Download presentation
Presentation is loading. Please wait.

1
Occupational Skin Diseases
Dr. Alireza Safaiean Occupationala Medicine Specialist

2
Introduction The second cause of occupational diseases ( 23-25% of all occ.diseases ) A skin disease that is caused by physical, biological or chemical factor in work Also a worsening of pre-existing skin disease can be termed as occupational skin disease

3
CAUSES OF SKIN DISORDERS
CONTACT DERMATITIS FOLLICULITIS AND ACNE PIGMENTARY DISTURBANCE NEOPLASMS, ULCERATION GRANULOMA CHEMICAL X MECHANICAL PHYSICAL BIOLOGICAL

4
Classifications of skin diseases
Occupational dermatitis Occupational photosensitivity reactions Occupational phototoxicity reaction Occupational skin cancers Occupational contact urticaria Occupational acne Occupational skin infections Occupational pigmentary disorders Miscellaneous

5
Work-aggravated Skin Diseases
Psoriasis Acne

6
APPROACH TO THE WORKER WITH SKIN DISEASE
History Physical examination Diagnostic techniques Supplemental information

7
History A. Present illness Date of onset Body site at onset
Patient description Onset – abrupt or gradual Appearance, spread Frequency Effect of treatment Course of disease Effect of weekend, vacation Work procedure change Treatment and effect on dermatitis

8
History B. Occupational information Current employer Employment dates
Job title (At time of onset, Description of job tasks, Materials contacted, Protection, Water exposure, Hand washing) Clothing/equipment: (Protective creams/cleansers, Skin cleaning, Method and frequency) Other workers affected Job since dermatitis Previous job tasks or jobs Episodes of dermatitis Second job Dates of disability Date of job changes
 Clothing/equipment: (Protective creams/cleansers, Skin cleaning, Method and frequency) Other workers affected. Job since dermatitis. Previous job tasks or jobs. Episodes of dermatitis. Second job. Dates of disability. Date of job changes.")
9
History C. Personal history
Other exposures (Animals, Foods, Plants, Clothing, Personal care products, Hobbies) Past history of skin disease (Plant dermatitis, Hand dermatitis, Psoriasis, Athlete’s foot) History of atopy Personal/family (Atopic dermatitis, Hay fever, Asthma) Medical problems Medications
 Past history of skin disease (Plant dermatitis, Hand dermatitis, Psoriasis, Athlete’s foot) History of atopy. Personal/family (Atopic dermatitis, Hay fever, Asthma) Medical problems. Medications.")
10
Physical examination Lesion type Secondary changes Distribution
Other skin disease Photographic documentation

11
Diagnostic techniques
Skin scrapings Fungus Fibers Culture Skin biopsy Patch test Contact urticaria test Photopatch test

13
Supplemental information
Material safety data sheets Medical records Workplace Other physician

14
Diagnosis Of Occupational Skin Diseases
Clinical symptoms: Are they in accordance to clinical disease? Patient history: Does skin disease relate to work? Exposure: Are there causative agents (allergens, irritants) in the work-place?
 in the work-place")
15
CAUSES OF OCCUPATIONAL SKIN DISEASE

16
Chemical agents The main cause of occupational skin diseases and disorders. These agents are divided into two types: Primary irritants: Primary or direct irritants act directly on the skin though chemical reactions. Sensitizers: may not cause immediate skin reactions, but repeated exposure can result in allergic reactions. A worker’s skin may be exposed to hazardous chemicals through: direct contact with contaminated surfaces, deposition of aerosols, immersion, splashes

17
Other Causes Physical agents such as extreme temperatures (hot or cold) and radiation (UV/solar radiation). Mechanical trauma includes friction, pressure, abrasions, lacerations and contusions (scrapes, cuts and bruises). Biological agents include parasites, microorganisms, plants and other animal materials. (Animal breeders, vets, horticulturists, bakers, tanners, bricklayers, etc. are all possible victims of biological)
. Biological agents include parasites, microorganisms, plants and other animal materials. (Animal breeders, vets, horticulturists, bakers, tanners, bricklayers, etc. are all possible victims of biological)")
18
CAUSES OF OCCUPATIONAL SKIN DISEASE
Predisposing Factors Age & experience Skin type Sweating Gender Seasons and humidity Hereditary allergy Personal hygiene Preexisting skin disease Atopy A type of inherited allergic response involving elevated immunoglobulin E . Sometimes called a reagin response, it means that you have hay fever , bronchial asthma , or skin problems like urticaria or eczema . It can also be acquired, sometimes following hepatitis or extended contact with solvents or alcohol. Atopic dermatitis Signs and symptoms of this type include itchy, thickened, scaly skin, most often in the folds of your elbows or backs of your knees. It's also common on the face, hands and feet. When this type occurs in babies, it's called infantile eczema. About 15 million Americans have atopic dermatitis.

