Download presentation
Presentation is loading. Please wait.

1
DIABETES AUTONOMIC NEUROPATHY MONICA MORENO MD ENDOCRINOLOGY AND DIABETES CLINIC IHC SAINT GEORGE UT SALT LAKE CITY NOVEMBER 2 2011

2
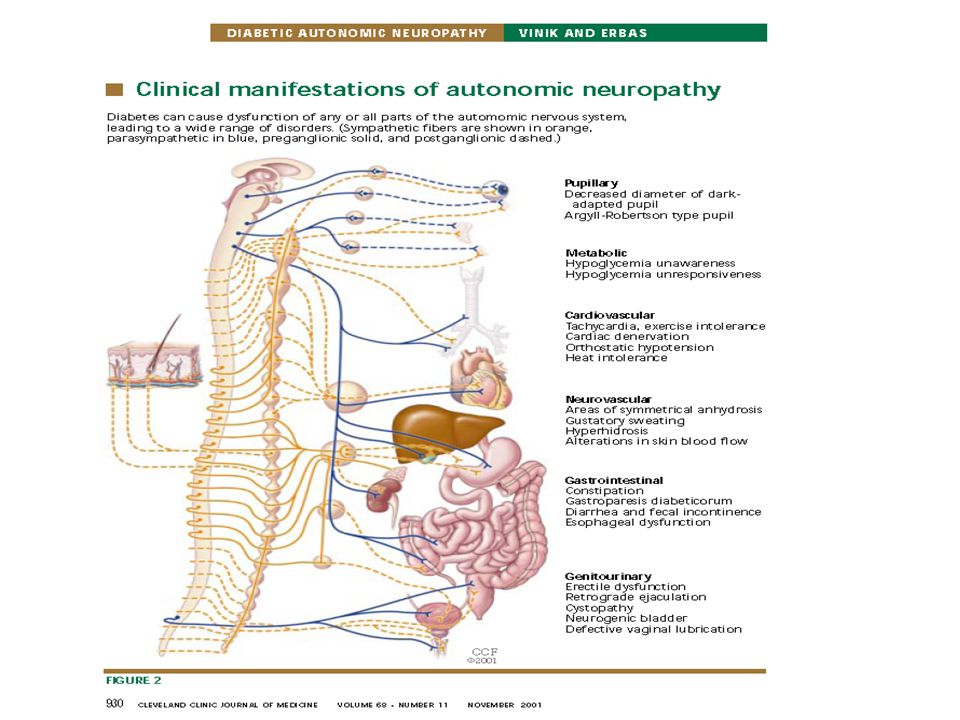
Objectives Identify the pathophysiologic mechanisms and clinical manifestations of diabetic autonomic neuropathy (DAN). Discuss and describe aspects of screening, prevention and education for patients at risk for DAN.

3
Diabetic Neuropathy Involvement of peripheral and autonomic nervous systems Most common complication of diabetes Underdiagnosed and Undertreated Substantial morbidity/mortality (CAN)
")
4
Diabetic neuropathy Distal symmetric polyneuropathy Focal Mononeuropathies Autonomic neuropathy Polyradiculopathies Mononeuropathy multiple

5
DIABETIC AUTONOMIC NEUROPATHY (DAN) Least recognized and understood complications of diabetes. Can involve the entire autonomic nervous system (ANS) May be either clinically evident or subclinical
 May be either clinically evident or subclinical.")
6
DAN: Incidence Panbianco et Al. The pittsburgh Epidemiology of Diabetes Complications Study experience

7
DAN: Prevalence Tesfaye et Al. Vascular Risk Factors and Diabetic Neuropathy. EURODIAB Prospective Complication Study Group NEJM 352;4 January 27, 2005

8
Pathophysiology Vinik A: Diabetic Neuropathy: Pathogenesis and Therapy. Am J Med 107 (2B):17S-26S, 1999
:17S-26S,")
9
DAN: Risk Factors Tesfaye et Al. Vascular Risk Factors and Diabetic Neuropathy. EURODIAB Prospective Complication Study Group NEJM 352;4 January 27, 2005

10
DAN: Risk Factors Tesfaye et Al. Vascular Risk Factors and Diabetic Neuropathy. EURODIAB Prospective Complication Study Group NEJM 352;4 January 27, 2005

11
Clinical Presentation Clinical symptoms generally do not appear until long after the onset of diabetes. However, subclinical autonomic dysfunction can occur within a year of diagnosis in type 2 diabetes patients and within two years in type 1 diabetes patients Pfeifer MA, Weinberg CR, Cook DL, Reenan A, Halter JB, Ensinck JW: Autonomic neural dysfunction in recently diagnosed diabetic subjects. Diabetes Care 7:447-453, 1984

12
Clinical Presentation Functional (e.g. gastroparesis with hyperglycemia and ketoacidosis) Organic (nerve fibers are actually lost) AN is not unique to diabetes: establish the diagnosis and exclude other causes. The best studied methods:evaluation of cardiovascular reflexes (can be easily done in clinic setting) This tests can be used as a surrogate for the diagnosis of AN of any system since it is generally rare to find involvement of any other division of the ANS in the absence of cardiovascular autonomic dysfunction
 Organic (nerve fibers are actually lost) AN is not unique to diabetes: establish the diagnosis and exclude other causes. The best studied methods:evaluation of cardiovascular reflexes (can be easily done in clinic setting) This tests can be used as a surrogate for the diagnosis of AN of any system since it is generally rare to find involvement of any other division of the ANS in the absence of cardiovascular autonomic dysfunction.")
14
Differential Diagnosis Idiopathic Orthostatic hypotension Panhypopituitarism Pheochromocytoma Amyloidosis Hypovolemia from diuretics SE from medications CHF Hypoglycemia due to intensive glycemic control.

