Download presentation
Presentation is loading. Please wait.

1
Lecture 6 and 7 Myelodysplastic syndromes; Chronic lymphocytic leukemia and related lymphoproliferative disorders Abdulkarim Aldosari

2
Objectives Describe the etiology, pathogenesis, clinical features and treatment of MDS Describe laboratory diagnosis of MDS Differentiate the subtypes of MDS based on morphology and laboratory features Distinguish between MDS and AML on PB and BM smears Know the International Prognostic Scoring System (IPSS) List general features of chronic lymphocytic leukemia List diagnostic criteria of CLL Explain differential diagnostic criteria used to characterize lymphoproliferative disorders Name laboratory methods used to study lymphocytes in lymphoproliferative disorders
 List general features of chronic lymphocytic leukemia. List diagnostic criteria of CLL. Explain differential diagnostic criteria used to characterize lymphoproliferative disorders. Name laboratory methods used to study lymphocytes in lymphoproliferative disorders.")
3
Myelodysplastic syndromes
The Myelodysplastic syndromes (MDS) are a collection of myeloid malignancies characterized by one or more peripheral blood cytopenias. MDS are diagnosed in slightly more than 10,000 people in the United States yearly, for an annual age-adjusted incidence rate of approximately 4.4 to 4.6 cases per 100,000 people. They are more common in men and whites. The syndromes may arise de novo or secondarily after treatment with chemotherapy and/or radiation therapy for other cancers or, rarely, after environmental exposures.
 are a collection of myeloid malignancies characterized by one or more peripheral blood cytopenias. MDS are diagnosed in slightly more than 10,000 people in the United States yearly, for an annual age-adjusted incidence rate of approximately 4.4 to 4.6 cases per 100,000 people. They are more common in men and whites. The syndromes may arise de novo or secondarily after treatment with chemotherapy and/or radiation therapy for other cancers or, rarely, after environmental exposures.")
4
Myelodysplastic syndromes
In Myelodysplastic diseases, the blood stem cells do not mature into healthy cells Versus myeloproliferative diseases - the total number of blood cells increases, usually mature cells A heterogeneous group of clonal hematological malignancies Characterized by PB cytopenias, dysplastic blood cells, propensity to become acute leukemia Clinical outcome is variable Outcome is almost always fatal No cure except for allogeneic stem cell transplantation

5
MDS etiology and pathogenesis
Mostly affect the elderly – 70+ years Mostly male Risk factors – exposure to environmental and occupational products Ammonia, petrochemicals, low dose irradiation, exposure to benzene, smoking, family history Mechanism that causes MDS not well known Genetic mutations/defects Caused by a somatic mutation → a growth advantage of the neoplastic cell

6
MDS etiology and pathogenesis
Which hematopoietic progenitor cell is responsible for the neoplastic clone? Pluripotent stem cell or an omnipotent stem cell? Controversial subject > various studies done Blast cell population in leukemic patients = myeloid or myelomonocytic Only few cases the blasts are lymphoid Most studies show that blasts arise from repopulating stem cells committed to myeloid differentiation

7
MDS etiology and pathogenesis
The main biological feature of MDS is increased apoptosis –programmed cell death Ineffective hematopoiesis seen in MDS – caused by abnormally high rate of intramedullary apoptosis Factors that are involved in stimulating apoptosis are increased and those which are anti- apoptotic are decreased TNF-α and TGF-β, Fas-ligand → initiate apoptosis GM-CSF - anti-apoptotic TNF-α and TGF-β are both ↑ in MDS patients GM-CSF ↓ in MDS patients The balance between growth-stimulatory and growth-inhibitory cytokines may favor apoptosis

8
MDS etiology and pathogenesis
Loss of genetic material is the most common genetic anomaly found in MDS MDS patients are missing key genes essential for maintaining normal hematopoiesis No single gene found – focus of research Characterized mainly by chromosomal deletions Either sections of a chromosome or the entire chromosome Versus chromosomal translocations in acute leukemias Deletions follow a tumor suppressor gene model Tumor-suppressor genes generally encode proteins that inhibit cell proliferation – (in MDS = apoptosis) Need mutated allele from both parents – recessive model Versus oncogene activity of acute leukemias Missing genes → more genetic anomalies → disease progression
 Need mutated allele from both parents – recessive model. Versus oncogene activity of acute leukemias. Missing genes → more genetic anomalies → disease progression.")
9
MDS progression Characteristics of MDS changes as it progresses towards leukemia Blast cells ↑ Leukocytosis replaces leukopenia Hepatoslenomegaly occurs Becomes a proliferative PB disorder Progression due to ↓ in medullary apoptosis, ↓ in apoptosis factors (Fas ligand) Multistep pathogenesis Normal → clonal and dysplastic → full blown malignancy → acute
 Multistep pathogenesis. Normal → clonal and dysplastic → full blown malignancy → acute.")
10
Morphology of PB and BM in MDS
Reliable analysis of blast phenotype of MDS difficult Blasts are not predominant in the BM and PB Determined using immunophenotyping Expression of CD34 > myeloid antigens > myeloid blasts Blast in BM determine type of MDS at initial diagnosis Different types of blasts and sideroblast according to FAB classification Type 1 myeloblast - variable size without granules or Auer rods Type 11 myeloblast– slightly larger with 1-20 granules Type 111 myeloblast –with ~20 granules, basophilic cytoplasm Type 1 sideroblast – 1-4 cytoplasmic iron-containing granules = 15-50% erythroblasts Type 11 sideroblast – 2-10 granules, scattered throughout cytoplasm Type ringed sideroblast

11
Morphology of PB and BM in MDS
MDS characterized by multilineage morphological abnormalities Lineage dysplasia includes: Dyserythropoiesis In PB – macrocytic/normochromic anemia in 90% of cases, ↓ retic count, macrocytosis, anisopoikilocytosis, basophilic stippling, dimorphic RBC population (normochromic, hypochromic), Pappenheimer bodies, teardrop (dacryocytes), schistocytes, elliptocytes, Howell-jolly bodies, acanthocytes In BM – Erythroblasts with asynchronous cytoplasmic maturation, internuclear bridging, nuclear budding, Howell-Jolly bodies, Basophilia, ghosts cells, abnormal ringed sideroblasts (types 1 and 11)
, Pappenheimer bodies, teardrop (dacryocytes), schistocytes, elliptocytes, Howell-jolly bodies, acanthocytes. In BM – Erythroblasts with asynchronous cytoplasmic maturation, internuclear bridging, nuclear budding, Howell-Jolly bodies, Basophilia, ghosts cells, abnormal ringed sideroblasts (types 1 and 11)")
12
Morphology of PB and BM in MDS
Megaloblastoid change Megaloblastoid erythroid precursors with and multinucleation nuclear irregularities and a multinucleated erythroid precursor

13
Morphology of PB and BM in MDS
Characterized by multilineage morphological abnormalities Lineage dysplasia includes: Dysgranulocytopoiesis in peripheral blood neutropenia in 60% of cases nuclear and cytoplasmic dysplasia in 90% of cases neutrophilia possible pseudo-Pelger-Huët and variable degrees of hyposegmentation monolobulation (pseudo- Stodtmeister anomaly) variable degrees of hypogranulation pseudo-Dohle bodies rare hypergranulation abnormal chromatin
 variable degrees of hypogranulation. pseudo-Dohle bodies. rare hypergranulation. abnormal chromatin.")
14
Stodtmeiser Pelger-Huet anomaly
Stodtmeiser anomaly