19
Contact Dermatitis Occupational dermatitis is an inflammation of the skin causing itching, pain, redness, swelling and small blisters. Contact dermatitis is an eczematous eruption caused by external agents, which can be broadly divided into: Irritant substances that have a direct toxic effect on the skin (irritant contact dermatitis, ICD) Allergic chemicals where immune delayed hypersensitivity reactions occur (allergic contact dermatitis, ACD).
 Allergic chemicals where immune delayed hypersensitivity reactions occur (allergic contact dermatitis, ACD).")
20
Types of contact dermatitis
Irritant Contact 80% of all dermatitis is caused by direct contact with a substance It may occur randomly Allergic Contact Once sensitised, the problem is life long and any exposure to the substance will result in an attack

21
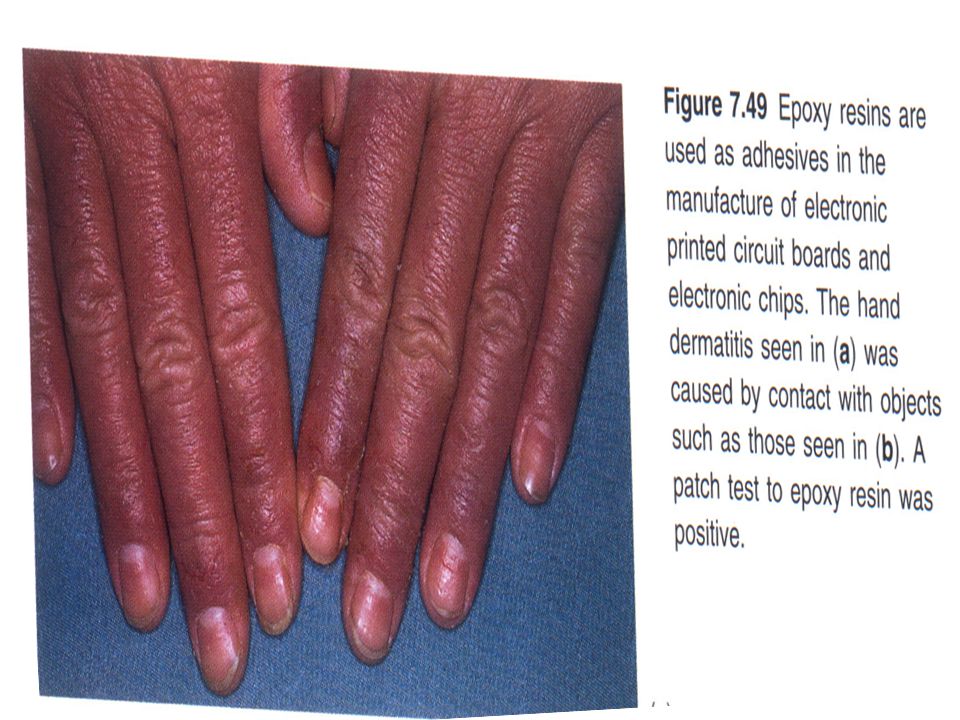
The Causes Irritants Detergents Solvents Engine oils Cutting fluid
Lubricants Fibreglass Allergens Salts Nickel Epoxy resins Dyes Rubber

22
Common site of involvement
Skin disease starts on the area of contact. Dorsal aspects of hands and fingers, volar aspects of arms, interdigital webs, medial aspect of thighs, dorsal aspects of feet.

