Download presentation
Presentation is loading. Please wait.

1
1.Pulmonary Vascular Disease 2.Pleural Disease Prof. Frank Carey

2
Pulmonary Circulatuion r Dual supply l Pulmonary arteries l Bronchial arteries r Low pressure system r Pulmonary artery receives entire cardiac output (a filter)
")
3
Low pressure system…. r Thin walled vessels r Low incidence of atherosclerosis At normal pressures

4
Pulmonary Oedema r Accumulation of fluid in the lung l Interstitium l Alveolar spaces r Causes a restrictive pattern of disease

5
Pulmonary Oedema (causes) 1. Haemodynamic ( hydrostatic pressure) 2. Due to cellular injury i. Alveolar lining cells ii. Alveolar endothelium Localised – pneumonia Generalised – adult respiratory distress syndrome (ARDS)
.")
6
ARDS r Diffuse alveolar damage syndrome (DADS) r Shock lung l Causes include sepsis, diffuse infection (virus, mycoplasma), severe trauma, oxygen
 r Shock lung l Causes include sepsis, diffuse infection (virus, mycoplasma), severe trauma, oxygen")
7
Pathogenesis of ARDS Injury (eg bacterial endotoxin) r Infiltration of inflammatory cells r Cytokines r Oxygen free radicals r Injury to cell membranes
 r Infiltration of inflammatory cells r Cytokines r Oxygen free radicals r Injury to cell membranes")
8
Pathology of ARDS r Fibrinous exudate lining alveolar walls (hyaline membranes) r Cellular regeneration r Inflammation
 r Cellular regeneration r Inflammation")
9
ARDS with hyaline membrane

10
ARDS – cellular reaction

11
Outcome of ARDS r Death r Resolution r Fibrosis (chronic restrictive lung disease

12
Neonatal RDS r Premature infants r Deficient in surfactant (type 2 alveolar lining cells r Increased effort in expanding lung physical damage to cells

13
Embolus r A detached intravascular mass carried by the blood to a site in the body distant from its point of origin r Most emboli are thrombi – others include gas, fat, foreign bodies and tumour clumps

14
Pulmonary Embolus r Common r Often subclinical r An important cause of sudden death and pulmonary hypertension 95% + of emboli are thromboemboli

16
Source of most pulmonary emboli….. r Deep venous thrombosis (DVT) of lower limbs
 of lower limbs")
20
Risk factors for PE are those for DVT…. 1. Factors in vessel wall (eg endothelial hypoxia) 2. Abnormal blood flow (venous stasis) 3. Hypercoaguable blood (cancer patients, post-MI etc) - Virchow’s triad
 3. Hypercoaguable blood (cancer patients, post-MI etc) - Virchow’s triad.")
21
Effects of PE r Sudden death r Severe chest pain/dyspnoea/haemoptysis r Pulmonary infarction r Pulmonary hypertension

22
Effects of PE depend on… r Size of embolus r Cardiac function r Respiratory function

23
Effect of embolus size… r Large emboli l Death l Infarction l Severe symptoms r Small emboli l Clinically silent l Recurrent pulmonary hypertension