15
Morphology of PB and BM in MDS
Dysgranulocytopoiesis in bone marrow Pseudo-Pelger-Huët or Stodtmeiser anomaly, hypersegmentation ring formation chromatin sticks asynchronous nuclear-cytoplasmic maturation hybrid myelomonocytic cells vacuolated monocytes/myeloid precursors Pelger-Huët anomaly is considered to be the most specific dysplastic marker for the diagnosis of MDS

16
Morphology of PB and BM in MDS
Ring formation Hypersegmentation with nuclear sticks

17
Morphology of PB and BM in MDS
Characterized by multilineage morphological abnormalities Lineage dysplasia includes: Dysmegakaryocytopoiesis In PB – Thrombocytopenia in 60% of cases, platelet gigantism, ballooning, hypogranulation, rare thrombocytosis associated with 5q-syndrome In BM – micromegakaryocytes (dwarf or mononuclear megakaryocytes), megakaryocytes with multiple small detached nuclei, or nuclei separated by thin strand, “pawn ball” shape, cytoplasmic vacuoles
, megakaryocytes with multiple small detached nuclei, or nuclei separated by thin strand, pawn ball shape, cytoplasmic vacuoles.")
18
Morphology of PB and BM in MDS
Discrete nuclear lobes, or multinucleation Micromegakaryocytes Pawn ball megakaryocyte.

