of the ridge fractured facial plate should be stabilized with a screw or miniplate Recommendation by Misch – sedation or GA

25
Techniques on the rise Utilization of Distraction osteogenesis techniques After the ridge split – device is inserted to control horizontal expansion Latency of 5-7 days Then the device is activated – segment is distracted 1.0 mm per day until the desired ridge width is achieved Consolidation period of 8 weeks – device removed and implants placed Healing time is less than onlay bone grafting Does not allow simultaneous implant placement

26
Summary Ridge splitting techniques are useful for managing the narrow edentulous ridge for implant placement or interpositional bone grafting Surgical approach may be used in both jaws -- best suited for the maxilla Limited to treating ridge width deficiency cortical plates of the residual ridge must be carefully split while maintaining periosteal attachment Allows simultaneous implant placement Proper patient evaluation and case selection is essential to achieving a successful surgical and prosthetic outcome

27
References Sethi A, Kaus T. Maxillary ridge expansion with simultaneous implant placement: 5-year results of an ongoing clinical study. Int J Oral Maxillofacial Implants 2000;15:491– 9. Misch CM. Ridge augmentation using mandibular ramus bone grafts for the placement of dental implants: presentation of a technique. Prac Periodont Aesth Dent 1996;8:127 – 35. Misch CM. Comparison of intraoral donor sites for onlay grafting prior to implant placement. Int J Oral Maxillofacial Implants 1997;12:767– 76. Misch CM. The use of the mandibular ramus as a donor site for onlay bone grafting. J Oral Implantol 2000;26:42 –9. Pietrokovski J, Massler M. Alveolar ridge resorption following tooth extraction. J Prosthet Dent 1975;17: 21–7. Mecall RA, Rosenfeld AL. The influence of residual ridge resorption patterns on fixture placement and tooth position in the partially edentulous patient. Part III. Presurgical assessment of ridge augmentation requirements. Int J Periodont Rest Dent 1996;16:323– 37. Misch CE. Divisions of available bone. In: Misch CE, editor. Contemporary implant dentistry. St. Louis (MO): Mosby; p. 98– 9. [11] Triplett RG, Schow SR. Summers RB. The osteotome technique: part 4—future site development. Comp Cont Ed Dent 1995;16: 1090– 9.
: Mosby; p. 98– 9. [11] Triplett RG, Schow SR. Summers RB. The osteotome technique: part 4—future site development. Comp Cont Ed Dent 1995;16: 1090– 9.")
Similar presentations





.>")