23
Prognosis Of Occupational Dermatitis After Treatment
25% complete recovery 25% refractory 50% remitting / relapsing

24
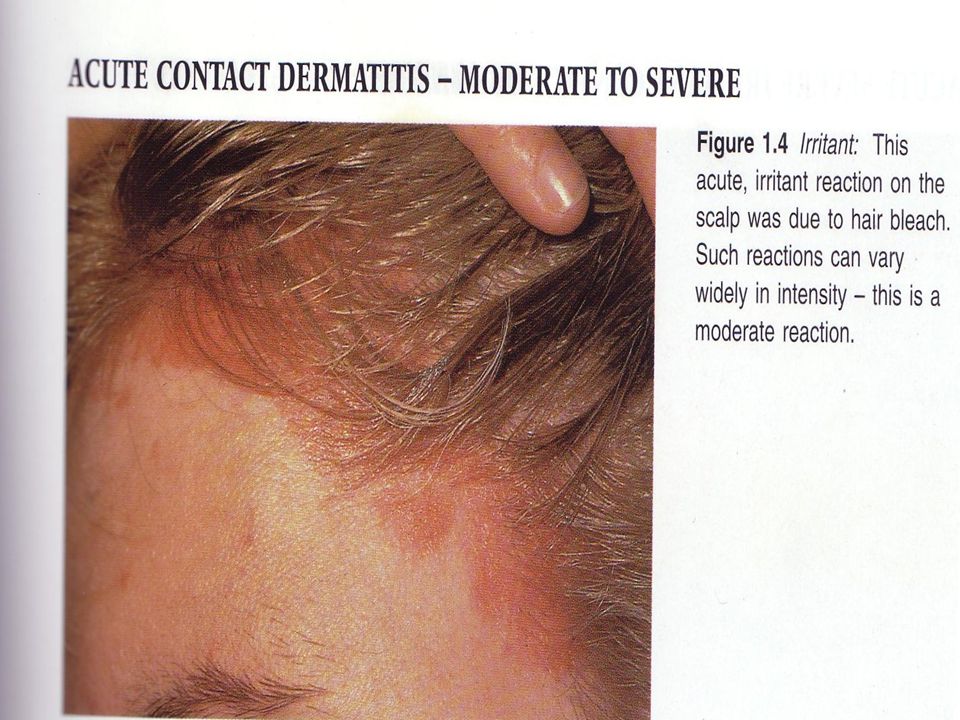
Irritant Contact Dermatitis ICD

25
Classification of ICD Acute Chronic

26
Acute ICD This is often the result of a single overwhelming exposure or a few brief exposures to strong irritants or caustic agents. Common work chemicals: – Concentrated acids (sulfuric, nitric, chromic, hydrochloric, hydrofluoric acids) – Strong alkali(CaOH,NaOH,KOH),wet concrete, sodium and potassium cyanide – Organic and inorganic salts, e.g. dichromates, arsenic salts – Solvents/gases, e.g. acrylonitrile, ethylene oxide, CS2
 – Strong alkali(CaOH,NaOH,KOH),wet concrete, sodium and potassium cyanide. – Organic and inorganic salts, e.g. dichromates, arsenic salts. – Solvents/gases, e.g. acrylonitrile, ethylene oxide, CS2.")
27
Clinical Presentation
Stinging, burning, painful, erythematous eruption occur after brief contact with strong irritant chemicals. Erosion and skin ulceration may occur. May result in permanent scar.

32
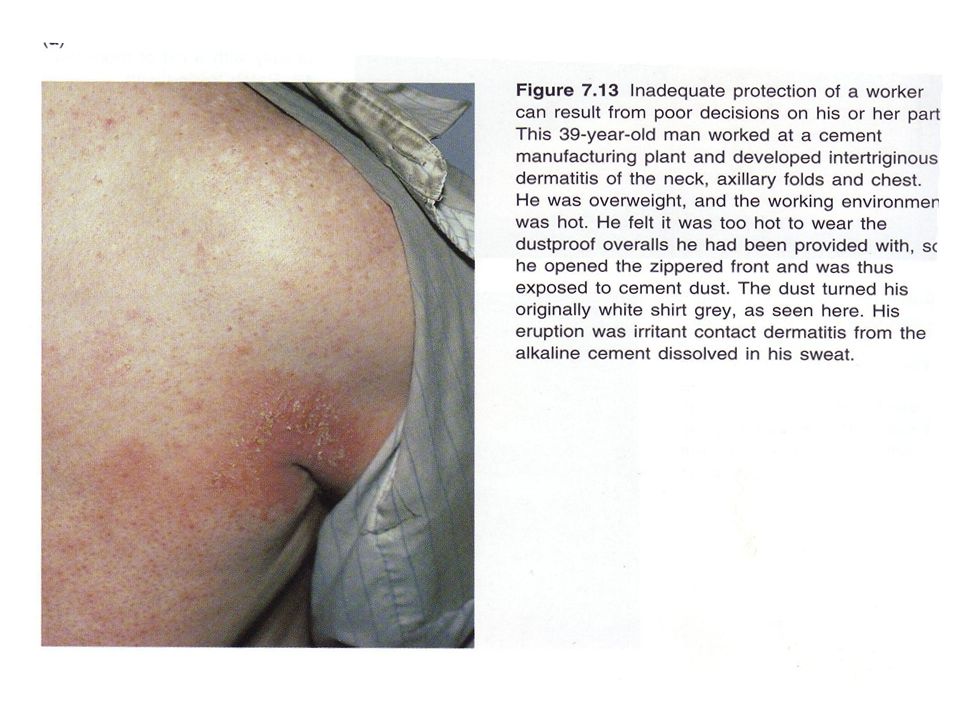
Chronic (cumulative) ICD
Repetitive exposure to weaker irritants -Wet : detergents, organic solvents, soaps, weak acids, and alkalis -Dry : low humidity air, heat ,dusts , and powders Disease of the stratum corneum Is due to a stepwise progression of damage to the barrier function of the skin

33
Predisposing Factors Endogenous factors: Dryness vs. wetness Sweating
Age Atopic predisposition Hx of skin diseases

34
Causes of Chronic ICD Water/wet work Fiberglass fibers Detergents
Antiseptics Disinfectants Soap/cleansing agents Weak Acids & alkali Wet cement Solvents Low humidity friction Fiberglass fibers Cutting oil Food Pesticides Plants & vegetation Rubber products Acrylic resins Soldering flux Dusts Degreasing agents