19
FAB classification Refractory anemia (RA)
MDS Peripheral Blood Bone Marrow Refractory anemia (RA) Cytogenetic studies needed to diagnose- 50% of patients have clonal abnormalities Most difficult to recognize and diagnose. Anemia 90% of cases (normochromic & macrocytic); cytopenias; variable dyserythropoiesis; <1% blasts neutropenia, dysmyelopoiesis & dysmegakaryopoiesis are rare normal - hypercellular; erythroid hyperplasia with variable dyserythropoiesis; normal myeloid & megakaryocytic lines; <5% blasts; ringed sideroblasts < 15% Refractory anemia with ringed sideroblasts (RAS) Ringed sideroblast + lineage dysplasia enough to make diagnosis Similar to RA; anemia (macrocytic or dimorphic); variable dyserythropoiesis; <1% blasts neutropenia, dysmyelopoiesis & dysmegakaryopoiesis are rare; cytopenias ringed sideroblasts >15% nucleated cells Refractory anemia with excess blasts (RAEB) Anemia (macrocytic normochromic) ovalocytes and dacryocytes; 2 or more of dyserythropoiesis, dysmyelopoiesis with hyposegmentation, hypogranulation; dysmegakaryopoiesis with thrombocytopenia, giant platelets; <5% blasts hypercellular; dyserythropoiesis, dysmyelopoiesis, and dysmegakaryopoiesis; 5-20% blasts, no Auer rods; ringed sideroblasts variable Refractory anemia with excess blasts in transformation (RAEB-t) Can mimic M2 - AML as in RAEB, but > 5% blasts, may contain Auer rods as in RAEB, but 20-30% blasts or Auer rods Chronic myelomonocytic leukemia (CMML) monocytosis >1.0 x109/L; WBC ≤ 13 x109/L <5% blasts; dysmyelopoiesis variable as in RAEB, but ↑ monocytes & promonocytes ≥ 20%; % blasts; variable ringed sideroblast FAB classification
 Cytogenetic studies needed to diagnose- 50% of patients have clonal abnormalities. Most difficult to recognize and diagnose. Anemia 90% of cases (normochromic & macrocytic); cytopenias; variable dyserythropoiesis; <1% blasts neutropenia, dysmyelopoiesis & dysmegakaryopoiesis are rare. normal - hypercellular; erythroid hyperplasia with variable dyserythropoiesis; normal myeloid & megakaryocytic lines; <5% blasts; ringed sideroblasts < 15% Refractory anemia with ringed sideroblasts (RAS) Ringed sideroblast + lineage dysplasia enough to make diagnosis. Similar to RA; anemia (macrocytic or dimorphic); variable dyserythropoiesis; <1% blasts neutropenia, dysmyelopoiesis & dysmegakaryopoiesis are rare; cytopenias. ringed sideroblasts >15% nucleated cells. Refractory anemia with excess blasts (RAEB) Anemia (macrocytic normochromic) ovalocytes and dacryocytes; 2 or more of dyserythropoiesis, dysmyelopoiesis with hyposegmentation, hypogranulation; dysmegakaryopoiesis with thrombocytopenia, giant platelets; <5% blasts. hypercellular; dyserythropoiesis, dysmyelopoiesis, and dysmegakaryopoiesis; 5-20% blasts, no Auer rods; ringed sideroblasts variable. Refractory anemia with excess blasts in transformation (RAEB-t) Can mimic M2 - AML. as in RAEB, but > 5% blasts, may contain Auer rods. as in RAEB, but 20-30% blasts or Auer rods. Chronic myelomonocytic leukemia (CMML) monocytosis >1.0 x109/L; WBC ≤ 13 x109/L. <5% blasts; dysmyelopoiesis variable. as in RAEB, but ↑ monocytes & promonocytes ≥ 20%; 1-20% blasts; variable ringed sideroblast. FAB classification.")
20
RAEB-t is eliminated; patients considered to have acute leukemia
Diseases Blood findings Bone marrow findings Comments Refractory anemia (RA) Anemia No or rare blasts Erythroid dysplasia only < 5% blasts < 15% ringed sideroblasts 5-10% Refractory anemia with ringed sideroblasts (RARS) Anemia No blasts Erythroid dysplasia only < 5% blasts ≥ 15% ringed sideroblasts Makes up about 3% to 11% of MDS cases; also generally good prognosis Refractory cytopenias with multilineage dysplasia (RCMD) Cytopenias (bicytopenia or pancytopenia) No or rare blasts No Auer rods < 1 x 109/L monocytes Dysplasia in ≥ 10% of cells in ≥ 2 myeloid cell lines < 5% blasts No Auer rods < 15% ringed sideroblasts Makes up about 30% of MDS cases; about 10% of people with RCMD will develop acute leukemia; less favorable prognosis. Refractory cytopenias with multilineage dysplasia and ringed sideroblasts (RCMD-RS) Cytopenias (bicytopenia or pancytopenia) No or rare blasts No Auer rods < 1 x 109/L monocytes Dysplasia in ≥ 10% of cells in ≥ 2 myeloid cell lines < 5% blasts ≥ 15% ringed sideroblasts No Auer rods Refractory cytopenias with excess blasts (RAEB-1) Cytopenias < 5% blasts No Auer rods < 1 x 109/L monocytes Unilineage or multilineage % blasts No Auer rods 20% of MDS cases; About 25% develop acute myeloid leukemia (AML); poorer prognosis Refractory cytopenias with excess blasts (RAEB-2) Cytopenias % blasts ± Auer rods < 1 x 109/L monocytes Unilineage or multilineage % blasts ± Auer rods 20%; Up to 40% may develop AML; the remainder of cases are fatal due to bone marrow failure. Myelodysplastic syndrome unclassified (MDS-U) Cytopenias ± Blasts ± Auer rods Unilineage in granulocytes or megakaryocyte < 5% blasts No Auer rods Variable; Lacks findings appropriate for classification into any other MDS category MDS associated with isolated del(5q) Anemia < 5% blasts Platelets normal or increased Normal to increased megakaryocytes with hypolobulated nuclei % blasts No Auer rods Isolated del(5q) < 5%; Affected cells are missing part of chromosome 5; generally good prognosis; progression to acute leukemia occurs in less than 10% of patients. WHO classification RA and RARS subdivided according to presence or absence of multilineage dysplasia RAEB-t is eliminated; patients considered to have acute leukemia CMML reclassified under a subgroup of myelodysplastic/myeloproliferative disorders Separate out patients with a 5q deletion syndrome
 Anemia No or rare blasts. Erythroid dysplasia only < 5% blasts < 15% ringed sideroblasts. 5-10% Refractory anemia with ringed sideroblasts (RARS) Anemia No blasts. Erythroid dysplasia only < 5% blasts ≥ 15% ringed sideroblasts. Makes up about 3% to 11% of MDS cases; also generally good prognosis. Refractory cytopenias with multilineage dysplasia (RCMD) Cytopenias (bicytopenia or pancytopenia) No or rare blasts No Auer rods < 1 x 109/L monocytes. Dysplasia in ≥ 10% of cells in ≥ 2 myeloid cell lines < 5% blasts No Auer rods < 15% ringed sideroblasts. Makes up about 30% of MDS cases; about 10% of people with RCMD will develop acute leukemia; less favorable prognosis. Refractory cytopenias with multilineage dysplasia and ringed sideroblasts (RCMD-RS) Cytopenias (bicytopenia or pancytopenia) No or rare blasts No Auer rods < 1 x 109/L monocytes. Dysplasia in ≥ 10% of cells in ≥ 2 myeloid cell lines < 5% blasts ≥ 15% ringed sideroblasts No Auer rods. Refractory cytopenias with excess blasts-1 (RAEB-1) Cytopenias < 5% blasts No Auer rods < 1 x 109/L monocytes. Unilineage or multilineage 5-9% blasts No Auer rods. 20% of MDS cases; About 25% develop acute myeloid leukemia (AML); poorer prognosis. Refractory cytopenias with excess blasts-2 (RAEB-2) Cytopenias 5-9% blasts ± Auer rods < 1 x 109/L monocytes. Unilineage or multilineage 10-19% blasts ± Auer rods. 20%; Up to 40% may develop AML; the remainder of cases are fatal due to bone marrow failure. Myelodysplastic syndrome unclassified (MDS-U) Cytopenias ± Blasts ± Auer rods. Unilineage in granulocytes or megakaryocyte < 5% blasts No Auer rods. Variable; Lacks findings appropriate for classification into any other MDS category. MDS associated with isolated del(5q) Anemia < 5% blasts Platelets normal or increased. Normal to increased megakaryocytes with hypolobulated nuclei 5% blasts No Auer rods Isolated del(5q) < 5%; Affected cells are missing part of chromosome 5; generally good prognosis; progression to acute leukemia occurs in less than 10% of patients. WHO classification. RA and RARS subdivided according to presence or absence of multilineage dysplasia. RAEB-t is eliminated; patients considered to have acute leukemia. CMML reclassified under a subgroup of myelodysplastic/myeloproliferative disorders. Separate out patients with a 5q deletion syndrome.")
21
Cytochemical abnormalities of MDS
Cytochemical studies included iron stain, periodic acid-Schiff (PAS), peroxidase, butyrate esterase, chloroacetate esterase, and double esterase stains ↓activity and abnormal positive results of MPO, chloroesterase, alkaline phosphatase, SSB, dual esterase in myeloid and monocytic cells Especially more difficult to diagnose RARS, RAEB-t, CMML due to major qualitative and quantitative abnormalities, than RA The iron stain remained most helpful in identifying abnormal ringed sideroblasts, a feature of dyserythropoiesis - supports the diagnosis of MDS The PAS stain was helpful, if positive, in identifying patients with MDS; when negative did not help distinguish MDS from non-MDS hematologic disorders The combination of two stains, PAS and iron stain or PAS and double esterase - helpful in excluding MDS – negative results
, peroxidase, butyrate esterase, chloroacetate esterase, and double esterase stains. ↓activity and abnormal positive results of MPO, chloroesterase, alkaline phosphatase, SSB, dual esterase in myeloid and monocytic cells. Especially more difficult to diagnose RARS, RAEB-t, CMML due to major qualitative and quantitative abnormalities, than RA. The iron stain remained most helpful in identifying abnormal ringed sideroblasts, a feature of dyserythropoiesis - supports the diagnosis of MDS. The PAS stain was helpful, if positive, in identifying patients with MDS; when negative did not help distinguish MDS from non-MDS hematologic disorders. The combination of two stains, PAS and iron stain or PAS and double esterase - helpful in excluding MDS – negative results.")
22
Bone Marrow Histology of MDS
Aspirate and biopsy helpful to estimate: Cellularity – which cells are dysplastic Histological changes – displacement of hematopoiesis cells from their usual sites Abnormal localization of immature precursors (ALIP) – may find clusters of immature myeloid cells away from the BM trabeculae = early indicator of leukemic transformation Myelofibrosis – Rare occurrence, associated with BM hypoplasia Useful to determine dysmegakaryocytopoiesis, not so much for dyserythro- or dysgranulopoeisis
 – may find clusters of immature myeloid cells away from the BM trabeculae = early indicator of leukemic transformation. Myelofibrosis – Rare occurrence, associated with BM hypoplasia. Useful to determine dysmegakaryocytopoiesis, not so much for dyserythro- or dysgranulopoeisis.")
23
Cytogenetics and molecular abnormalities of MDS
Clonal abnormalities present in 30-60% of patients with MDS Most frequent abnormalities: 5q- = deletion of the long arm of chromosome 5 The common deleted region always spans the chromosome band 5q31 Several genes related to hematopoiesis are found on 5q Genes that encode cytokines and their receptors More frequent in RA Clinical features include macrocytic anemia, normal or ↑ platelet, mild leukopenia, monolobular or dwarf megakaryocytes, erythroid hypoplasia Affects mostly females Good prognosis – median survival ~8yrs The prognosis of 5q deletions in MDS is generally favorable if they are not part of complex abnormalities

24
Cytogenetics and molecular abnormalities of MDS
Deletion comprise any region located between band 5q13 and 5q33 Band 5q31 is consistently deleted in most patients

