Download presentation
Presentation is loading. Please wait.

1
CPAP – A “GENTLE” VENTILATION DR ASHOK MODI MD, DNB, MRCP(UK) CONSULTANT NEONATAL INTENSIVIST Bhagirathi Neotia Woman & Child Care Centre
 CONSULTANT NEONATAL INTENSIVIST Bhagirathi Neotia Woman & Child Care Centre")
2
CONTENTS Introduction Historical aspects How it works Methods Indications WeaningWeaning Adverse effectsAdverse effects

3
Introduction Respiratory distress in a just born baby- bad news! –For doctors – Inconvenience, complications(BPD) –More so for family – death, handicap, cost Solution – CPAP –Doctors – convenient, less likely to go wrong –Family – baby saved, low cost Do I need to tell more? –Continuous distending pressure to upper & lower airways, spontaneously breathing, throughout
 –More so for family – death, handicap, cost Solution – CPAP –Doctors – convenient, less likely to go wrong –Family – baby saved, low cost Do I need to tell more. –Continuous distending pressure to upper & lower airways, spontaneously breathing, throughout.")
4
What is CPAP ? A technique of airway Management in which :- 1. Positive intrapulmonary pressure is applied artificially to the airways, whereby Distending Pressure is created in the Alveoli 2. Spontaneously breathing baby 2. Spontaneously breathing baby 3. Throughout the respiratory cycle

5
Historical aspects Harrison – 1 st increased alveolar pressure during expiration in RDS; Abolition of the grunt in RDS – deterioration Gregory et al(1971) – used CPAP 1 st in spontaneously breathing neonate in RDS Last 3 decades – long way to newer devices with better knowledge of physiology & bio- physics
 – used CPAP 1 st in spontaneously breathing neonate in RDS Last 3 decades – long way to newer devices with better knowledge of physiology & bio- physics")
6
What does it do? Prevents alveolar atelectasis, enhances & maintains FRC Decreases total airway resistance Regularises breathing pattern Improvement in surfactant metabolism Splints chest wall, airways & Pharynx Reduces work of breathing

7
What does it do? Results in reopening of collapsed/unstable alveoli - – Increased surface area for gas exchange –Preserves surfactant esp if applied early –Prevents Intrapulmonary shunting Net result improved oxygenation & ventilation

