Download presentation
Presentation is loading. Please wait.

1
High-Resolution Manometry & 24-hour Reflux Testing Swallowing: One Bite At A Time -or- Don ’ t Bite Off More Than You Can Chew Presented by Ron Turner, CRCP, Clinical Educator Swallowing Disorder Diagnostics ronturner57@gmail.com GuideWare™ Copyright Ron Turner, CRCP ManoScan™, ManoView ™, AccuView ™ screen captures courtesy & copyright Sierra Scientific/Given Imaging, Inc.

2
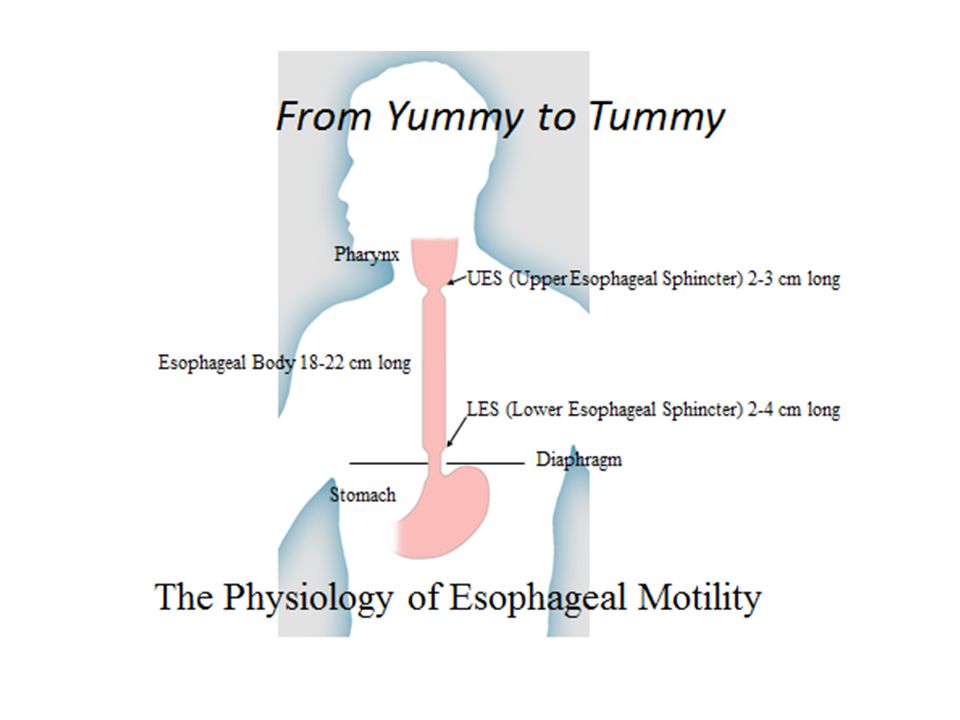
What is Esophageal Motility? The Ability of Esophageal Swallowing Pressures to Effectively Transport Swallowed Substances from the Pharynx to the Stomach

4
GI Motility online (May 2006) | doi:10.1038/gimo44 Why We Do What We Do: Endoscopic Photograph of Barrett ’ s Esophagus, the Road to Esophageal Cancer
 | doi: /gimo44 Why We Do What We Do: Endoscopic Photograph of Barrett ’ s Esophagus, the Road to Esophageal Cancer")
7
Treatment of Esophageal Motility Disorders Achalasia: Progressive Endoscopic Dilation, Botox injection, Heller Myotomy Weak and Ineffective Esophageal Motility (IEM): Bethanechol (muscle contractor) and new pro-motility meds Spasm (DES, Jackhammer Esophagus), & Hypertensive LES: Meds (calcium channel blockers, botox, nitrates, tricyclic antidepressants), progressive dilatation, esophageal wall myotomy Scleroderma: Anti-inflammatory and anti-fibrotic medications Hyptotensive LES (with qualifying GERD): Laparoscopic Fundoplication* Choice of Half (Toupet) or Full (Nissen) Anti-Reflux Wrap *Qualified by pre-surgical reflux testing and manometric assessment to determine (a) the presence of hypotensive LES residual pressure with or without hiatal hernia, and (b) the confirmation of sufficient esophageal contraction amplitudes necessary to overcome a surgically-tightened LES.
: Bethanechol (muscle contractor) and new pro-motility meds Spasm (DES, Jackhammer Esophagus), & Hypertensive LES: Meds (calcium channel blockers, botox, nitrates, tricyclic antidepressants), progressive dilatation, esophageal wall myotomy Scleroderma: Anti-inflammatory and anti-fibrotic medications Hyptotensive LES (with qualifying GERD): Laparoscopic Fundoplication* Choice of Half (Toupet) or Full (Nissen) Anti-Reflux Wrap *Qualified by pre-surgical reflux testing and manometric assessment to determine (a) the presence of hypotensive LES residual pressure with or without hiatal hernia, and (b) the confirmation of sufficient esophageal contraction amplitudes necessary to overcome a surgically-tightened LES.")
8
What is Manometry? Manometry is the measurement of PRESSURE. Just like blood pressure measures the force that blood exerts on the walls of blood vessels, esophageal manometry measures the pressures exerted by the esophageal muscles and valves in the esophagus that cause motility.