25
Cytogenetics and molecular abnormalities of MDS
Monosomy 7 (-7) Abnormalities in chromosome 7 occur in about 20 percent of MDS patients Common in patients who have prior chemotherapy exposure Associated with a poor prognosis Monosomy 7 + complex karyotype = short survival rate and ↑ progression to AML Rarely seen in RA In children - > risk of bacterial infections independent of neutrophil count
 Abnormalities in chromosome 7 occur in about 20 percent of MDS patients. Common in patients who have prior chemotherapy exposure. Associated with a poor prognosis. Monosomy 7 + complex karyotype = short survival rate and ↑ progression to AML. Rarely seen in RA. In children - > risk of bacterial infections independent of neutrophil count.")
26
Cytogenetics and molecular abnormalities of MDS
Trisomy 8 (+8) Categorized as intermediate cytogenetic risk group The most frequent cytogenetic abnormality in de novo MDS in China Found in 15-20% of MDS 5-10% of MDS with +8 are treatment-related MDS Present in each FAB subgroup: up to 25-30% of RARS cases have +8; 15-20% of other subgroups have +8
 Categorized as intermediate cytogenetic risk group. The most frequent cytogenetic abnormality in de novo MDS in China. Found in 15-20% of MDS. 5-10% of MDS with +8 are treatment-related MDS. Present in each FAB subgroup: up to 25-30% of RARS cases have +8; 15-20% of other subgroups have +8.")
27
Cytogenetics and molecular abnormalities of MDS
Deletion of part of chromosomes 11q, 20q 20q- alone is associated with a good prognosis regarding survival and potential for AML evolution pathogenic mechanism by which 20q- alters the hematopoietic stem cells is unknown Anomalies of p17 Where p53 gene reside Associated with hypolobulated granulocytes with cytoplasmic vacuoles Mainly refractory anemia with excess of blasts RAEB/ RAEB-t in MDS Other rare chromosome abnormalities are present in a substantial portion of patients

28
Secondary MDS After significant exposure to chemotherapy, radiotherapy or other toxic agents Laboratory findings, clinical manifestations, evolution similar to new MDS Higher frequency of chromosomal abnormalities Greater tendency to early leukemic transformation

29
Clinical features of MDS
Symptoms associated with progressive bone marrow failure Depends on the degree of anemia, neutropenia, thrombocytopenia Patients without excess blast in BM may be asymptomatic for a long time Abnormal physical findings are not prominent, non specific Fatigue and malaise result from anemia. Signs and symptoms of chronic heart failure may develop in patients with underlying cardiac problems – in the elderly Petechiae, ecchymosis, and nose and gum bleeding- low platelet count. If underlying dysplastic changes were missed initially - may be mistaken for immune thrombocytopenia. Fever, cough, dysuria, or shock - serious bacterial or fungal infections associated with neutropenia.

30
MDS in children Rare- less than 5% of all blood cancers in children
The median age at diagnosis in children is 7 years old RA is the most common subtype of childhood MDS. About half of all children with MDS are diagnosed with RA RAEB and RAEB-t subtypes Symptomatic – fever, pallor, physical weakness/loss of strength Normocytic, normochromic anemia rather than macrocytic anemia ↑ risk of development of AML associated with Down’s syndrome, Fanconi’s anemia Children with treatment-related and secondary MDS tend to have less favorable treatment outcomes than children with primary MDS

31
Prognosis Factors that affect prognosis:
The number of blast cells in the bone marrow. Whether one or more types of blood cells are affected. Whether the patient has symptoms of anemia, bleeding, or infection. Whether the patient has a low or high risk of leukemia. The nature and number of chromosome abnormality Whether the myelodysplastic syndrome occurred after chemotherapy or radiation therapy for cancer. The age and general health of the patient. The presence of abnormal localization of immature precursors (ALIP)
")
32
Prognostic scoring systems
The International Prognostic Scoring System (IPSS) - used to help assess the severity of MDS Based on the IPSS score, the patient's history, and observations, a treatment plan is designed to address the MDS Based on The presence of one or more low blood cell counts (cytopenias) BM blast cell count Cytogenetic results – chromosomal changes in the marrow cells
 - used to help assess the severity of MDS. Based on the IPSS score, the patient s history, and observations, a treatment plan is designed to address the MDS. Based on. The presence of one or more low blood cell counts (cytopenias) BM blast cell count. Cytogenetic results – chromosomal changes in the marrow cells.")
33
Prognostic scoring systems

34
Diagnostic problems with MDS
Difficult to differentiate from aplastic anemia Clonal anomaly will confirm MDS BM smear for dysplastic changes Differentiate from acute myelofibrosis (AML, M7) 15% of MDS show BM fibrosis – sMDS Dry tap in BM aspiration, trilineage dysplasia, cytopenias No organomegaly Cytogenic abnormalities From essential thrombocytosis JAK2 mutation in ET Cytogenetic analysis – 5q- or other translocation in MDS
 15% of MDS show BM fibrosis – sMDS. Dry tap in BM aspiration, trilineage dysplasia, cytopenias. No organomegaly. Cytogenic abnormalities. From essential thrombocytosis. JAK2 mutation in ET. Cytogenetic analysis – 5q- or other translocation in MDS.")
35
Diagnostic problems with MDS
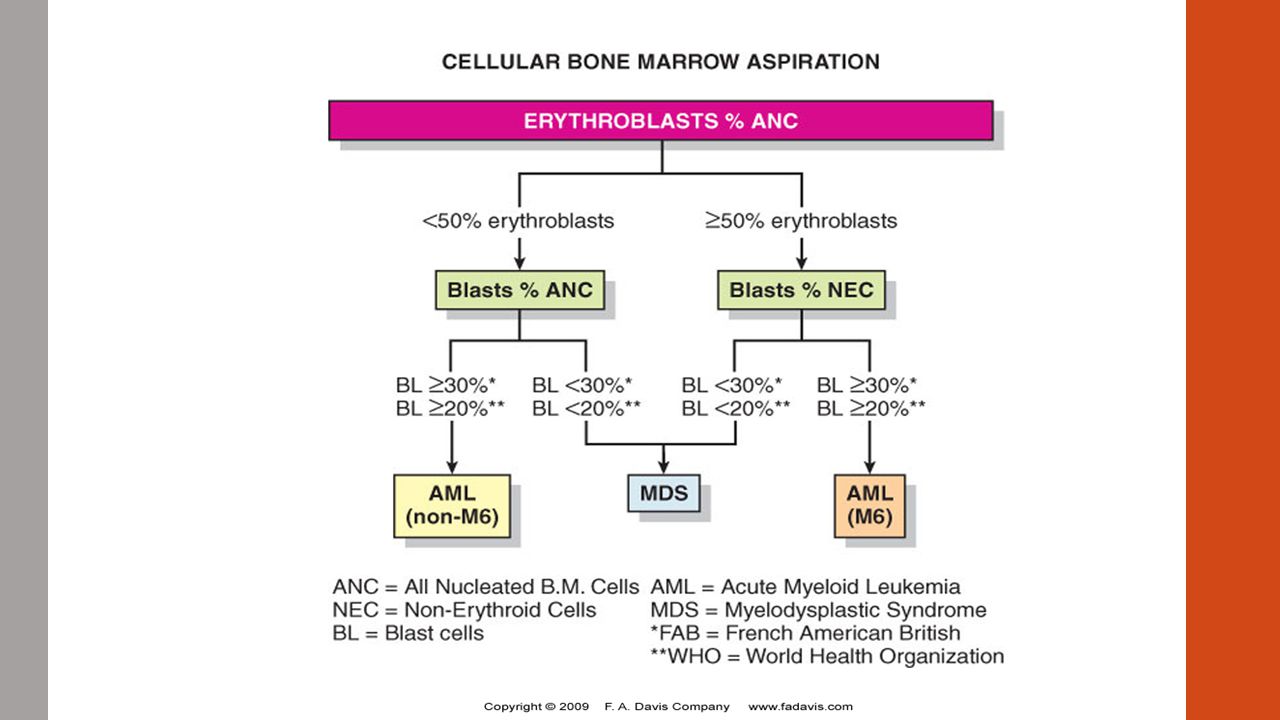
CMML to be differentiated from CML CMML, patients have an elevated number of monocytes in the blood CMML patients have abnormal looking (dysplastic) cells in their bone marrow CMML has features of both myelodysplastic syndrome and myeloproliferative disorder Cytogenetic studies to differentiate Differentiate from Acute erythroid leukemia When the total population of BM erythroblasts > 50% of all nucleated cells Algorithm to help with diagnosis
 cells in their bone marrow. CMML has features of both myelodysplastic syndrome and myeloproliferative disorder. Cytogenetic studies to differentiate. Differentiate from Acute erythroid leukemia. When the total population of BM erythroblasts > 50% of all nucleated cells. Algorithm to help with diagnosis.")
37
Treatment of MDS Allogeneic stem cell transplantation – only therapy with potential to treat MDS Since most are elderly – not as practical Limited to younger patients <60yrs with a matched sibling <55yrs unrelated but matched donor High dose chemotherapy (without transplantation) Short lived response Response - < 20% of patients still in remission 2 years after therapy Advances in pathogenesis – development of novel drugs IPSS used to tailor therapy
 Short lived response. Response - < 20% of patients still in remission 2 years after therapy. Advances in pathogenesis – development of novel drugs. IPSS used to tailor therapy.")
38
For the elderly - IPSS low or intermediate-1 risk category – treat to improve hematopoiesis
For younger patients – IPSS-2 or high risk – treat to improve survival