35
At risk occupations: Bartenders Caterers Cleaners Hairdressers Metalworkers Nurses Solderers Fisherman construction workers. 35% Washing 10% Solvents 6% Plastics and adhesives 6% Foodstuff 5% Dirty, wet work 5% Mineral oils

36
Clinical Presentations
Usually presents with dry, scaly fissuring, lichenified and eczematous lesions on the fingers and hands. Vesicular lesions do occur but are less common than in ACD. May in face ( forehead, eyelids, ears, neck) and arms due to airborne irritant dusts and volatile irritant chemicals
 and arms due to airborne irritant dusts and volatile irritant chemicals.")
40
Management In workplace Treating the active case
Removal from exposure in active lesion Skin cleansing (water rinse without soap if possible) Barrier cream Gloves Treating the active case Topical corticosteroids Soap substitutes Emollients (either water- or oil-based) Second line (for steroid resistant cases): Topical PUVA Azathioprine Cyclosporin
 Barrier cream. Gloves. Treating the active case. Topical corticosteroids. Soap substitutes. Emollients (either water- or oil-based) Second line (for steroid resistant cases): Topical PUVA. Azathioprine. Cyclosporin.")
42
Allergic Contact Dermatitis ACD

43
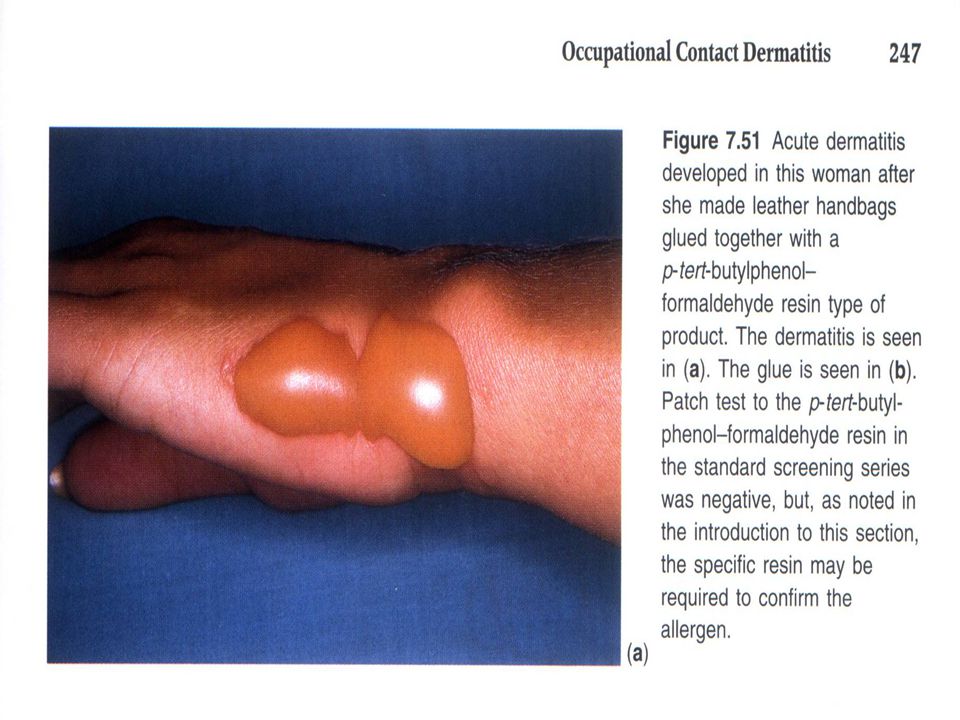
Allergic Contact Dermatitis
Caused by low-molecular weight haptens Hapten is “incomplete allergen” Binds to carrier protein for immunogenicity Low molecule weight enables penetration of hapten Hapten penetrates through stratum corneum of a sensitized individual A classical Type IV reaction

