Download presentation
Presentation is loading. Please wait.

1
Abdominal Compartment Syndrome (ACS) Dr Emily Lai Princess Margaret Hospital Joint Hospital Surgical Grand Round 17 Apr 2010
 Dr Emily Lai Princess Margaret Hospital Joint Hospital Surgical Grand Round 17 Apr 2010")
2
World Congress on Abdominal Compartment Syndrome 2004 Intra-abdominal pressure (IAP): – steady-state pressure concealed within the abdominal cavity; –increases with inspiration and decreases with expiration –affected by the volume of solid organs and the intestines, space-occupying lesions, and the extensibility of the abdominal wall Abdominal perfusion pressure = MAP – IAP
: – steady-state pressure concealed within the abdominal cavity; –increases with inspiration and decreases with expiration –affected by the volume of solid organs and the intestines, space-occupying lesions, and the extensibility of the abdominal wall Abdominal perfusion pressure = MAP – IAP")
3
World Congress on Abdominal Compartment Syndrome 2004 Normal IAP ~ 5-7mmHg Intra-abdominal hypertension (IAH) –Sustained or repeated pathological elevation in IAP >= 12mmHg Abdominal compartment syndrome (ACS) –a sustained IAP > 20mmHg that is associated with a new organ dysfunction / failure
 –Sustained or repeated pathological elevation in IAP >= 12mmHg Abdominal compartment syndrome (ACS) –a sustained IAP > 20mmHg that is associated with a new organ dysfunction / failure")
4
Classification of ACS Primary –Associated with injury or disease in the abdominopelvic region or a condition that develops after abdominal surgery –Frequently requires early surgical and radiological intervention –e.g. # pelvis, massive retroperitoneal haematoma, ruptured AAA, ileus, post-liver transplantation

5
Classification of ACS Secondary (medical or extra-abdominal) –Include conditions that do not originate from the abdomen –e.g. major burns, sepsis or other condition requiring massive fluid resuscitation

6
Classification of ACS Recurrent (tertiary) –ACS redevelops following previous surgical or medical treatment of primary or secondary ACS –Associated with significant morbidity and mortality
 –ACS redevelops following previous surgical or medical treatment of primary or secondary ACS –Associated with significant morbidity and mortality")
7
Causes of ACS Intraperitoneal or retroperitoneal haematoma –Trauma, # pelvis, ruptured AAA… Sepsis –Intra-abdominal sepsis, pancreatitis, major burns… Excessive fluid resuscitation > 5L within 24 hours Pneumoperitoneum Ileus/ intestinal obstruction Iatrogenic –Post incisional hernia repair, post abdominal packing… ** Patient with ascites, large abdominal tumors, pregnancy and morbid obesity have lower thresholds to develop ACS

8
Pathophysiology Physiological Insult/ critical illness (e.g. Haemorrhage, sepsis) Systemic inflammatory response Capillary endothelial damage Interstitial edema (including bowel wall and mesentery) Fluid accumulates, stretching the abdominal wall until it becomes less compliant Intra-abdominal pressure increases
 Systemic inflammatory response Capillary endothelial damage Interstitial edema (including bowel wall and mesentery) Fluid accumulates, stretching the abdominal wall until it becomes less compliant Intra-abdominal pressure increases.")
9
Multisystem effects of ACS Cardiovascular –Compression of IVC diminishes venous return to the heart (preload) –Increased afterload due to raised systemic vascular resistance and raised intra-thoracic pressure – Reduces cardiac output –Venous stasis in the legs
 –Increased afterload due to raised systemic vascular resistance and raised intra-thoracic pressure – Reduces cardiac output –Venous stasis in the legs")
10
Multisystem effects of ACS Respiratory –Diaphragm is forced into the thorax, reducing the intra-thoracic volume, increasing the intra- thoracic pressure and compressing lung parenchyma – Hypoventilation and VQ mismatch causing hypoxia and respiratory acidosis –Compensatory increase in positive end expiratory pressure may further impede venous return and raised jugular pressure, which can result in raised ICP and cerebral edema