39
Review questions The most common dyserythropoietic finding in the bone marrow in MDS Megaloblastoid development Impaired hemoglobinization Pseudo-Pelger- Huet cells Agranular cytoplasm Ans. a Why should you test B12 and folate levels when entertaining a diagnosis of MDS? Ans. Megaloblastoid changes are often seen in the erythroid and megakaryocytic lines of MDS and are similar to abnormalities of megaloblastic anemia. MDS should not be diagnosed if there is evidence of either a B12 or folate deficiency.

40
Chronic lymphocytic disorders
Clonal proliferations of morphologically and immunophenotypically mature B or T lymphocytes Diagnosis based on morphology, immunology, cytogenetic, molecular and clinical features Leukemias = diseases affecting the BM and the PB Lymphomas = disease affecting extramedullary sites Chronic lymphoid leukemias have various stages Early stage – small tumor cells, with low proliferation, prolonged survival Transformative stage – proliferation in extramedullary sites, increase in large immature cells

41
Chronic lymphocytic disorders
Advances in cytogenetics and molecular biology show that hematopoietic neoplasms are associated with unique genotypic profile Genotype affects the development and the clinical features of the disease Advances in the development of monoclonal antibodies → identification of unique immunophenotypic profile for most leukemias and lymphomas Advances have enhanced accuracy and reproducibility of diagnosis

42
Chronic lymphocytic leukemia
A monoclonal disorder characterized by a progressive accumulation of functionally incompetent lymphocytes. Most common form of leukemia found in adults in Western countries In some people with CLL, the disease grows and progresses slowly May take years for symptoms to appear or for treatment to be needed Some patients may never need treatment for their CLL

43
Chronic lymphocytic leukemia
In other patients the disease grows more quickly and needs treatment sooner. Some patients die rapidly, within 2-3 years of diagnosis, because of complications from CLL, but most patients live 5-10 years 90% people diagnosed with CLL are over the age of 50 Mostly affects men – incidence is twice that of women When present - symptoms are related to anemia, thrombocytopenia and neutropenia Signs and symptoms may develop gradually

44
Chronic lymphocytic leukemia
B lymphocyte neoplasm (B-CLL) – T lymphocyte very rare CLL is a stage of small lymphocytic lymphoma (SLL) -a type of B-cell lymphoma primarily in the lymph nodes CLL and SLL are considered the same underlying disease but with different clinical presentation Included in the lymphoproliferative disorders
 – T lymphocyte very rare. CLL is a stage of small lymphocytic lymphoma (SLL) -a type of B-cell lymphoma primarily in the lymph nodes. CLL and SLL are considered the same underlying disease but with different clinical presentation. Included in the lymphoproliferative disorders.")
45
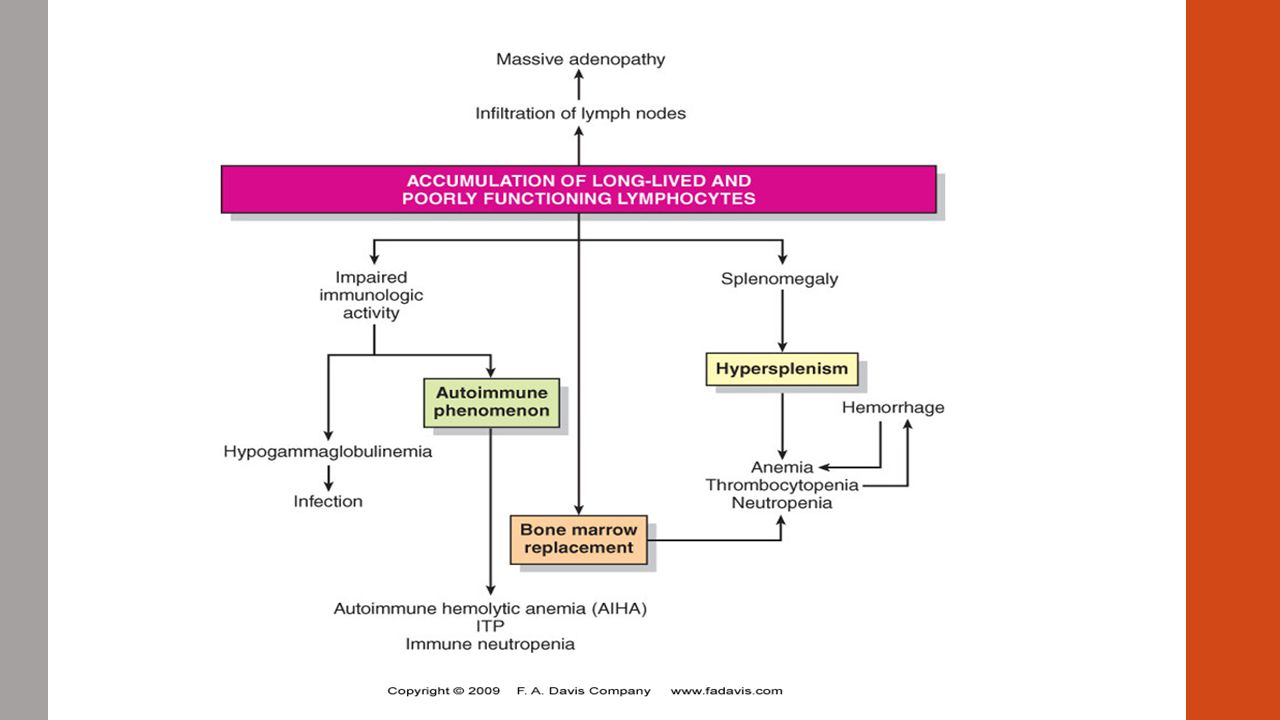
Chronic lymphocytic leukemia
Characterized by lymphocytosis in PB and BM Accumulating lymphocytes in CLL → crowding out of other cells → neutropenia, anemia, thrombocytopenia → Organ infiltration → adenopathy, splenomegaly, hypersplenism Neoplastic cells of CLL are more fragile than normal lymphocytes > burst open during smear preparation > smudge cells (bare nuclei) Smudge cells can also be found in reactive lymphocytosis and other neoplasms Therefore not diagnostic Reduce smudge cells by mixing a drop of albumin with a drop of blood prior to making smear
 Smudge cells can also be found in reactive lymphocytosis and other neoplasms. Therefore not diagnostic. Reduce smudge cells by mixing a drop of albumin with a drop of blood prior to making smear.")
46
CLL morphology CLL in BM, with numerous mature- appearing lymphocytes
CLL in PB with smudge cells