44
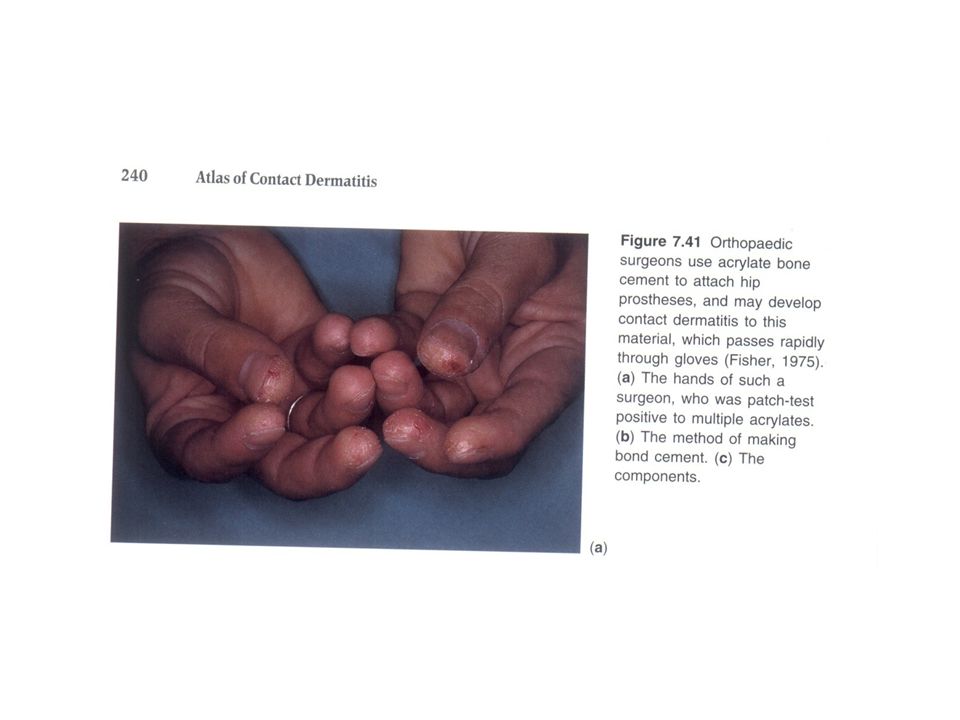
Occupational Skin Allergens
Poison oak/ivy Metals: Chromium Nickel Gold Mercury Cobalt Rubber industry Accelerators Antioxidants Plastic resins Epoxy resins PU resins Phenolic resins Formaldehyde resins Acrylic resins Rosin ( colophony ) Soft soldering Organic dyes ( azo dyes ) Methyl metacrylate Plants Latex and its powder Germicides and biocides e.g. lanolin Some pesticides Some solvents Formaldehyde Turpentine Aliphatic amines Nitrates Ethylene oxide
 Soft soldering. Organic dyes ( azo dyes ) Methyl metacrylate. Plants. Latex and its powder. Germicides and biocides. e.g. lanolin. Some pesticides. Some solvents. Formaldehyde. Turpentine. Aliphatic amines. Nitrates. Ethylene oxide.")
45
Classification of ACD Acute chronic

46
Clinical Features ( Acute Form )
Rash appears in areas exposed to the sensitizing agent, usually asymmetric or unilat. Sensitizing agent on the hands or clothes is often transferred to other body parts. The rash is characterized by erythema, vesicles and sever edema. Pruritus is the overriding symp.

47
Acute Allergic Contact Dermatitis
Showing Erythema, Edema, and Vesiculobullae

54
Clinical Features ( Chronic Form )
Thickened , fissured, lichenified skin with scaling The most common sites: Dorsal aspect of hands Eyelids periorbital

55
Subacute Eczema Showing Erythema, Oozing, Crusting, Lichenification, and Scale

56
Chronic Eczema: Showing Lichenification, Fissuring, and Scale

63
Diagnosis Complete history Physical examination Patch test
Occupational Non-occupational Physical examination Patch test

65
Patch Test Confirm delayed hypersensitivity Material& technique:
Medium Adhesive Marking of the test Occlusion for 48 h Read in after h

66
Angry back

67
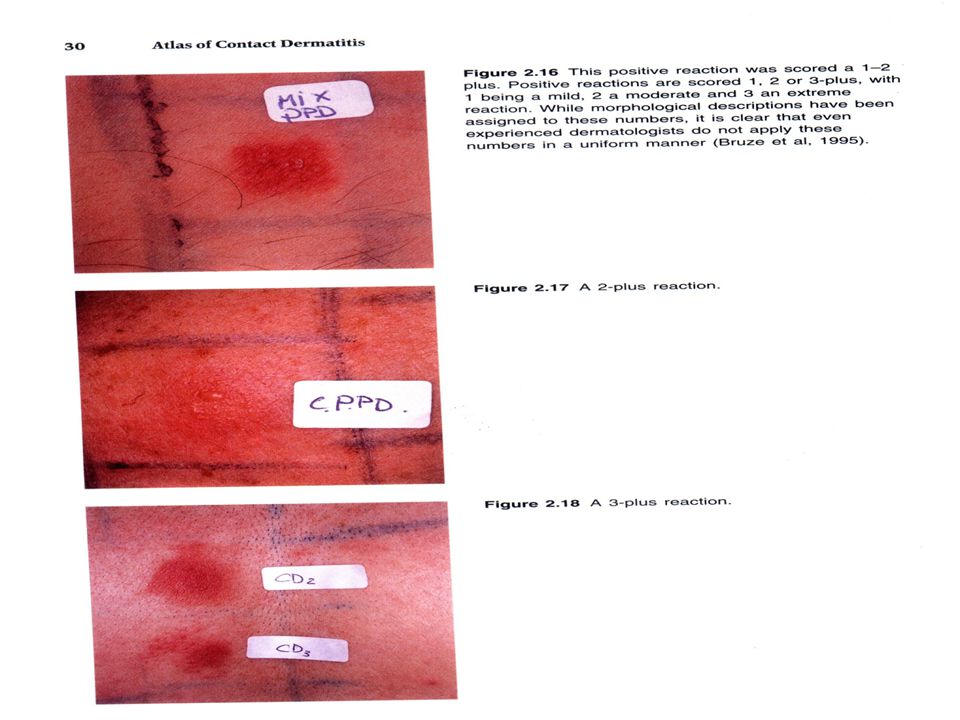
Interpretation of patch test result
Nothing: negative reaction Erythema, papules, infiltration, no vesicle: weak reaction Erythema, vesicular eruption, edema: strong reaction Bulla, ulceration: extreme reaction Erythema to eczematous: irritant reaction

