Download presentation
Presentation is loading. Please wait.

1
RETAINED PLACENTA Dr Mona Shroff

2
Definition Failure of placental delivery within 30 minutes after delivery of the fetus. Dr Mona Shroff

3
Causes Morbid Adherence of the placenta Uterine Abnormality
Placenta Acreta Placenta Increta Placenta Percreta Uterine Abnormality Constriction Ring - reforming cervix Full bladder Dr Mona Shroff

4
Management Inform Anaesthetist
If the placenta is undelivered after 30 minutes consider: Emptying bladder Breastfeeding or nipple stimulation Change of position - encourage an upright position If bleeding: immediately Inform Anaesthetist Insertion of large bore IV (18g) cannula Insert urinary catheter Commence/continue oxytocin infusion 20 units in 1 litre / rate – 60drops per min Measure and accurately record blood loss Prepare and transfer patient to theatre for manual removal of placenta (MROP) Dr Mona Shroff
 cannula. Insert urinary catheter. Commence/continue oxytocin infusion 20 units in 1 litre / rate – 60drops per min. Measure and accurately record blood loss. Prepare and transfer patient to theatre for manual removal of placenta (MROP) Dr Mona Shroff")
5
Introducing one hand into the vagina along cord
Dr Mona Shroff

6
Supporting the fundus while detaching the placenta

7
Withdrawing the hand from the uterus

8
POST-PROCEDURE CARE Observe the woman closely until the effect of IV sedation has worn off. Monitor the vital signs (pulse, blood pressure, respiration) every 30 minutes for the next 6 hours or until stable. Palpate the uterine fundus to ensure that the uterus remains contracted. Check for excessive lochia. Continue infusion of IV fluids. Transfuse as necessary. Dr Mona Shroff
 every 30 minutes for the next 6 hours or until stable. Palpate the uterine fundus to ensure that the uterus remains contracted. Check for excessive lochia. Continue infusion of IV fluids. Transfuse as necessary. Dr Mona Shroff")
9
Complications of Retained Placenta
Shock Postpartum haemorrhage Puerperal Sepsis Subinvolution Hysterectomy Dr Mona Shroff

10
Umbilical vein injection for management of retained placenta
Umbilical vein injection of saline solution plus oxytocin appears to be effective in the management of retained placenta. Saline solution alone does not appear be more effective than expectant management. The difficulties in implementing this intervention are related to the training of personnel in the technique of giving injections into the umbilical vein. The WHO Reproductive Health Library, No 8, Oxford, 2005. The Cochrane Database of Systematic Reviews 2006 Issue 4 Dr Mona Shroff

12
largely as a result of the increase in the number of cesarean sections
The incidence of placenta accreta has increased 10-fold in the past 50 years, to a current frequency of 1 per 2,500 deliveries. largely as a result of the increase in the number of cesarean sections Dr Mona Shroff

13
Risk factors Risk factors for placenta accreta include :
placenta previa with or without previous uterine surgery. previous myomectomy. previous cesarean delivery. Asherman's syndrome. submucous leiomyomata. maternal age of 36 years and older. The ACOG committee Dr Mona Shroff

14
Prenatal risk probability
Because of the fact that many of these cases become evident only at the first attempt to separate the placenta at delivery, it is essential to attempt to identify antenatally both placenta accreta and its attendant risk factors, the most common of which is concurrent placenta previa & previous CS. Dr Mona Shroff

15
Gray-scale sonographic signs of placenta accreta
normal placenta characterized by a hypoechoic boundary between the placenta and the urinary bladder that represents the myometrium and normal retroplacental myometrial vasculature. The normal placenta has a homogenous appearance as well. Dr Mona Shroff