8
How to deliver CPAP Delivery of continuous positive airway pressure requires 3 components – 1. Flow circuit(warm & humidified) 2. An airway interface 3. A positive pressure system
 2. An airway interface 3. A positive pressure system.")
9
Airway Interface Single nasal prongs Binasal prongs(Short & Long) Nasopharyngeal prongs Endotracheal tube Head boxes, nasal cannulae, face masks Short binasal prongs most effective, least invasive
 Nasopharyngeal prongs Endotracheal tube Head boxes, nasal cannulae, face masks Short binasal prongs most effective, least invasive")
11
Positive pressure system Fluid column(Bubble CPAP) Resistance applied at the expiratory valve e.g Draeger / Ventilator Pressure generation at nasal level CPAP generation in the immediate vicinity of nasal airway by converting kinetic energy e.g Infant flow driver
 Resistance applied at the expiratory valve e.g Draeger / Ventilator Pressure generation at nasal level CPAP generation in the immediate vicinity of nasal airway by converting kinetic energy e.g Infant flow driver")
12
DEVICES Infant Flow Driver –unique fluid mechanics(fluidic flip action) Bubble CPAP – oscillatory vibrations Infant Ventilator with CPAP mode Which is the best?
 Bubble CPAP – oscillatory vibrations Infant Ventilator with CPAP mode Which is the best")
14
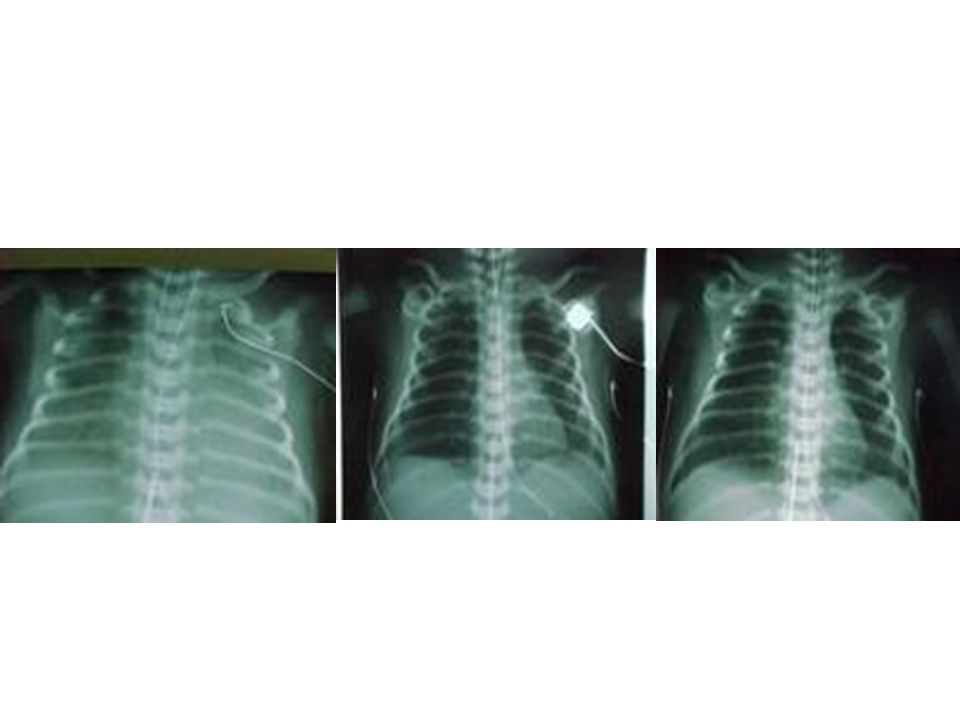
Optimal pressure No compelling Data Traditional 4 –6 cm of water However some studies as high as 10 cm H2O Tailored to baby’s needs Increments by 1 cm of water Guided by CXR

15
INDICATIONS Mild to moderate RDS Apnoea of prematurity After extubation Alternative to mechanical ventilation ( INSURE) Presence of poorly expanded or infiltrated lung fields on CXR Tracheomalacia or abnormalities of lower airways
 Presence of poorly expanded or infiltrated lung fields on CXR Tracheomalacia or abnormalities of lower airways")
16
CONTRA-INDICATIONS Definite need for intubation & Ventilation –Upper airway anomaly e.g choanal atresia, cleft lip & palate, TOF –Cardiovascular instability & impending arrest –Unstable respiratory drive –Untreated CDH –When CPAP is failing Bronchiolitis

18
Monitoring & Care Minimal handling/Sedation Nasal prongs of right size in place(FIXATION) Orogastric tube Care of the nares Change of posture Vitals & Continuous pulse oximetry Blood gas, haematological, radiological & biochemical monitoring
 Orogastric tube Care of the nares Change of posture Vitals & Continuous pulse oximetry Blood gas, haematological, radiological & biochemical monitoring")
19
Is CPAP Helping? Reduction in respiratory rate Stabilization or reduction in Fio2 Resolution of grunting Reduction in degree of sternal & intercostal recession

20
When is CPAP failing Recurrent apnoeic attacks Spontaneous episodes of desaturation Increasing oxygen requirements Worsening respiratory distress Agitation not relieved by simple measures Worsening blood gases

21
WEANING Once baby very stable with minimal respiratory distress, normal blood gas & improving CXR Fio2 gradually weaned to 40 – 50% Then pressure decreased in steps of 1 cm of water until 3 – 4 cm

22
Not without its complications Do not take CPAP lightly! Pulmonary air leaks Excessive pressure- compromise o2 Abdominal distension Hypotension Local – excoriation, scarring, deformity

23
Setting an simple CPAP

24
To conclude Gentle & poor man’s ventilation Easy to set up & minimal training Save babies with RDS in developing countries vs headbox O2 Lots of unanswered questions yet – –Optimal device –Ideal pressure

Similar presentations



>")

>")






>")


 NICU Population Nursing Educational Series.>")

>")