11
Multisystem effects of ACS Renal –Reduction in GFR and renal plasma flow, with increase in renal vascular resistance –Leads to oliguric renal failure –Raised ADH, renin and aldosterone leads to retention of sodium and water

12
Multisystem effects of ACS Gastrointestinal –marked reduction in hepatic, splanchnic and mesenteric blood flow when IAP > 15 – Mucosal ischemia and translocation of bacteria or inflammatory mediators into the circulation –Provokes systemic inflammatory response, prolonged ileus or leads to anastomotic dehiscence post-operatively Central nervous system –Raised intracranial pressure

14
Symptoms/ signs No characteristic clinical signs are indicative of ACS Clinical judgment fails to detect significant IAH over 40% of the time –Kirkpatrick, A.W., et al., Is clinical examination an accurate indicator of raised intra- abdominal pressure in critically injured patients ? Can J Surg, 2000. 43(3): p. 207-11. –Sugrue, M., et al., Clinical examination is an inaccurate predictor of intraabdominal pressure. World J Surg, 2002. 26(12): p. 1428-31.
: p –Sugrue, M., et al., Clinical examination is an inaccurate predictor of intraabdominal pressure. World J Surg, (12): p")
15
Measurement of IAP Direct –Catheter in the peritoneum Indirect – Intravesical pressure (Gold standard) –Stomach pressure –Rectal pressure –Uterine pressure –Inferior vena cava pressure
 –Stomach pressure –Rectal pressure –Uterine pressure –Inferior vena cava pressure")
16
Bladder Technique Foley catheter tubing clamped 50ml saline instilled into the bladder A 16G needle inserted via the aspiration port proximal to the clamp and attached to a pressure transducer/ manometer The level of pubic symphysis is used as zero Measured at end-expiration and in supine position Contraindication: patient with suspected or confirmed bladder trauma