25
Pulmonary Infarct (ischaemic necrosis) r Embolus necessary but not sufficient r Bronchial artery supply compromised (eg in cardiac failure)
 r Embolus necessary but not sufficient r Bronchial artery supply compromised (eg in cardiac failure)")
26
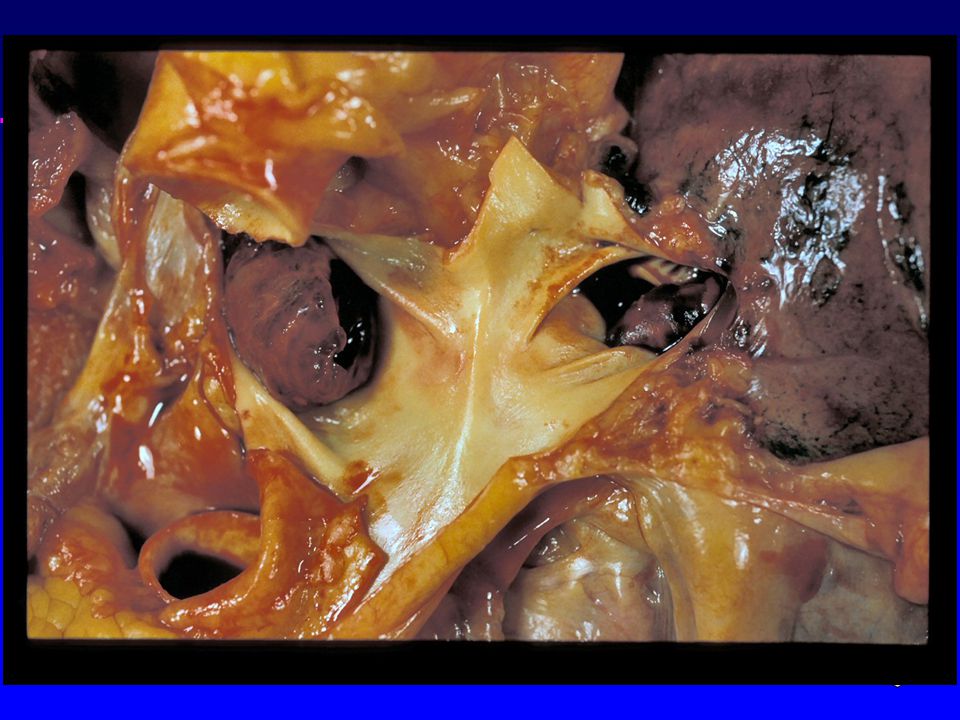
Pummonary Embolus

27
Pulmonary infarct – tumour embolus

28
Pulmonary Hypertension r Primary (rare, young women) r Secondary
 r Secondary")
29
Pulmonary Hypertension (mechanisms) r Hypoxia (vascular constriction) r Increased flow through pulmonary circulation (congenital heart disease) r Blockage (PE) or loss (emphysema) of pulmonary vascular bed r Back pressure from left sided heart failure
 r Hypoxia (vascular constriction) r Increased flow through pulmonary circulation (congenital heart disease) r Blockage (PE) or loss (emphysema) of pulmonary vascular bed r Back pressure from left sided heart failure")
30
Morphology of pulmonary hypertension r Medial hypertrophy of arteries r Intimal thickening (fibrosis) r Atheroma r Right ventricular hypertrophy r Extreme cases (congenital heart disease, primary pulmonary hypertension) – plexogenic change/necrosis
 r Atheroma r Right ventricular hypertrophy r Extreme cases (congenital heart disease, primary pulmonary hypertension) – plexogenic change/necrosis")
32
Pulmonary artery – intimal fibrosis

33
Plexiform lesion – primary pulmonary hypertension

34
“Cor Pulmonale” r Pulmonary hypertension complicating lung disease r Right ventricular hypertrophy r Right ventricular dilatation r Right heart failure (swollen legs, congested liver etc)
")
35
Cardiomegaly due to right ventricular dilatation

36
Right ventricular hypertrophy and dilatation

37
The Pleura r A mesothelial surface lining the lungs and mediastinum r Mesothelial cells designed for fluid absorption r Hallmark of disease is the effusion

38
Pleural Effusion r Transudate (low protein) l cardiac failure l hypoproteinaemia r Exudate (high protein) l pneumonia l TB l connective tissue disease l malignancy (primary or metastatic)
 l cardiac failure l hypoproteinaemia r Exudate (high protein) l pneumonia l TB l connective tissue disease l malignancy (primary or metastatic)")
39
Pleural effusion

40
Purulent Effusion Full of acute inflammatory cells r Empyema r Can become chronic

41
Pneumothorax Air in pleural space r Trauma r Rupture of bulla

42
Large bullae

43
Pleural Neoplasia r Primary l benign (rare) l malignant mesothelioma r Secondary l common (adenocarcinomas - lung, GIT, ovary)
 l malignant mesothelioma r Secondary l common (adenocarcinomas - lung, GIT, ovary)")
44
Mesothelioma r Asbestosis related r Increasing incidence r Mixed epithelial/mesenchymal differentiation r Dismal prognosis

45
Mesothelioma

46
Pleural biopsy - mesothelioma

47
Metastases in Pleura

48
Differential diagnosis of malignant effusions….. r Cytology, biopsy r Difficult r Immunohistochemistry for lineage specific antigens may help r Medicolegal importance

Similar presentations















 intracellular. (1/3)extracellular (interstitial fluid) 5% blood plasma. edema = an accumulation of interstitial.>")

 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")
, fibrous material and.>")