17
Gray-scale sonographic signs of placenta accreta
Loss of the retroplacental hypoechoic zone Progressive thinning of the retroplacental hypoechoic zone Presence of multiple placental lakes ("Swiss cheese" appearance) Thinning of the uterine serosa-bladder wall complex (percreta) Elevation of tissue beyond the uterine serosa (percreta) Dr Mona Shroff
 Thinning of the uterine serosa-bladder wall complex (percreta) Elevation of tissue beyond the uterine serosa (percreta) Dr Mona Shroff")
18
Color Doppler signs suggestive of placenta accreta
Dilated vascular channels with diffuse lacunar flow. Irregular vascular lakes with focal lacunar flow. Hypervascularity linking placenta to bladder. Dilated vascular channels with pulsatile venous flow over cervix. Dr Mona Shroff

19
Multiple layers of newly formed vessel
Newly formed vessel & multiple placental lakes Dr Mona Shroff

20
Sensitivity Specificity GRAY SCALE USG 94 79 COLOUR DOPPLER 82 97 MRI
100 72 Dr Mona Shroff

21
MANAGEMENT HYSTERECTOMY CONSERVATIVE
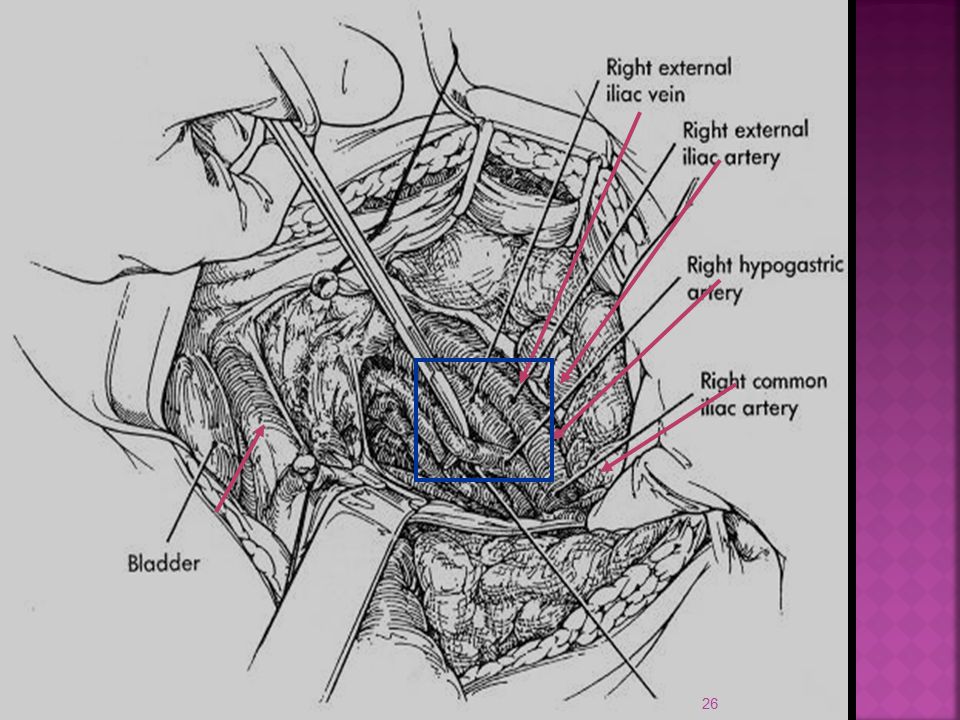
Leave placenta undisturbed +/- METHOTREXATE Uterine artery ligation UAE Internal iliac ligation Oversewing of placental bed Condom temponade B-Lynch/square sutures Argon beam coagulation Fertility desired Patient stable No bleeding Informed written consent Dr Mona Shroff