47
Chronic lymphocytic leukemia
Characterized by altered humoral immunity (antibody mediated immunity) Due to suppression of all classes of immunoglobulin (Ig) → hypogammaglobulinemia → increased susceptibility to infections Production of autoantibodies → autoimmune disease - idiopathic thrombocytopenia or autoimmune hemolytic anemia 15-35% of patients develop autoimmune hemolytic anemia at some time during course of the disease Immune-mediated destruction of red blood cells and platelets = unique feature that is not present in other kinds of leukemia .
 Due to suppression of all classes of immunoglobulin (Ig) → hypogammaglobulinemia → increased susceptibility to infections. Production of autoantibodies → autoimmune disease - idiopathic thrombocytopenia or autoimmune hemolytic anemia % of patients develop autoimmune hemolytic anemia at some time during course of the disease. Immune-mediated destruction of red blood cells and platelets = unique feature that is not present in other kinds of leukemia. .")
48
Chronic lymphocytic leukemia
51% of B-CLL patients positive for Bence-Jones paraproteinemia Bence Jones proteins are considered the first tumor marker; made by plasma cells; The presence of these proteins in a person's urine is associated with a malignancy of plasma cells .

49
Cause and physiological process of CLL
No specific cause known Possibly due to viral infections B-CLL cells from some patients appear to be a malignant transformation of an antigen-committed B cell responding to the human T-lymphotropic virus type 1 (HTLV-1) infection HTLV-1 infection seems to precede development of CLL in some patients May be due to failed apoptosis B-CLL cells have been shown to have high levels of anti-apoptotic agents (protein BCL2) The proto-oncogene BCL2 is a known suppressor of apoptosis, resulting in a long life for the involved cells BCL-2 seen in 80% of B-CLL cells Presence of p53- tumor suppressor gene in CLL –del of 17p
 infection. HTLV-1 infection seems to precede development of CLL in some patients. May be due to failed apoptosis. B-CLL cells have been shown to have high levels of anti-apoptotic agents (protein BCL2) The proto-oncogene BCL2 is a known suppressor of apoptosis, resulting in a long life for the involved cells. BCL-2 seen in 80% of B-CLL cells. Presence of p53- tumor suppressor gene in CLL –del of 17p.")
51
Cause and physiological process of CLL
Deregulation of cell cycle regulatory genes Abnormality of the regulation of cell proliferation CLL is characterized by the gradual accumulation of small mature B cells which are in the G0/G1 phase of the cell Cell Cycle progression governed by interactions between cyclins, cyclin-dependent kinases (CDKs), cyclin-dependent kinase inhibitors cyclin D1 and D3 mRNA levels correlated positively with lymphocyte doubling time (LDT) cyclin D1 and D3 mRNA levels were 4 to 6-fold higher in CLL cells than in normal peripheral blood B cells
, cyclin-dependent kinase inhibitors. cyclin D1 and D3 mRNA levels correlated positively with lymphocyte doubling time (LDT) cyclin D1 and D3 mRNA levels were 4 to 6-fold higher in CLL cells than in normal peripheral blood B cells.")
53
Immunologic features for studying lymphocytes
20% of circulating lymphocytes have surface Igs and are B cells 61-89% are T cells 22% are NK cells It is not possible to differentiate by morphological features only Need to differentiate in lymphoproliferative disorders As lymphocyte matures from pluripotent stem cell → lymphoid tissue – acquire developmental markers – identify subpopulations

54
Immunologic features for studying lymphocytes
Malignant B-cells do not progress normally; do not become plasma cell – arrested development – at earlier stage Genetic recombination – generate an immature B cell that expresses functional sIg Characteristic immunophenotype for B-CLL – expression of sIg

55
Chromosomal abnormalities
Most common in B-CLL is an extra chromosome 12 = trisomy 12 Occurs in 15-20% of cases May occur alone or with other deletions or translocations of chromosome 13q14 Most common chromosomal abnormality – 13q In 25% of cases Early clonal abnormality Suggestive of a loss or inactivation of a tumor suppressor gene Undetectable at cytogenetic level Detectable in 50% of CLL cases using molecular probes for the 13q14 region Presence of multiple chromosomal abnormalities = poor prognosis indicator Trisomy 12 Del 11q Del 17p13 (p53) 13q, 14q abnormalities
 13q, 14q abnormalities.")
56
Chromosomal abnormalities

57
Chromosomal abnormalities

58
Clinical course of CLL Median survival for CLL = 4-5yrs
50% of patients live beyond 5yrs 30% have a 10yr survival Can be indolent, asymptomatic, may not require any treatment Until lymphocytosis of the PB, BM, lymphadenopathy, splenomegaly, anemia, neutropenia, thrombocytopenia, autoimmune symptoms, and infection develops This can take up to 10-15yrs to develop after initial diagnosis

59
Clinical course of CLL On the other hand – 20% of cases have aggressive clinical course Rapid progression > Death within 1-2yrs Not clear why the variation in response to the disease Various prognostic markers used to help predict outcome CD38, ZAP-70, and mutational status of Ig heavy chain variable region (VH) ZAP-70 = protein normally expressed near the surface membrane of T cells and natural killer cells. It is part of the T cell receptor, and plays a critical role in T-cell signaling Aggressive CLL = higher expression of CD38, ZAP-70, “unmutated” Ig VH gene Clinical and pathologic data have been used to try to predict prognosis, to identify stages and risk groups
 ZAP-70 = protein normally expressed near the surface membrane of T cells and natural killer cells. It is part of the T cell receptor, and plays a critical role in T-cell signaling. Aggressive CLL = higher expression of CD38, ZAP-70, unmutated Ig VH gene. Clinical and pathologic data have been used to try to predict prognosis, to identify stages and risk groups.")
60
Staging of CLL Two staging systems are in common use for CLL:
Modified Rai staging in the United States Has historical precedent and widely used Binet staging in Europe Neither is completely satisfactory - both have often been modified. These CLL staging systems have been unable to provide information regarding disease progression due to its heterogeneity

