Download presentation
Presentation is loading. Please wait.

1
Gastrointestinal bleeding
Ehud Melzer M.D. Kaplan Med Ctr

2
Forms of bleeding Upper Lower Occult Obscure

3
Presentation Hematemesis – vomiting of blood (or coffee ground material) (indicates bleeding proximal to the Treitz) Melena – passage of black tarry stools > 50ml (indicates degradation of blood in the bowel) Hematochezia (rectal bleeding) – passage of red blood Occult bleeding – bleeding that is not apparent to the patient and results from small amounts of blood Obscure bleeding – occult or obvious but source not identified
 Hematochezia (rectal bleeding) – passage of red blood. Occult bleeding – bleeding that is not apparent to the patient and results from small amounts of blood. Obscure bleeding – occult or obvious but source not identified.")
4
Initial patient assessment (acute bleeding)
Assess severity of bleeding: Vital signs Resuscitation: 2 large-bore IV lines Volume replacement Oxygen Careful hemodynamic & electrolyte monitoring (preferably in ICU) Transfuse blood when indicated
 Transfuse blood when indicated.")
5
Initial patient assessment
History: (should be taken during resuscitation and not instead of) Age: elderly pts tend to bleed from lesions less common than young pts (i.e. diverticula, ischemic colitis, cancer) Young pts may bleed from Meckel’s diverticula previous bleeding: ulcer hereditary telangiectasia (Osler-Weber-Rendu) diverticula Previous surgery: Aortic graft Tumor
 Age: elderly pts tend to bleed from lesions less common than young pts (i.e. diverticula, ischemic colitis, cancer) Young pts may bleed from Meckel’s diverticula. previous bleeding: ulcer. hereditary telangiectasia (Osler-Weber-Rendu) diverticula. Previous surgery: Aortic graft. Tumor.")
6
Initial patient assessment
Known liver disease NSAID’s Associated abdominal pain (ulcer, malignancy, mesenteric or colonic ischemia) Retching (Mallory-Weiss) Change in bowel habits, anorexia, weight loss (suspect malignancy)
 Retching (Mallory-Weiss) Change in bowel habits, anorexia, weight loss (suspect malignancy)")
7
Initial patient assessment
Physical examination: Skin: Spider angiomata Telangiectasia Hyperpigmentation (Peutz-Jegher) Abdomen: Hepato-splenomegaly Ascites Caput medusae Tenderness Mass Lymphadenopathy
 Abdomen: Hepato-splenomegaly. Ascites. Caput medusae. Tenderness. Mass. Lymphadenopathy.")
8
Lab Hemoglobin: in early stage of acute bleeding does not reflect actual amount of blood loss Chronic overt or occult bleeding: hypochromic microcytic anemia reflecting iron deficiency Urea: may be elevated in upper GI bleeding out of proportion to elevation of creatinine (breakdown of blood proteins by bacteria) Fe, transferrin. ferritin
 Fe, transferrin. ferritin.")
9
Clinical localization of bleeding
Hematemesis – always UGI source Melana – indicates that blood has been in GIT for extended periods – Mostly UGI Small bowel Rt colon (if bleeding relatively slow) Hematochezia – Mostly colon Massive UGI bleeding (not enough time for degradation)
 Hematochezia – Mostly colon. Massive UGI bleeding (not enough time for degradation)")
10
Acute UGI bleeding Following resuscitation the diagnostic tool of choice is gastroscopy Endoscopic therapy Timing Visibility

11
Acute UGI bleeding - Esophagitis
< 10% of cases Tx – aimed at the cause – mainly reflux disease

12
Acute UGI bleeding - Mallory-Weiss Tear
Mucosal laceration at the GEJ 10% of cases Typically follows retching but mostly on 1st vomit (75%) 90% stop bleeding spontanuously Endoscopic Tx sometimes required
 90% stop bleeding spontanuously. Endoscopic Tx sometimes required.")
13
Acute UGI bleeding – portal hypertension
Source of bleeding – Esophageal varices Gastric varices Portal hypertensive gastropathy Urgent gastroscopy – Sclerotherpay Band ligation Somatostatin Antibiotic prophylaxis (quinolones?) Balloon tamponade (Sengstaken-Blackmore tube)
 Balloon tamponade (Sengstaken-Blackmore tube)")
14
Acute UGI bleeding – duodenal & gastric ulcer
Most common etiology of UGI bleeding Duodenum>stomach Predisposing factors for bleeding – NSAID’s Underlying medical conditions: IHD; cerebrovascular disease Ethanol, anticoagulant Tx Hospitalization