68
Weak positive reaction (+)
Doubtful reaction (?) Faint macular or homogeneous Erythema, no infiltration Weak positive reaction (+) Erythema , Infiltration Discrete papules
 Faint macular or homogeneous Erythema, no infiltration. Weak positive reaction. (+) Erythema , Infiltration Discrete papules.")
69
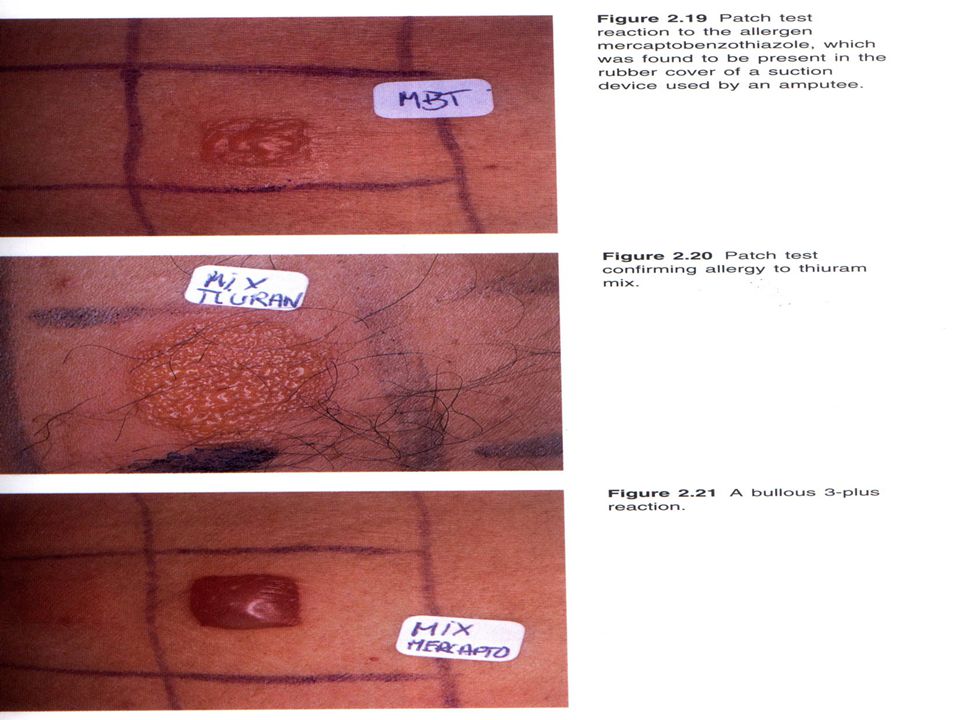
Strong positive reaction
(++) Erythema Infiltration Papules Discrete vesicles Extreme positive reaction (+++ ) Coalescing vesicles/bullous reaction
 Erythema Infiltration Papules Discrete vesicles. Extreme positive reaction. (+++ ) Coalescing vesicles/bullous reaction.")
70
Interpretation codes (Ladou 2004)
")
73
Management & Prevention
Removal from exposure ( lifelong) Drug treatment Topical steroid Emollients Prevention Like ICDs
 Drug treatment. Topical steroid. Emollients. Prevention. Like ICDs.")
75
Irritant versus Allergic dermatitis
Hx. Of contact with known irritant Acute onset Stinging, Burning Neg. patch test Localized Many people Improved with long vacation (3 weeks) ACD Hx. Of contact with known allergen Delay onset (1-3d) Itching, Vesicle Positive patch test Spreads Few people May improved even on weekends
 ACD. Hx. Of contact with known allergen. Delay onset (1-3d) Itching, Vesicle. Positive patch test. Spreads. Few people. May improved even on weekends.")
76
Criteria to Determine Occupational Causation
1. The clinical appearance is consistent with contact dermatitis. 2. There are workplace exposures to potential cutaneous irritants or allergens. 3. The anatomic distribution of dermatitis is consistent with cutaneous exposure in relation to the job task. 4. The temporal relationship between exposure and onset is consistent with contact dermatitis. 5. Non-occupational exposures are excluded as probable causes. 6. The dermatitis improves if work exposure to the suspected irritant or allergen ceases. 7. Patch or provocation tests identify a probable causal agent. If four of the seven statements in Table are true, the eczema is probably occupational in origin.