9
So, what is Esophageal Manometry? An esophageal manometry test (or an esophageal motility test) measures the pressures exerted by the esophageal muscles and valves within the esophagus during swallowing contractions. Contractions occur as pressure waves that carry the food or liquid from the throat to the stomach. This carriage of food is called motility. The pressure of the esophageal muscles and valves is the “ motor ” that drives motility. Esophageal manometry measures this motor (muscle) function, and thus, motility.
 measures the pressures exerted by the esophageal muscles and valves within the esophagus during swallowing contractions. Contractions occur as pressure waves that carry the food or liquid from the throat to the stomach. This carriage of food is called motility. The pressure of the esophageal muscles and valves is the motor that drives motility. Esophageal manometry measures this motor (muscle) function, and thus, motility..")
10
The Physics of Bolus Transit Normal esophageal bolus transit is the movement of any swallowed substance in a proximal-to-distal squeezing (peristaltic) direction within the functional swallowing anatomy that spans from the pharynx to the stomach. This normal peristaltic movement is called motility, and is caused by pressure differences, or gradients, within the esophagus. A pressure gradient is the difference in pressure between any two given physical locations at any given point in time. Normal antegrade (forward) esophageal bolus transit occurs when the pressure in any given location in the esophagus exceeds the pressure that is distal to (below) that specific location. Conversely, retrograde (backward) bolus movement occurs when the pressure in any given location in the esophagus exceeds the pressure that is proximal to (above) that specific location.
 esophageal bolus transit occurs when the pressure in any given location in the esophagus exceeds the pressure that is distal to (below) that specific location. Conversely, retrograde (backward) bolus movement occurs when the pressure in any given location in the esophagus exceeds the pressure that is proximal to (above) that specific location..")
11
The Direction of Bolus Transit In short, substances move from a location of higher pressure to a location of lower pressure. Just like squeezing a tube of toothpaste, proximal pressures that occlude the esophageal lumen must occur to create peristaltic movement distally. This is what causes the either downward or upward direction in the movement of swallowed substances within the esophagus.

12
The Mechanics of Bolus Transit For complete bolus clearance to occur in the esophagus, the squeeze pressure in the esophageal body must exceed and overcome the esophagogastric junction pressure (EGJ) (the residual pressure in the LES plus intragastric pressure), during any given swallow. When this occurs, this pressure gradient causes flow from the esophagus to pass down through the EGJ and empty into the stomach. Much like the physics of a weakened dam, when the pressure behind the dam exceeds the barrier strength of the dam, the dam breaks and the water flows. Conversely, when esophageal body pressure cannot overcome EGJ pressure, antegrade flow through the LES cannot occur. If the dam is stronger than the pressure of the water, the water stays behind the dam. Even patients with a poor relaxing LES or a hypertensive LES will have effective swallows as long as the esophageal body pressures are sufficient to overcome the EGJ barrier pressure during the swallow.

13
Effective Bolus Transit Means Effective Swallowing Again, effective swallowing is a simple function of esophageal pressure gradients between proximal and distal locations, not merely the physical state of the LES. And although the overall EGJ barrier pressure of the LES includes the external pressure from the physical diaphragm pressing upon the LES, effective bolus clearance is still fundamentally accomplished when this overall combined LES/diaphragmatic barrier pressure is overcome by higher distal esophageal pressure. Bottom line: The effectiveness and direction of any given swallow is primarily determined by the esophageal and EGJ pressure gradients that exists during that swallow.