61
Rai-Sawitsky staging of CLL
Original 5-stage staging system was revised in 1987 to a simpler 3-stage system The revised system divides patients into low-, intermediate-, and high-risk groups Low risk (formerly stage 0) Lymphocytosis in the blood and marrow (≥ 5 x 109/L in PB, ≥ 30% lymphs in BM) 25% of presenting population Median survival > 12.5yrs
 Lymphocytosis in the blood and marrow (≥ 5 x 109/L in PB, ≥ 30% lymphs in BM) 25% of presenting population. Median survival > 12.5yrs.")
62
Rai-Sawitsky staging of CLL
Intermediate risk (formerly stages I and II) Lymphocytosis + enlarged lymph nodes - Median survival (Ms) 8.5yrs Lymphocytosis + enlarged spleen or liver, ± lymphadenopathy – Ms 6yrs 50% of presentation High risk (formerly stages III and IV) Lymphocytosis + anemia (Hgb < 11 g/dL), ± enlarged nodes, spleen, liver – Ms 1.5yrs Lymphocytosis + thrombocytopenia (plts <100 x 109/L), ± anemia, organomegaly – Ms 1.5yrs 25% of all patients
 Lymphocytosis + enlarged lymph nodes - Median survival (Ms) 8.5yrs. Lymphocytosis + enlarged spleen or liver, ± lymphadenopathy – Ms 6yrs. 50% of presentation. High risk (formerly stages III and IV) Lymphocytosis + anemia (Hgb < 11 g/dL), ± enlarged nodes, spleen, liver – Ms 1.5yrs. Lymphocytosis + thrombocytopenia (plts <100 x 109/L), ± anemia, organomegaly – Ms 1.5yrs. 25% of all patients.")
63
Binet staging of CLL Stage A Hemoglobin ≥ 10 g/dL, no anemia
Platelets ≥ 100 × 109/L, no thrombocytopenia Fewer than 3 lymph node areas involved Stage B Hemoglobin and platelet levels as in stage A 3 or more lymph node areas involved Ms 5yrs Stage C Hemoglobin < 10 g/dL Platelets < 100 × 109/L, or both Ms 2yrs After successful treatment of immune cytopenias, CLL may be down-staged

64
Staging of CLL Staging systems do not predict whether patient’s clinical course is more likely to be slow moving or progressive Most reliable predictive factor for slow growing CLL blood lymphocyte doubling time (LDT) greater than12 months Non-diffuse pattern of BM lymphocyte infiltration + a Rai stage of 0,1 or 11 (low or intermediate) Progressive clinical course and shorter survival Short LDT – less than 12 months diffuse lymphocyte infiltration of the BM + Rai of 111 or 1V (high risk) ↑ β2-microglobulin, CD23 in serum Presence of chromosomal abnormalities
 greater than12 months. Non-diffuse pattern of BM lymphocyte infiltration + a Rai stage of 0,1 or 11 (low or intermediate) Progressive clinical course and shorter survival. Short LDT – less than 12 months. diffuse lymphocyte infiltration of the BM + Rai of 111 or 1V (high risk) ↑ β2-microglobulin, CD23 in serum. Presence of chromosomal abnormalities.")
65
Transformation of CLL Prolymphocytic transformation Richter’s syndrome
Low grade, slow progression Richter’s syndrome Diffuse large-cell lymphoma Rapid progression Accounts for 5% of all deaths in CLL p53 present in 40% of patients -associated with resistance to chemotherapy Acute leukemia Unusual in CLL Terminal transformation When there is a proliferation of a new population of immature cells Appearance of chromosomal changes not previously present More malignant clone → resistance to therapy Poor prognosis

66
Clinical features of CLL
Patients > 50yrs presenting with lymphadenopathy, lymphocytosis CBC with differential shows absolute lymphocytosis > 5000 B-lymphocytes/µL Lymphocytosis must persist for longer than 3 months 30% lymphocytosis of the BM consisting of morphologically mature appearing lymphocytes Lymphocytes with hyper-clumped nuclear chromatin pattern, smudge cells Positive sIg, CD19, CD20, CD5, CD23, CD43 Cytopenia caused by clonal bone marrow involvement establishes the diagnosis of CLL regardless of the peripheral B-lymphocyte count Clonality must be confirmed by flow cytometry.

67
Other features of CLL Varies from no treatment to the use of chemotherapeutic agents with or without radiation therapy Prognosis – 50% 5yr survival; 30% ≤ 10yr survival Differential diagnosis – ALL, PLL, SLL, HCL, Sezary syndrome, LGL, ATCL, SCCL, Waldenstrom’s macroglobulinemia, viral infection

68
Clinical features and differential diagnosis of CLL
Microscopic examination of PB smear is indicated to confirm lymphocytosis Morphologically identical to SLL Presence of smudge cells = artifacts from lymphocytes damaged during the slide preparation. Large atypical cells, cleaved cells, and prolymphocytes may account for up to 55% of peripheral lymphocytes. If >55%, prolymphocytic leukemia (B-cell PLL) is a more likely diagnosis
 is a more likely diagnosis.")
69
Clinical features and differential diagnosis of CLL

70
Diagnosis of CLL CLL can be diagnosed morphologically via immunophenotyping – immunoperoxidase and flow cytometry Using monoclonal abs to detect specific surface antigens (cluster differentiation CD antigens) The typical CLL phenotype is CD5+, CD23+, FMC7-, weak expression of surface Ig (sIg) and weak or absent expression of membrane CD22 and CD79b CD 19, CD 20, CD79a, CD5, CD23, CD45, faint CD11 = B-CLL Characteristic for B-CLL = detection of a predominance of sIg with κ or λ light-chain restriction = monoclonality
 The typical CLL phenotype is CD5+, CD23+, FMC7-, weak expression of surface Ig (sIg) and weak or absent expression of membrane CD22 and CD79b. CD 19, CD 20, CD79a, CD5, CD23, CD45, faint CD11 = B-CLL. Characteristic for B-CLL = detection of a predominance of sIg with κ or λ light-chain restriction = monoclonality.")
71
Diagnosis of CLL Peripheral blood flow cytometry - most valuable test to confirm a diagnosis of CLL Confirms the presence of circulating clonal B-lymphocytes expressing CD5, CD19, CD20(dim), CD 23, and an absence of FMC-7 staining Bone marrow aspiration and biopsy with flow cytometry is not required in all cases of CLL. may be necessary in selected cases to establish the diagnosis and to assess other complicating features such as anemia and thrombocytopenia Lymph node biopsy - if lymph node(s) begin to enlarge rapidly in a patient with known CLL to assess the possibility of transformation to a high-grade lymphoma When such transformation is accompanied by fever, weight loss, and pain, it is termed Richter syndrome
, CD 23, and an absence of FMC-7 staining. Bone marrow aspiration and biopsy with flow cytometry is not required in all cases of CLL. may be necessary in selected cases to establish the diagnosis and to assess other complicating features such as anemia and thrombocytopenia. Lymph node biopsy - if lymph node(s) begin to enlarge rapidly in a patient with known CLL. to assess the possibility of transformation to a high-grade lymphoma. When such transformation is accompanied by fever, weight loss, and pain, it is termed Richter syndrome.")
72
Diagnosis of CLL Molecular testing now exists that may help predict prognosis or clinical course - not necessary for the diagnosis or staging of CLL At present, these tests are not recommended for routine use, although this may change with further research. Chromosomal evaluation using FISH can identify certain chromosomal abnormalities of CLL with prognostic significance. Patients with del(17p) tend to have a worse prognosis, as well as resistance to therapy with alkylating agents and purine analogues. Patients with del(11q) also have a worse prognosis and bulky lymphadenopathy at presentation.
 tend to have a worse prognosis, as well as resistance to therapy with alkylating agents and purine analogues. Patients with del(11q) also have a worse prognosis and bulky lymphadenopathy at presentation.")
73
Mantle cell -derived from a subset of center cells in the mantle region of lymphoid follicles. MCL represents 2-10% of all non-Hodgkin lymphomas

