Download presentation
Presentation is loading. Please wait.

1
ILL EFFECTS OF RADIOTHERAPY IN THE MANAGEMENT OF ORAL CANCER by Dr kashif ali Assistant professor

2
ORAL CANCER Approximately 90% of oral cancer is SCC Approximately 90% of oral cancer is SCC Particularly common in developing world Particularly common in developing world Multifactorial etiology Multifactorial etiology life style Habits and diet Others

3
Head & Neck Cancer Diagnosis

4
Squamous Cell Carcinoma 90% of all oral cancers 50% 5-year survival can occur in: tongue skin throat soft palate

5
Treatment plan is based on: anatomical considerations

6
Treatment plan is based on: Staging of disease using TNM classification Eg. T 3 N 2 M 0 laryngeal carcinoma Eg. T 3 N 2 M 0 laryngeal carcinoma

7
Treatment Options +/- OR

8
Aims of radiotherapy Radical radiotherapy - -- curative intent Radical radiotherapy - -- curative intent Palliative radiotherapy --To control symptoms Palliative radiotherapy --To control symptoms

9
Radiation Therapy External beam –most common –largest fields

10
Radiation Therapy Brachytherapy –interstitial implantation of radioisotope-filled needles

11
Radiation Therapy Au grain or Iridium Implants

12
Radiation How much? Where?

13
How much radiation? 1 “rad” = 1 centiGray (cGy) 200 cGy per day 5 days per week 1000 cGy per week
 200 cGy per day 5 days per week 1000 cGy per week")
14
How much radiation? Total dose ranges from 6000 cGy – 7000 cGy 6 – 7 WEEKS of treatment

15
ORAL CANCER TREATMENT MODALTIES Ablative Surgery Ablative Surgery Surgery and / or radiotherapy Surgery and / or radiotherapy Radiotherapy and Chemotherapy Radiotherapy and Chemotherapy

16
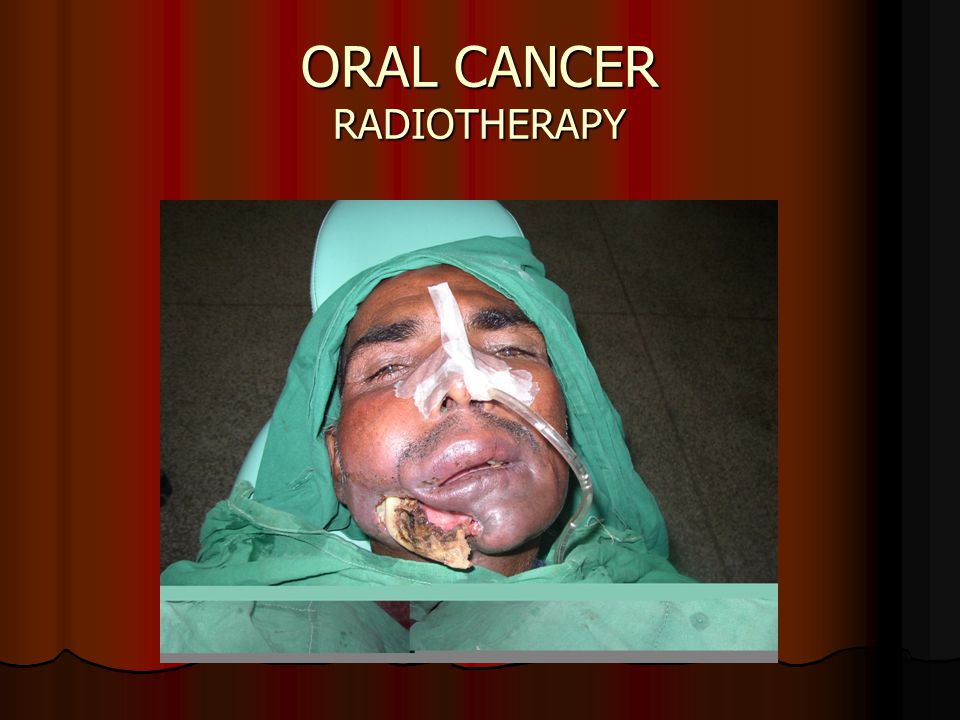
ORAL CANCER RADIOTHERAPY Advantages Normal Anatomy and function Normal Anatomy and function Is maintained Is maintained GA not needed GA not needed Can be used to debulk inaccessible lesions Can be used to debulk inaccessible lesions

17
ORAL CANCER RADIOTHERAPY Conventionally upto 60 Gys dose is given Conventionally upto 60 Gys dose is given Post radiotherapy complaints increase tremendously when the radiation dose is increased Post radiotherapy complaints increase tremendously when the radiation dose is increased

18
ORAL CANCER RADIOTHERAPY ill effects ill effects Oral mucositis Oral mucositis Xerostomia Xerostomia Loss of taste Loss of taste Osteoradionecrosis Osteoradionecrosis