15
CAN Most studied and clinically important Increased CV mortality damage to the autonomic nerve fibers that innervate the heart and blood vessels, resulting in abnormalities in heart rate control and vascular dynamics.4

17
Relative risks and 95% CIs for studies of cardiovascular neuropathy (CAN) and mortality. Maser R E et al. Dia Care 2003;26:1895-1901 Copyright © 2011 American Diabetes Association, Inc.

18
Effects of Cardiac Autonomic Dysfunction on Mortality Risk in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Trial. Pop-Busui R et al. Dia Care 2010;33:1578-1584

19
Central CAN 1.Tachycardia (HR >100 bpm) 2.Decreased exercise tolerance 3.Orthostasis (>20mmHg fall in systolic BP upon standing without compensationHR) 4.Cardiac denervation syndrome= SILENT MI 5.Paradoxic supine or nocturnal hypertension 6.Intraoperative and perioperative cardiovascular instability 7. Left ventricular diastolic dysfunction

20
Peripheral CAN 1.Decreased thermoregulation 2.Decreased sweating 3.Altered blood flow 4.Impaired vasomotion 5.Edema

21
Testing for CAN

23
METABOLIC 1.Hypoglycemia unawareness: decreased counterregulatory catecholamine responses 2.Hypoglycemia unresponsiveness: Reduction in glucagon and epinephrine secretion in response to Hypoglycemia

25
GI Esophageal dysmotility Gastroparesis diabeticorum (25%) Diarrhea (20% nocturnal diarrhea/fecal incontinence) Constipation (60%) Fecal incontinence
 Diarrhea (20% nocturnal diarrhea/fecal incontinence) Constipation (60%) Fecal incontinence")
26
GU Erectile dysfunction (50% at 10 years) Retrograde ejaculation Neurogenic bladder and cystopathy Female sexual dysfunction (20% loss of vaginal lubrication)
 Retrograde ejaculation Neurogenic bladder and cystopathy Female sexual dysfunction (20% loss of vaginal lubrication)")
27
Sudomotor Anhidrosis Hyperhidrosis Heat intolerance Gustatory sweating Dry skin

28
Pupillary 1.Pupillomotor function impairment (e.g., decreased diameter of dark adapted pupil) 2. Pseudo Argyll-Robertson pupil

29
DAN Screening ADA Guidelines 2011 At the time of diagnosis DM2 5 years after diagnosis DM1 Special testing rarely needed, may not affect management or outcomes

30
DAN Screening ADA Guidelines 2011 Increase risk of exercise induce injury or adverse event Patients should undergo cardiac investigation before intensifying physical activity

31
DAN Screening ADA Guidelines 2011 Comprehensive HPI Microvascular complications: – DPN – DAN (ED,gastroparesis, incontinence, recurrent infections, hypogycemia unawareness)
")
32
DAN Screening ADA Guidelines 2011 Signs: tachycardia, orthostatic hypotension, abnormal monofilament or VPT testing Test HR variability E:I ratio, valsalva maneuver, standing, EKG If normal repeat once a year

33
DAN treatment !!Prevention!! Once stablished: Improve glycemic control can slow progression but not reversal of neuronal loss if advanced at time of diagnoses. Symptomatic treatment: can improve quality of life of the patient.

36
DAN treatment Gaede et Al. Multifactorial Intervention and Cardiovascular disease in Patients with Type 2 Diabetes. Steno 2 Trial. N Engl J Med 2003;348:383-93

37
CAN Nuclear Stress test ACE I, BB, Antioxidants (Alpha-lipoic acid) Supportive garments for orthostatic hypotension Clonidine, fludrocortisone, midodrine, octreotide?
 Supportive garments for orthostatic hypotension Clonidine, fludrocortisone, midodrine, octreotide")
38
Gastroparesis Suspect if erratic glucose control or upper GI symptoms without other identified cause Gastric emptying study, barium study, Endoscopy : poorly correlation with symptoms. Diet, prokinetic agents, bulking agents

39
GU ED: therapy, phosphodiesterase type 5 inhibitors, intracorporeal or intraurethral prostaglandins, vacuum devices, or penile prostheses. Bladder: Postvoidal residual: bethanechol, intermitent catheterization

40
Hypoglycemia Avoidance of recurrent hypoglycemia Frequent FSBG testing or CMGS Individualized HgA1c goals

41
CGMS

Similar presentations























>")