77
Contact photodermatitis
Some chemicals may cause CD only in the presence of light Sunlight or artificial light sources that emit specific wavelengths 2 categories: -phototoxic -photoallergic

78
Phototoxic Photoallergic Antifungal agents Fragrances
Halogenated salicylanilide Phenothiazines Sunscreens Whiteners Agricultural Coal-tar derivative Dyes (Eosin) Drug -phenothiazines -sulfonamides Plants&derivative -psoralen -lemon
 Drug. -phenothiazines. -sulfonamides. Plants&derivative. -psoralen. -lemon.")
79
Clinical course Phototoxcic:
- painful , exaggerated sunburn that may develop bullae and pigmentation -by avoiding the agent, dermatitis usually disappears promptly Photoallergic: - many of the features of ACD ( itching , vesiculation)
")
80
Where involved ? Exposed areas: face, ant. V of the neck, back of the hand, uncovered sites on the arm&leg Hairy areas, upper eyelids, and below the chin may be spared

81
Diagnoses Distribution (on sun-exposed surfaces) of the reaction
Photopatch test

82
treatment Avoidance of contact Other are the same as CD

83
Contact Urticaria Immunologic :
Caused by proteins that act as allergens Proteins penetrate through skin⇝bind to IgE on the surface of mast cell⇝ release of histamine and other mediators (type-1 reaction) Sometimes generalized reactions occur Latex allergy
 Sometimes generalized reactions occur. Latex allergy.")
84
Contact Urticaria Nonimmunologic: Caused by chemicals
Direct pharmacologic action on skin cells No sensitization necessary More common than suspected

85
Occupational Causes Latex allergy ( m/c ) Formaldehyde Food industry
Plants Vegetables Animal products Pharmaceutical industry Streptomycin

86
Clinical Features Of Contact Urticaria
Hives (edema) appear on sites of contact within minutes The hives disappear within 1-4 hours Mild: Only itching Severe: Systemic symptoms (anaphylaxis)
 appear on sites of contact within minutes. The hives disappear within 1-4 hours. Mild: Only itching. Severe: Systemic symptoms (anaphylaxis)")
88
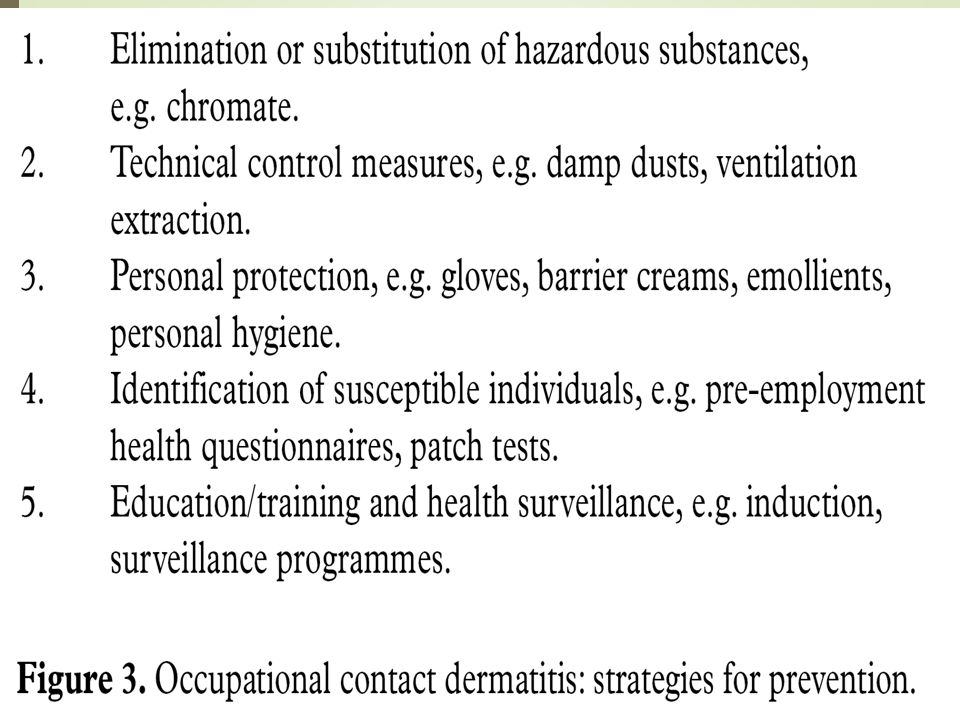
Management & Prevention
Removal from exposure Treatment of active disease Preventive measures