19
Oral mucosa Seen in 1-2 weeks Seen in 1-2 weeks Erythema with sever mucositis Erythema with sever mucositis With or without ulceration Pain and disphagia Pain and disphagia Loss of test- test bud atrophy Loss of test- test bud atrophy Delayed healing Delayed healing Pale and less vascular mucosa Pale and less vascular mucosa Radiotherapy induced Submucous fibrosis Radiotherapy induced Submucous fibrosis

20
ORAL CANCER RADIOTHERAPY

21
Salivary glands 1st week of radiotherapy 1st week of radiotherapy Xerostomia Xerostomia Difficulty in swallowing Difficulty in swallowing Nasua Nasua Rampant caries Rampant caries Periodontitis Periodontitis Recovery 3 to 4 months Recovery 3 to 4 months

22
Management Sipped of water Sipped of water Salivary substitute Salivary substitute Mucous based sprays -saliva orthane spray Cellulose --- glandosane, glycerin Pilocarpine hydrocloride 5mg QID Cevimelive hydroloride 30mg TDS Stimulation of exocrine gland

23
Skin Erythema Erythema 3 rd week 3 rd week Dose greater than 50 gy Dose greater than 50 gy Healing 7 to 10 days Healing 7 to 10 days

24
Bone Osteoradionecrosis Osteoradionecrosis Is devitilization of bone after cancericidal dose of radiation Is devitilization of bone after cancericidal dose of radiation Endarteritis Endarteritis Bone turn over become slow, remolding dose not occur leads to exposed bone Bone turn over become slow, remolding dose not occur leads to exposed bone

29
ORAL CANCER RADIOTHERAPY

33
Other effects Alteration of flora Alteration of flora Inc anaerobic species Inc anaerobic species Inc fungi, Candida Inc fungi, CandidaNystatin 0.1% chlorexidine

34
Late effects of radiation Eyes Eyes Cataract 10 gy Blindness 50 gy Spinal cord Spinal cord Paraplegia dose Inc 45gy Carotid artery stenosis Carotid artery stenosis

35
ORAL CANCER RADIOTHERAPY Conclusion Surgery is the first choice Surgery is the first choice Surgery may be followed by Radiotherapy or Chemotherapy if required Surgery may be followed by Radiotherapy or Chemotherapy if required Where bone is involved, Radiotherapy / Chemotherapy do not work Where bone is involved, Radiotherapy / Chemotherapy do not work Radiotherapy / Chemotherapy alone only work as palliative therapy Radiotherapy / Chemotherapy alone only work as palliative therapy Radiotherapy must be done under the supervision of experienced oncologist Radiotherapy must be done under the supervision of experienced oncologist

36
ORAL CANCER RADIOTHERAPY THANK YOU

37
Evaluation of dentition before radiotherapy Most feared side effect is ORN Most feared side effect is ORN Factor determine the fate of teeth Factor determine the fate of teeth 1. Condition of residual dentition-- ? 2. Pt awareness – past care pt with good oral hygiene, the clinician must retain as many of teeth as possible pt with good oral hygiene, the clinician must retain as many of teeth as possible Neglected oral health --ext Neglected oral health --ext

38
Factor determine the fate of teeth 3 Immediacy of radiotherapy 4 Radiation location Pre radiation ext considered 1- 2 week delay radiation 5 Radiation dose Inc 50 GY--- ext indicated Less than 50 – conservative

39
Preparation of dentition for radiotherapy Pre radiation Pre radiationRestorations Topical fluoride application Oral hygiene measures and instructions Prevention of mechanical trauma Encourage to stop habitts

40
Preparation of dentition for radiotherapy cont Per radiation Per radiation Rinse mouth with saline at least 10 times daily Rinse mouth with saline at least 10 times daily Chlorhaxidine mouth wash 2 times Chlorhaxidine mouth wash 2 times Dental evaluation twice a week during radiotherapy Dental evaluation twice a week during radiotherapy If overgrowth of candida than nystatin / clotimazole If overgrowth of candida than nystatin / clotimazole Exercise – maintain mouth opening Exercise – maintain mouth opening Weight loss should be checked NG tubes Weight loss should be checked NG tubes

41
Post radiation Post radiation Regular follow up every 3- 4 week Regular follow up every 3- 4 week Topical fluoride Topical fluoride

42
Method of preparing preirradiation extraction atraumatic extraction atraumatic extraction Interval B/w preirradiation ext and beginning of radiotherapy Interval B/w preirradiation ext and beginning of radiotherapy 7-14 days 3 weeks if possible

43
Impacted 3 rd molar removal before radiotherapy Partially erupted Partially erupted Complete embedded Complete embedded

44
Carious teeth after radiotherapy Treatment accordingly Treatment accordingly Composite, amalgam Composite, amalgam Necrotic pulp __ RCT Necrotic pulp __ RCT If RCT is difficult – amputation above the gingiva left at place If RCT is difficult – amputation above the gingiva left at place

45
Tooth ext after radiotherapy 4 month gap 4 month gap HBO before and after ext HBO before and after ext 20- 30 dives 20- 30 dives

46
Denture after radiation Yes Yes Soft liners Soft liners

Similar presentations









 ‘ Brushing Up on Mouth Care ’ Education.>")