15
Acute UGI bleeding – duodenal & gastric ulcer
Gastric acid H. Pylori: Role in bleeding not certain but definitely, eradication prevents rebleeding Aspirin & NSAID’s: Gastric>duodenal Dose dependant risk Preparation dependant Older age – higher risk for bleeding

16
Acute UGI bleeding – duodenal & gastric ulcer
Endoscopic signs predictive of rebleeding: Active bleeding Visible vessel Adherent clot Management: Medical Tx – IV PPI’s Endoscopic injection Endoscopic coagulation Angiography + embolization Surgery

17
Acute UGI bleeding – duodenal & gastric ulcer
Prevention of rebleeding: Eradication of H. Pylori If NSAID induced – avoid if possible or add high dose H2B or PPI for as long as treated with NSAID Gastric ulcer should be always biopsied and followed until complete healing

18
Acute UGI bleeding – gastric erosions
NSAID’s Stress: Serious trauma Extensive burns Major surgery Major illness (ICU) Major neurologic disease (CVA, tumor, trauma) Alcohol abuse
 Major neurologic disease (CVA, tumor, trauma) Alcohol abuse.")
19
Acute UGI bleeding – malignancy
Malignant: Esophageal cancer Gastric cancer or lymphoma Small intestinal lymphoma or cancer Benign: Leiomyoma Gastro-Intestinal-Stromal-Tumor (GIST)
")
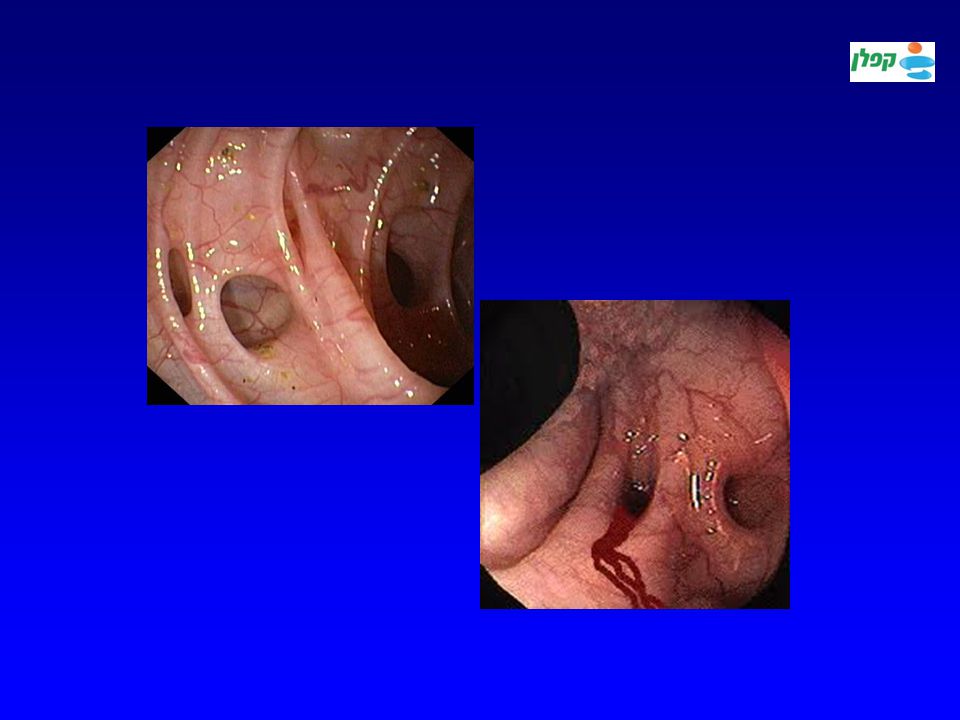
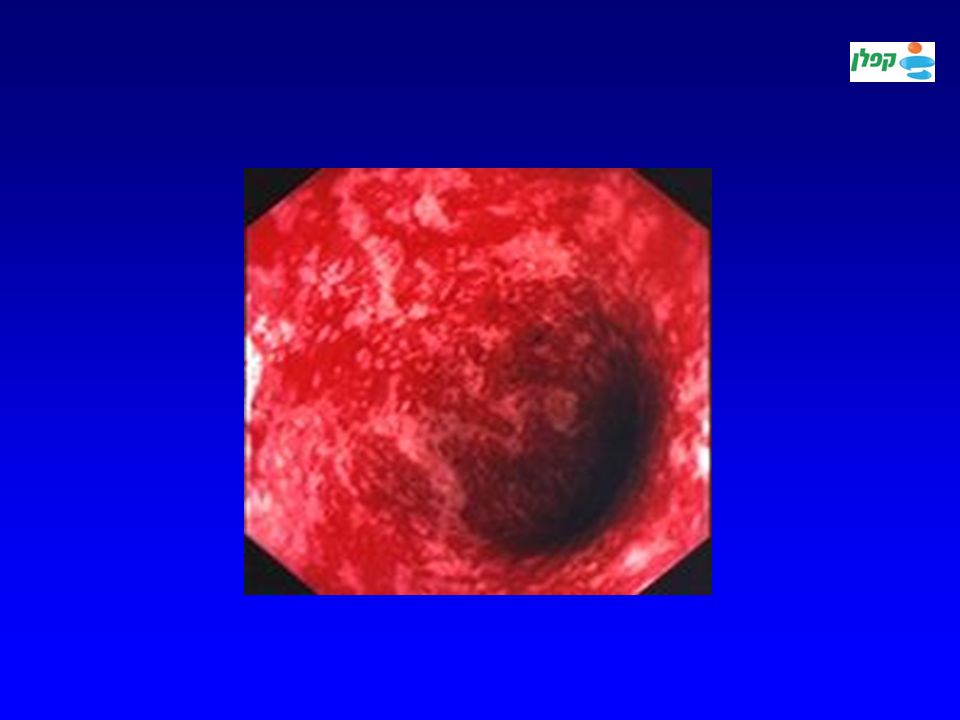
20
Acute UGI bleeding – vascular lesions
Dieulafoy Angiodysplasia Osler-Weber-Rendu syndrome