14
Comparing Conventional Manometry with High-Resolution Manometry Conventional Solid-State Catheter: 4 Pressure Channels, Spaced 5 cm Apart

15
Conventional Esophageal Manometry: 40-minutes, 30+ swallows, 13 catheter repositionings Four sensors spaced at 5 cm intervals; the distal sensor is positioned in the LES with 4 radial sensors evenly spaced at 90-degrees at that same level; the other three unidirectional sensors are thus positioned in the esophagus, spanning a non-contiguous 15 cm above the LES LES

16
Conventional Manometry Is Difficult to Standardize: Measures 4 Pressures Only, and Cannot Measure the Flow of Swallowed Liquid (1) The catheter has only 4 measuring sensors and must be repeatedly repositioned in an attempt to chase the constantly moving swallowing anatomy during the 45-minute study. (2) This sensor is supposed to be inside the lower valve, but this drop in pressure is very often simply due to the valve moving off the sensor, but it is impossible to know for sure because the sensors do not span the entire swallowing anatomy. 2 1
 This sensor is supposed to be inside the lower valve, but this drop in pressure is very often simply due to the valve moving off the sensor, but it is impossible to know for sure because the sensors do not span the entire swallowing anatomy")
17
High-Resolution Impedance Manometry (HRMZ) Catheter: 36 Pressure Sensors (432 circumferential pressures) Spaced 1 cm Apart + 18 Impedance Channels (which display the transit of swallowed liquid)
 Catheter: 36 Pressure Sensors (432 circumferential pressures) Spaced 1 cm Apart + 18 Impedance Channels (which display the transit of swallowed liquid)")
18
UES LES HRMZ is 100% standardized because the circumferential pressure-impedance catheter simultaneously spans the entire swallowing anatomy from pharynx to stomach to simultaneously assess & calculate uninterrupted 360-degree circumferential motor function & bolus transit of the entire swallowing anatomy. The catheter NEVER has to be repositioned because it captures ALL real-time anatomical movement of the UES, esophagus, and LES. At the Same Time, All the Time

19
The Combined Visualization and Measurement of the Real-Time Pressures (Muscle Function) & Resulting Transport of Swallowed Liquids (Bolus Transit) of the Entire Swallowing Anatomy, from Pharynx to Stomach It is literally THE LIVING ESOPHAGUS™ displayed as a real-time, full-color movie, using blue-to-red (cold-to-hot) color to identify pressure and magenta color to identify bolus presence and transit What is High-Resolution Pressure/Impedance Manometry?
 & Resulting Transport of Swallowed Liquids (Bolus Transit) of the Entire Swallowing Anatomy, from Pharynx to Stomach It is literally THE LIVING ESOPHAGUS™ displayed as a real-time, full-color movie, using blue-to-red (cold-to-hot) color to identify pressure and magenta color to identify bolus presence and transit What is High-Resolution Pressure/Impedance Manometry")
20
The Basics of High-Resolution Manometry: Hot in Daytona Beach, Cold in Tampa Hot= High Pressure Cold= Low Pressure Hot Cold

21
The Key to High-Resolution Manometry (HRM) is PATTERN RECOGNITION: The average esophagus is 18-22 cm long. The HRM catheter (1) spans the entire swallowing anatomy, from pharynx to stomach, with 36 cm of uninterrupted circumferential measurement. As the anatomy tightens and loosens its grip on the catheter during swallowing, these low-to-high pressure changes are reflected as cool-to-hot color changes. Pharynx UES Esophagus LES Stomach 1
 spans the entire swallowing anatomy, from pharynx to stomach, with 36 cm of uninterrupted circumferential measurement. As the anatomy tightens and loosens its grip on the catheter during swallowing, these low-to-high pressure changes are reflected as cool-to-hot color changes. Pharynx UES Esophagus LES Stomach 1.")
Similar presentations





 Clase 3: Fisiopatología Esofágica Dr. Michel Baró Aliste.>")



, FACS, FCCP Consultant & Asst. Professor of Cardiothoracic Surgery Consultant.>")






, FRACP. SHAKESPEARE SPECIALIST GROUP MILFORD, AUCKLAND.>")