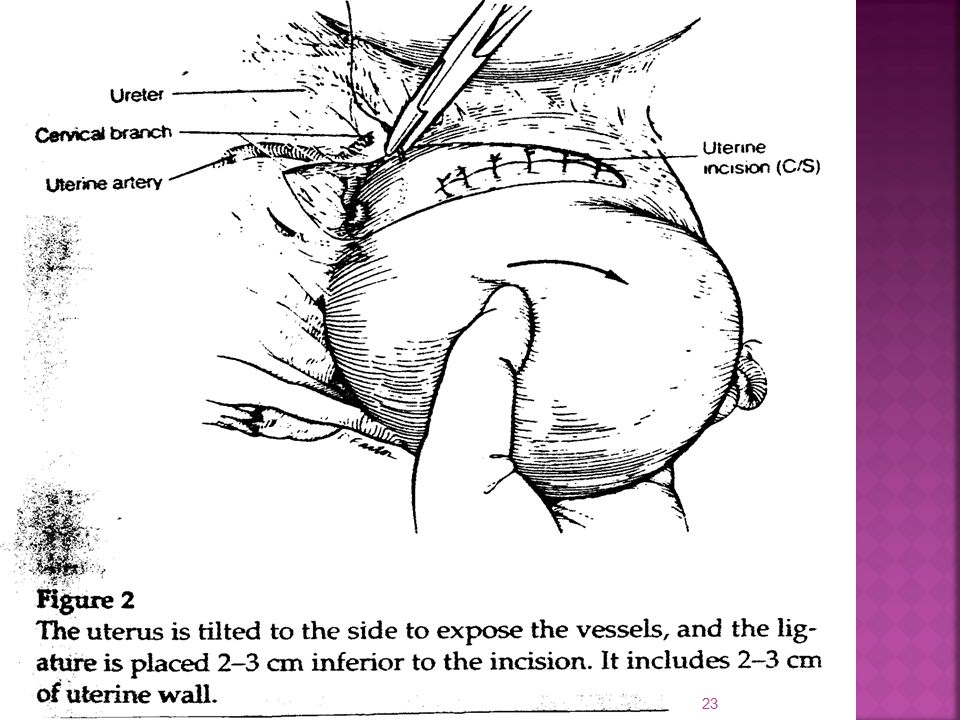
22
-Placenta Accreta - Intraoperative management
1.-Map exact position of placenta Make high transverse uterine incision to avoid cutting through placenta 2.- Deliver fetus Rapid hemostasis of uterine incision (clamps, sutures) Definitive Rx Dg uncertain Avoid TAH & Dg certain Do not remove pl UAE/Ligation UAE/ligation TAH Remove pl Leave Pl in situ Dr Mona Shroff
 Definitive Rx. Dg uncertain. Avoid TAH & Dg certain. Do not remove pl. UAE/Ligation. UAE/ligation. TAH. Remove pl. Leave Pl in situ. Dr Mona Shroff")
24
Pre/intra op EMBOLISATION

25
Haemostatic multiple square suture method

27
B-LYNCH SUTURES 2 5 1 6 3 4

28
-Placenta Accreta - Follow-up management
1.- Ultrasound /doppler :Vascularity/involution 2.- HCG titers (If plateau consider Mtx) 3. Daily Temp, Other S&S of infection 4.- Bleeding 5.- Coagulation profile Oxytocics & prophylactic antibiotics : Benefit & duration not universal Dr Mona Shroff
 3. Daily Temp, Other S&S of infection. 4.- Bleeding. 5.- Coagulation profile. Oxytocics & prophylactic antibiotics : Benefit & duration not universal. Dr Mona Shroff")
29
Follow-up OUTCOME SPONTANEOUS EXPULSION RESORPTION
INTERVAL SURGERY –placental removal If Intervention necessary for - Heavy Bleeding - Infection - DIC Proceed directly to TAH Dr Mona Shroff

30
hysterectomy Resort to hysterectomy SOONER RATHER THAN LATER (especially in cases of placenta accreta when future fertility is out of concern) Dr Mona Shroff

31
Take home message Active Mx of third stage can prevent & reduce the incidence of retained placenta. In case of risk factors,always consider placenta accreta & L/f usg/doppler features in antenatal period & plan accordingly. Dr Mona Shroff

32
THANK YOU Dr Mona Shroff

Similar presentations



: leading cause of maternal mortality worldwide Prevalence rate: 6% Africa has highest prevalence.>")


 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")