21
The surgeon’s point of view

22
Acute lower GI bleeding
Initial management – similar to acute upper GI bleeding Presentation: wide range of presentation: Mostly self-limiting bleeding that does not require hospitalization Rarely massive with hemorrhagic shock

23
Acute lower GI bleeding
Evaluation of source: History: Age (tumors & diverticular disease more common in elderly pts; IBD more common in young) HIV (CMV colitis) NSAID’s Family or personal Hx of polyps or CRC Change in bowel habits Pain (in IBD, ischemic colitis…); Anal pain Previous abdominal irradiation Previous surgery (particularly vascular) ASCVD (ischemic colitis)
 HIV (CMV colitis) NSAID’s. Family or personal Hx of polyps or CRC. Change in bowel habits. Pain (in IBD, ischemic colitis…); Anal pain. Previous abdominal irradiation. Previous surgery (particularly vascular) ASCVD (ischemic colitis)")
24
Acute lower GI bleeding
Diagnostic procedures: Colonoscopy (urgent??) Tagged RBC- scintigraphy – low predicrive value Angiography + embolization (diagnostic only if bleeding is severe) Surgery (rare)
 Tagged RBC- scintigraphy – low predicrive value. Angiography + embolization (diagnostic only if bleeding is severe) Surgery (rare)")
25
Acute lower GI bleeding diverticular disease of colon
Common cause (25%) Acute, painless, bright red, maroon or melena (depending on site) May compromise hemodynamics (elderly) Diagnosis: per exclusion Significant recurrence Tx: most subside spontaneously, some need angiographic embolization or surgery
 Acute, painless, bright red, maroon or melena (depending on site) May compromise hemodynamics (elderly) Diagnosis: per exclusion. Significant recurrence. Tx: most subside spontaneously, some need angiographic embolization or surgery.")
27
Acute lower GI bleeding angiodysplasia
Presentation: Acute (recurrent) Chronic Occult Older pts (mainly>70) High association with CRF Most – Rt colon
 Chronic. Occult. Older pts (mainly>70) High association with CRF. Most – Rt colon.")
28
Acute lower GI bleeding angiodysplasia
Diagnosis: Colonoscopy Angiography Treatment: Electrocoagulation Argon-Plasma-Coag (APC) Injection Clips Surgery
 Injection. Clips. Surgery.")
29
Acute lower GI bleeding neoplasia
Presentation: Chronic Occult Acute (rare) Diagnosis: colonoscopy Tx: according to lesion
 Diagnosis: colonoscopy. Tx: according to lesion.")
30
Acute lower GI bleeding hemorrhoids
Most common cause Presentation: recurrent low-volume bright red blood on the paper or on stool Straining aggravates bleeding Rarely associated with anemia (acute or chronic) Never relate bleeding to hemorrhoids before exclusion of other lesions Diagnosis: always colonoscope after age 50. Otherwise at least sigmidoscope
 Never relate bleeding to hemorrhoids before exclusion of other lesions. Diagnosis: always colonoscope after age 50. Otherwise at least sigmidoscope.")
31
Acute lower GI bleeding other causes
Meckel’s diverticulum (young children) Infectious colitis: Shigella; Salmonella; campylobacter Pseudo-membranous colitis (rarely bloody; Klebsiella sp.) Radiation proctitis Ischemic colitis IBD – colitis (UC;CD)
 Infectious colitis: Shigella; Salmonella; campylobacter. Pseudo-membranous colitis (rarely bloody; Klebsiella sp.) Radiation proctitis. Ischemic colitis. IBD – colitis (UC;CD)")
33
Occult bleeding Fecal Occult Blood Test (FOBT):
+ive if bleeding > 2ml/d Good for CRC screening only (reduces mortality) Of no value when iron deficieny already present
 Of no value when iron deficieny already present.")
34
Occult bleeding History: Physical examination: Age Anticoagulation
Family Hx (CRC; polyposis; Osler-Weber-Rendu) Menses Physical examination: Skin: Pallor; Telangiectasia; Café aux lait (neurofibromatosis); hyperpigmentation Lymphadenopathy Abdominal mass
 Menses. Physical examination: Skin: Pallor; Telangiectasia; Café aux lait (neurofibromatosis); hyperpigmentation. Lymphadenopathy. Abdominal mass.")
35
Occult bleeding Diagnosis: Imaging of the colon (for Fe def & FOBT):
Colonoscopy CTC ?? Gastroscopy (controversial for FOBT) Small bowel follow-through (controversial for FOBT) Video-capsule (controversial for FOBT)
 Small bowel follow-through (controversial for FOBT) Video-capsule (controversial for FOBT)")
36
Iron deficiency Low hemoglobin Microcytosis + hypochromia
Low serum iron + high transferin (saturation < 15%) Low ferritin (acute phase reactant)
 Low ferritin (acute phase reactant)")
37
Iron deficiency D.D. Chronic/occult blood loss: Esophagus: Stomach:
Esophagitis Tumor Stomach: Gastric ulcer Small intestine: Chronic inflammation (Crohn’s disease) Angiodysplasia Colon: Inflammation (CD, UC)
 Angiodysplasia. Colon: Inflammation (CD, UC)")
38
Iron deficiency D.D. Iron malabsorption: Celiac disease
Chronic parasite infestation (Ankylostoma)
")
39
Iron deficiency evaluation
History: Age Menses Pain Bowel habits Wt loss Physical examination: Pallor LN Masses

40
Iron deficiency evaluation
Procedures: Colonoscopy/Barium enema Gastroscopy+small bowel biopsy Small bowel follow-through Enteroscopy Video-capsule Meckel scan Angiography

41
The surgeon’s point of view

Similar presentations















 682-3793; (p) 413-3222.>")