89
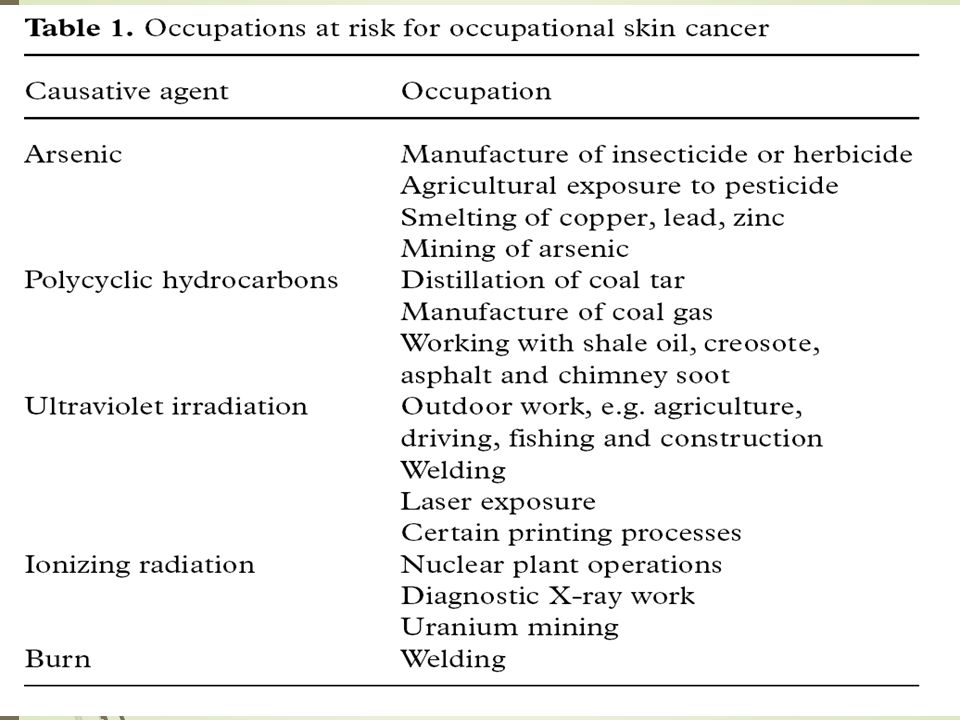
Occupational Skin Cancers
The second m/c form of occupational skin diseases About 17% of all cases of occupational skin diseases

90
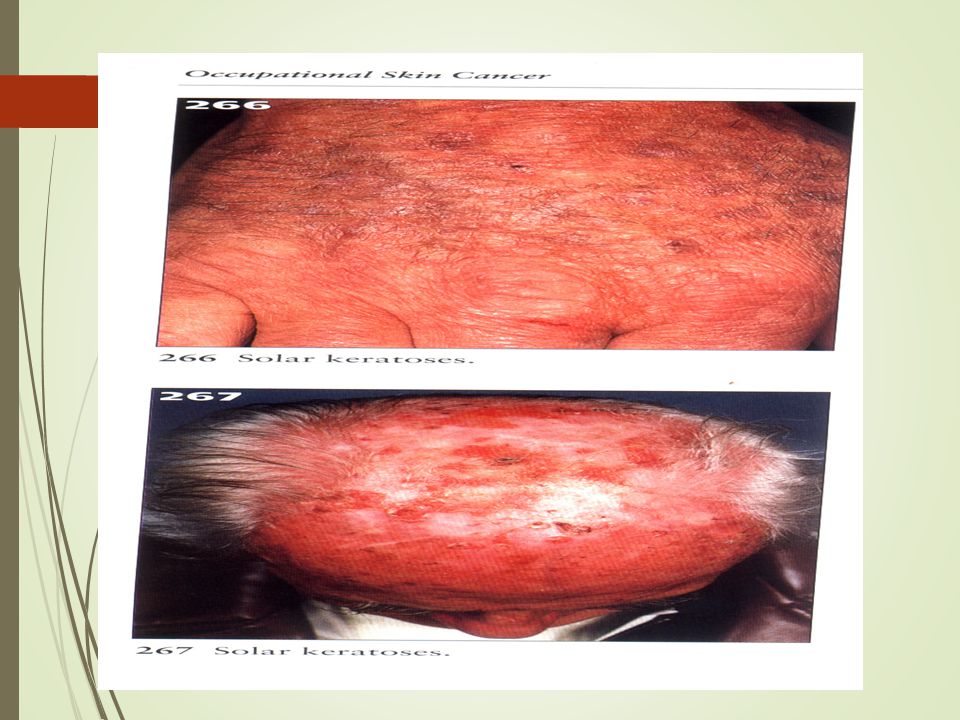
What Cancers? Actinic (solar) keratoses Basal cell carcinoma
Malignant lesions: Basal cell carcinoma Squamous cell carcinoma Malignant melanoma Pre-malignant lesions: Actinic (solar) keratoses Tar keratoses (‘warts’) Arsenical keratoses Keratoacanthoma Intra-epidermal carcinoma (Bowen’s disease) Lentigo maligna
 keratoses. Tar keratoses (‘warts’) Arsenical keratoses. Keratoacanthoma. Intra-epidermal carcinoma (Bowen’s disease) Lentigo maligna.")
96
زلال باش .... ، زلال باش .... ، فرقی نمی كند كه گودال كوچك آبی باشی ، یا دریای بیكران ، زلال كه باشی ، آسمان در توست

Similar presentations






















 Sahlgrenska academy and University Hospital 2013-03-21 Asthma,>")







>")