17
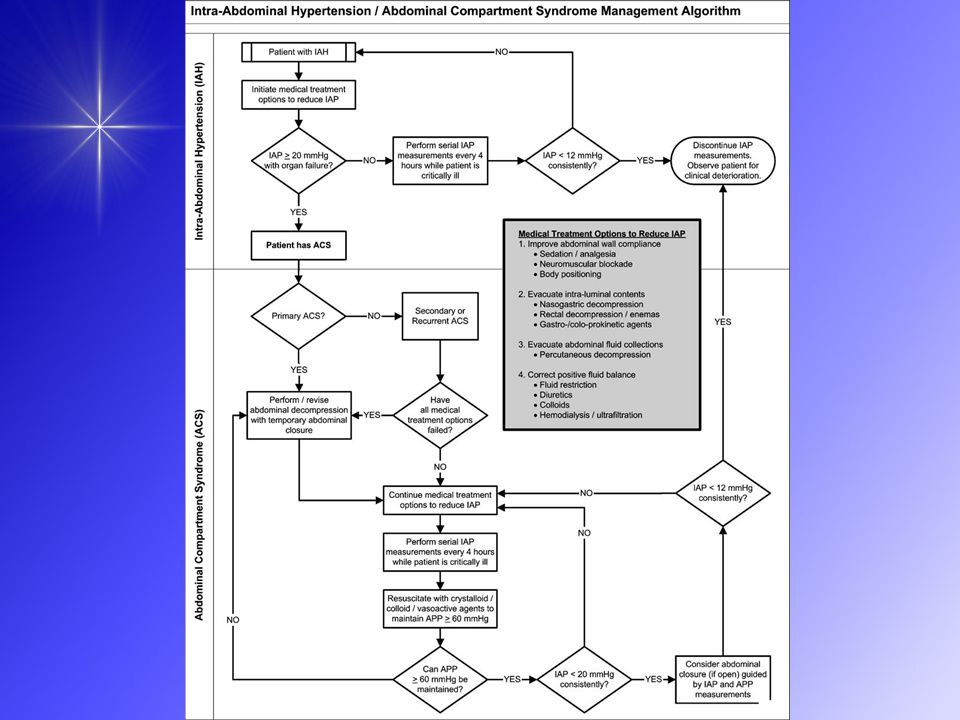
Management Medical Operative

18
Medical Management Close monitoring in ICU Sedation and paralysis Optimization of ventilation and oxygenation Optimal fluid resuscitation Administration of inotropes Gastric suctioning Correction of coagulopathy Correction of hypothermia CVVH for aggressive correction of metabolic acidosis associated with acute renal failure despite medical therapy

19
Operative Treatment Decompressive laparotomy –immediate improvement of haemodynamic status –Variety of techniques e.g. Bogota bag, Wittmann patch, vacuum-pack closure Temporary abdominal closure http://www.mdconsult.com/

20
Bogota bag http://bestpractice.bmj.com/best-practice/monograph/1125/resources/images.html

21
Decompressive laparotomy (DL) Detailed effects of DL on organ function are only rarely reported. IAP threshold levels for DL reported in the literature vary considerable. DL decreases IAP to < 20 mmHg in most studies A positive effect on organ function is reported in most studies, but the effect is inconsistent, and the duration of this effect is not clear. Reported mortality after DL for ACS is high. Jan J De Waele et al. Decompressive laparotomy for abdominal compartment syndrome – a critical analysis Critical Care 2006, 10:R51

23
Decompression-reperfusion Syndrome Haemodynamic instability Release of lactic acid, potassium and adenosine that accumulate during anaerobic metabolism Result in arrhythmias, metabolic acidosis and cardiac depression

24
Conclusion Abdominal compartment syndrome is fatal Early recognition of patients at risk, frequent monitoring of IAP, and early initiation of treatment are important in preventing irreversible multiorgan failure.

25
References World Society of the Abdominal Compartment Syndrome www.wsacs.org Results from the International Conference of Experts on Intra- abdominal hypertension and Abdominal Compartment Syndrome Intensive Care Med (2006) 32:1722–1732 Narendra Nath Basu, Simon Cottam Abdominal Compartment Syndrome Surgery 2006 260-262 Scheppach et al. Abdominal Compartment syndrome Best practice & Research Clinical Gastroenterology 23 (2009) 25-33 Kirkpatrick, A.W., et al., Is clinical examination an accurate indicator of raised intra-abdominal pressure in critically injured patients ? Can J Surg, 2000. 43(3): p. 207-11. Sugrue, M., et al., Clinical examination is an inaccurate predictor of intraabdominal pressure. World J Surg, 2002. 26(12): p. 1428-31. Jan J De Waele et al. Decompressive laparotomy for abdominal compartment syndrome – a critical analysis Critical Care 2006, 10:R51 Guideline for management of abdominal compartment syndrome (ACS) in trauma patients in PMH ICU
 Kirkpatrick, A.W., et al., Is clinical examination an accurate indicator of raised intra-abdominal pressure in critically injured patients . Can J Surg, (3): p Sugrue, M., et al., Clinical examination is an inaccurate predictor of intraabdominal pressure. World J Surg, (12): p Jan J De Waele et al. Decompressive laparotomy for abdominal compartment syndrome – a critical analysis Critical Care 2006, 10:R51 Guideline for management of abdominal compartment syndrome (ACS) in trauma patients in PMH ICU.")
Similar presentations


 for severe sepsis and septic shock treatment>")










. INTRODUCTION ACS has sometimes been used with the term intra-abdominal hypertension (IAH) interchangeably. IAH exists.>")

 Dr. Meg-angela Christi Amores.>")
 Abdominal Compartment Syndrome (ACS) & By: Tim Wolfe, MD>")