74
Clinical features and differential diagnosis of CLL
Patients with < 5000 B-lymphocytes/µL + lymphadenopathy and (-) cytopenias more likely = small lymphocytic lymphoma (SLL) diagnosis should be confirmed by lymph node biopsy Patients with a clonal B-cell population < 5000/µL (-) lymphadenopathy or organomegaly, cytopenia, or other disease-related symptoms = monoclonal B- lymphocytosis (MBL) MBL progress to CLL at a rate of 1-2% per year
 cytopenias more likely = small lymphocytic lymphoma (SLL) diagnosis should be confirmed by lymph node biopsy. Patients with a clonal B-cell population < 5000/µL (-) lymphadenopathy or organomegaly, cytopenia, or other disease-related symptoms = monoclonal B- lymphocytosis (MBL) MBL progress to CLL at a rate of 1-2% per year.")
75
Differential diagnosis of CLL
ALL – morphological differences of the proliferating population Smooth, nuclear chromatin of lymphoblasts in ALL versus, dense nuclear chromatin of CLL TdT (+) for ALL, TdT (-) for CLL B-prolymphocytic leukemia (B-PLL) – > 55-75% prolymphocytes <10% in CLL If 11-55% = Prolymphoid transformation = mixed cell type of CLL/PLL CD24/CD22, ± CD10 Strong expression of sIg and CD20 (+) FMC-7 antigen expressed on mature human B cells used in immunophenotypic analysis and differential diagnosis of lymphomas and leukemias Sezary syndrome – a type of cutaneous T-cell lymphoma CTCL) which belongs to a larger group of disorders known as non-Hodgkin’s lymphomas Sezary cells = malignant T lymphocytes, mature memory T cells Mycosis fungoides in the skin pleomorphic abnormal T cells with convoluted nucleus CD2, CD3, CD4, CD5 CD7 (-), CD8 (-)
 for ALL, TdT (-) for CLL. B-prolymphocytic leukemia (B-PLL) – > 55-75% prolymphocytes. <10% in CLL. If 11-55% = Prolymphoid transformation = mixed cell type of CLL/PLL. CD24/CD22, ± CD10. Strong expression of sIg and CD20. (+) FMC-7. antigen expressed on mature human B cells used in immunophenotypic analysis and differential diagnosis of lymphomas and leukemias. Sezary syndrome – a type of cutaneous T-cell lymphoma CTCL) which belongs to a larger group of disorders known as non-Hodgkin’s lymphomas. Sezary cells = malignant T lymphocytes, mature memory T cells. Mycosis fungoides in the skin. pleomorphic abnormal T cells with convoluted nucleus. CD2, CD3, CD4, CD5. CD7 (-), CD8 (-)")
76
Differential diagnosis of CLL
Hairy cell leukemia - abnormal growth of B cells The cells look "hairy" under the microscope because they have fine projections coming from their surface CD19/20/24; CD22 CD25; CD103 CD5(-) Pancytopenia Tartrate resistant acid phosphatase TRAP (+) T-granular lymphocytosis Lymphocytosis Anemia; neutropenia; thrombocytopenia Large cell size, moderate cytoplasm with prominent vacuoles CD2, CD3, CD8, CD57 (HNK-1)
 Pancytopenia. Tartrate resistant acid phosphatase TRAP (+) T-granular lymphocytosis. Lymphocytosis. Anemia; neutropenia; thrombocytopenia. Large cell size, moderate cytoplasm with prominent vacuoles. CD2, CD3, CD8, CD57 (HNK-1)")
77
ALOT, acute leukemia orientation tube; AML, acute myeloid leukemia; BC, blast crisis; BCP, B-cell precursor; BM, bone marrow; CLL, chronic lymphocytic leukemia; CLPD, chronic lymphoproliferative disorders; CML, chronic myeloid leukemia; CSF, cerebrospinal fluid; FL, follicular lymphoma; HCL, hairy cell leukemia; LN, lymph node; LST, lymphoid screening tube; MCL, mantle cell lymphoma; MDS, myelodysplastic syndrome; MPD, myeloproliferative disorders; PCD, plasma cell disorders; PCST, plasma cell screening tube; PNH, paroxysmal nocturnal hemoglobinuria; SST, small sample tube.

78
Other methods for diagnosing CLL
Molecular probes – rearrangements of B-cell Ig and T-cell receptor genes Cytogenetics – chromosomal abnormalities Cytochemistry – Electron microscopy

79
Treatment Chemotherapy Radiation therapy Stem cell transplantation
The most common treatment for CLL is the chemotherapy drug fludarabine. Radiation therapy an alternative or used in conjunction with other therapy Stem cell transplantation Only used to treat the occasional young patient with aggressive CLL, since most patients with CLL live so long that the risk of transplant can seldom be justified. Investigational therapy – clinical trials Clinical trials currently available to UCSF patients include Flavopiridol for CLL cases that don't respond to standard treatment. Flavopiridol kills CLL so quickly that blood salt and acid-base abnormalities arise, potentially causing kidney failure

80
Review questions What are the consequences of the accumulation of the lymphocytes in the peripheral blood and bone marrow in a patient with CLL? A) Neutropenia B) Anemia C) Thrombocytopenia D) All of the above E) None of the above Ans.: D
 Neutropenia. B) Anemia. C) Thrombocytopenia. D) All of the above. E) None of the above. Ans.: D.")
81
Review questions A cell that could suggest that lymphocytes in CLL are not normal is a: A) Smudge cell B) Lymphoblast C) Monoblast D) All of the above E) None of the above Ans. A
 Lymphoblast. C) Monoblast. D) All of the above. E) None of the above. Ans. A.")
82
Review questions Which type of MDS demonstrates a mild decreased white blood cell (WBC) count (3.9 ´ 10/L), increased erythropoiesis and normal numbers of blast cells in the marrow, and <15% sideroblasts? A) Refractory anemia with ringed sideroblasts (RARS) B) Refractory anemia (RA) C) Refractory anemia with excess blasts (RAEB) D) Chronic myelomonocytic leukemia (CMML) E) None of the above Ans. B
 count (3.9 ´ 10/L), increased erythropoiesis and normal numbers of blast cells in the marrow, and <15% sideroblasts A) Refractory anemia with ringed sideroblasts (RARS) B) Refractory anemia (RA) C) Refractory anemia with excess blasts (RAEB) D) Chronic myelomonocytic leukemia (CMML) E) None of the above. Ans. B.")
83
Review questions What is the purpose of transfusing granulocytes to a patient with RA? A) Prevent hemorrhages B) Prophylaxis to infection C) Increase blood volume D) Decrease plasma viscosity E) None of the above Ans.: B
 Prophylaxis to infection. C) Increase blood volume. D) Decrease plasma viscosity. E) None of the above. Ans.: B.")
Similar presentations

1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")









>")
 DEFINITION CLL is a neoplastic disease characterized by proliferation and accumulation (blood, marrow and lymphoid.>")


:>")
 leukemia Is characterized by an unregulated proliferation of myeloid elements in the bone marrow,>")
 to those.>")
>")

